

Abstract
Introduction
A fracture of the ceramic head in bipolar hemiarthroplasty using an inner polyliner has not been reported yet, and there seems to be no report of simultaneous breakage of the fourth-generation BIOLOX Delta ceramic head and liner in total hip arthroplasty.
Method
A 44-year-old male patient underwent bipolar hemiarthroplasty using a third-generation BIOLOX Forte ceramic head 3 years and 9 months earlier for osteonecrosis of femoral head (ONFH) and visited our hospital due to a ceramic head fracture. Conversion total hip arthroplasty was performed. A 64-year-old female patient underwent total hip arthroplasty using a fourth-generation BIOLOX Delta ceramic head and liner articulation for osteoarthritis of the hip. The ceramic head and liner were fractured during the third dislocation. Ceramic head and liner exchange revision surgery was performed.
Conclusion
When using ceramic bearings, fractures or delamination following trauma can occur, confirming the need to carefully evaluate the condition of the ceramic components in symptomatic patients.
Keywords: Arthroplasty, Hemiarthroplasty, Replacement, Hip, Ceramics
Introduction
Hip arthroplasty is said to be the operation of the century, and it will remain a dramatic treatment for hip diseases [1]. Hip replacement surgery shows the most stable and cost-effective long-term clinical outcomes [2]. However, there may be complications in hip replacement surgery. To improve the aseptic loosening, a disadvantage of conventional polyethylene, alternative bearings such as metal-on-metal, ceramic-on-ceramic and highly cross-linked polyethylene bearing were introduced in the early 1990 s [3]. Currently, combinations of joint surfaces are used for artificial joints, including metal-on-metal, ceramic-on-ceramic, ceramic-on-polyethylene, and metal-on-polyethylene [4, 5]. Since 1990s, ceramic-on-ceramic bearing has been used widely, especially in young active patients, because this hard-on-hard bearing has a low rate of wear and revision [4, 6]. However, squeaking and ceramic fracture appeared as complications of ceramic-on-ceramic bearings [7, 8].
These case reports describe very rare types of ceramic bearing fractures in bipolar hemiarthroplasty and total hip arthroplasty. In the first case, we describe the fracture of a BIOLOX Forte ceramic femoral head articulating with the polyethylene inner liner of hemiarthroplasty in a patient with a history of a two-meter traumatic fall. The second case describes a case in which BIOLOX Delta ceramic femoral head and liner fractures occurred simultaneously in total hip arthroplasty during reduction with recurrent dislocations.
To the best of our knowledge, there appears to be no previous reports of ceramic head fractures in hemiarthroplasty with an inner polyethylene liner. Five total hip arthroplasty cases were found that reported ceramic head fracture in ceramic-on-polyethylene bearings. Simultaneous ceramic head and liner fractures are also very rare. In the literature review, we were able to find only one case of both simultaneous ceramic head and liner fractures. However, this was a case report of the BIOLOX Forte ceramic rather than a report of simultaneous fracture of the BIOLOX Delta ceramic head and liner.
Case Presentation 1
A 44-year-old Asian male with a body mass index of 26.76 kg/m2 visited our hospital with left hip pain. Although there were no underlying diseases in his past medical history, he was chronic alcoholics and worked at a construction site. He underwent staged bilateral bipolar hemiarthroplasties for early stage of osteonecrosis of femoral head (ONFH) through a modified Gibson’s posterior approach at an outside hospital (Fig. 1). In the case of the left hip joint, surgery was performed using the following implant in 2018: A BIOLOX Forte (CeramTec, CeramTec-Platz, Plochingen, Germany) ceramic head with a polyethylene liner, and bipolar head cobalt-chromium-molybdenum casting alloy (Fig. 2). He recovered unharmed from his initial arthroplasty. There were no surgical wound problems or notable postoperative complications and the patient’s prognosis was generally considered good.
Fig. 1.

Early stage of osteonecrosis of femoral head (ONFH)
Fig. 2.

Bilateral bipolar hemiarthroplasties for early stage of osteonecrosis of femoral head
Three years and 9 months after the first surgery, this patient developed acute onset of traumatic hip pain caused by a fall while working and was admitted to the outpatient clinic for orthopedic evaluation. At the time of admission, a fracture of the ceramic head was diagnosed on radiographs and computed tomography (CT) of the pelvis and hip (Fig. 3). Physical examination of the left hip and lower extremities revealed a well-healed posterior surgical incision with pain-limited active and passive motion of the hip and prominent palpable crepitus. There were no abnormal findings on sensory and motor examination. He was diagnosed with a failed left bipolar hemiarthroplasty with a fracture of the ceramic head. The patient decided to emergency revision total hip arthroplasty, and the operation was performed the next day.
Fig. 3.

Radiographs and computed tomography (CT) of the pelvis and hip showing a fracture of the ceramic head
The hip was accessed through a modified Gibson’s posterior approach and the fractured ceramic head was removed. Several large fragments were contained within the polyethylene inner liner, as well as some smaller, comminuted pieces (Fig. 4). A complete synovectomy was done to remove as much ceramic debris as possible and to leave no potential source for third body wear. Damage to the original stem sleeve and trunnion damage was considered to be minimal. Therefore, a decision was made to perform conversion total hip arthroplasty while maintaining the existing stem. BIOLOX Delta (CeramTec, CeramTec-Platz, Plochingen, Germany) ceramic liner and one-step longer ceramic head (+ 8.5) were used to ensure more stability (Fig. 5). After confirming the excellent stability during the operation, the surgery was terminated, the patient awoke from anesthesia without any specific findings, and normal postoperative management was initiated. The patient stayed in the hospital for 14 days and was discharged home in good condition after confirming his safety by sufficient education on physical recovery treatment.
Fig. 4.

Ceramic head fracture in bipolar hemiarthroplasty
Fig. 5.
Postoperative radiograph showing conversion total hip arthroplasty
At his 1-year routine orthopedic follow-up, he had no symptoms and was almost normal in function. He had little pain and was able to walk long distances without the aid of a cane. His Harris Hip Score was 92.
Case Presentation 2
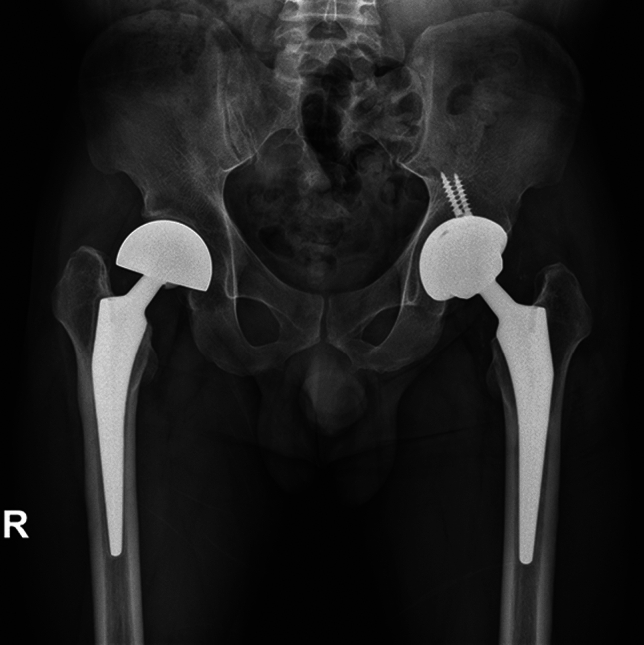
A 64-year-old Asian female with a body mass index of 33.20 kg/m2 visited our hospital with right hip pain. The patient had type II diabetes and hypertension as underlying diseases. She underwent staged bilateral total hip arthroplasties for primary hip arthritis through a modified Gibson’s approach at an outside hospital (Fig. 6). Her right side was operated on in 2014 with the following implants: BIOLOX Delta ceramic liner and a short neck ceramic head (Fig. 7). She recovered from the initial right total hip arthroplasty uneventfully. There were no wound problems or other postoperative complications related to the wound, and she was discharged with good progress and was under outpatient follow-up.
Fig. 6.

Right total hip arthroplasty for primary hip arthritis
Fig. 7.

Staged bilateral total hip arthroplasties for primary hip arthritis
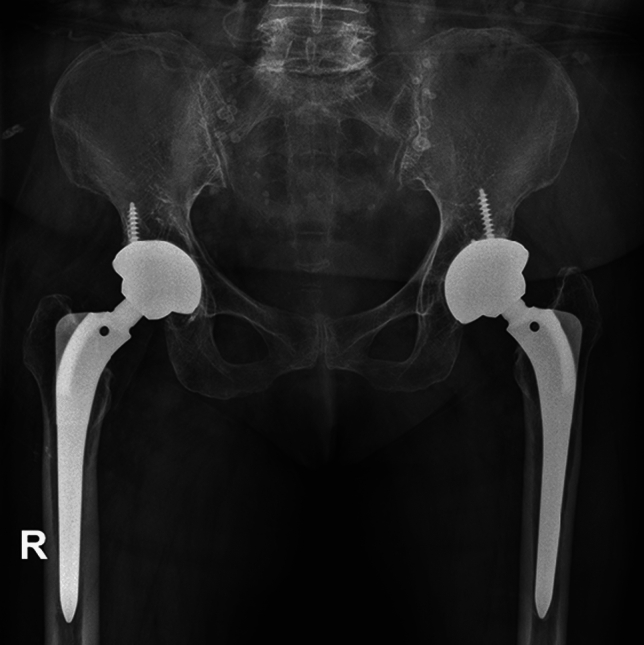
However, she experienced three dislocations as late postoperative complication. She had no major traumatic events, and the dislocations occurred during her daily activities. The first dislocation occurred 5 years after surgery, a second dislocation occurred two months later, and a third occurred 11 months after that. After the third dislocation, the patient was admitted to the emergency room of our hospital, and after orthopedic evaluation, she was diagnosed with ceramic head and liner fracture and needed revision surgery (Fig. 8).
Fig. 8.

Right hip radiographs and computed tomography (CT) taken in emergency room showing comminuted ceramic femoral head and liner fracture
The hip was operated using a modified Gibson’s posterior approach with the same access as the previous incision, revealing a fractured ceramic head and liner. There were several large fragments contained within the acetabular component and, a liner fracture was also observed. A total synovectomy was performed in an effort to remove as much ceramic debris and numerous smaller, comminuted fragments as possible (Fig. 9). Preoperative evaluation showed that the acetabular cup position appeared to have anteversion within acceptable range of 20.4 degrees and inclination of 37.8 degrees. The original stem sleeve and trunnion damage was also considered to be minimal and the decision was made to leave the acetabular component and original stem. BIOLOX Delta ceramic liner and a long neck ceramic head were used to ensure more stability (Fig. 10). Confirming the excellent stability, the surgery was terminated, the patient awoke from anesthesia without any specific findings, and normal postoperative care and ambulation was initiated. The patient was hospitalized for about 2 weeks, received proper walking and physical therapy, and was safely discharged after receiving sufficient education on precautions.
Fig. 9.

Clinical photographs of ceramic head and liner fracture after explant
Fig. 10.
Postoperative radiograph showing revision total hip arthroplasty and well-maintained implant
At her 1-year routine orthopedic follow-up, she had no symptoms and was almost normal in function. She had little to no pain and was able to walk moderate distances without a cane. Her Harris Hip Score was 90.
Discussion
The advantage of ceramic bearings include lower wear rates and fewer metal ions compared to polyethylene and metal bearings [5]. However, ceramic bearings have disadvantages in terms of squeaking, crack, and impingement [9]. Other issues, such as neck and stem-rim impingement and the mal-seating of ceramic liner, might accelerate wear and induce abnormal metal ion levels [10–12].
Ceramic head or liner fractures are one of the most serious complications and almost unconditionally require revision surgery. The fracture rate of ceramic bearing is known to be 0.5% in the forte group and 0.2% in the delta group [8]. In many cases, ceramic head or liner fractures have been reported in ceramic-on-ceramic bearings. This is because the ceramic-on-ceramic is a hard-on-hard bearing. Considering the effect of softness and shock absorption of the polyethylene liner, fracture of the ceramic component is considered less likely to occur and few reports appear in the literature (Table 1) [13–17]. However, attention should be paid to what is still happening, and even more attention should be paid because it was reported during revision [18]. The initiation of cracks on the surface of the alumina matrix by strong impact from acute trauma or repeated stress events on the implant may be the cause, as mentioned by Rankin et al. [17]. In order to achieve good results, one study recommended that the use of a shallow ceramic head with a short neck should be avoided [19]. In fact, in the present report, patients achieved excellent stability in revision arthroplasty using a ceramic head that was at least one or two steps thicker.
Table 1.
Summary of clinical data of ceramic head fracture with ceramic-on-polyethylene bearing or simultaneous ceramic head and liner fracture
| No | Author | Year | Sex/Age | THR-bearings | Etiology/mechanism of fracture | Treatment |
|---|---|---|---|---|---|---|
| 1 | Heiner et al. [13] | 2014 | F/45 | CoP | Bicycle accident/traumatic event | Revision to a CoP articulation with a same 36 mm sized ceramic head |
| 2 | Tucker et al. [14] | 2014 | M/68 | CoP | Atraumatic/no obvious mechanism | Revision to a CoC articulation with a 36 mm sized ceramic head |
| 3 | Pomeroy et al. [15] | 2015 | M/41 | CoP | Atraumatic/no obvious mechanism | Revision to a CoC articulation with a same 32 mm sized ceramic head |
| 4 | Rankin et al. [17] | 2019 | M/52 | CoP | Slipped and fell on the ice/traumatic event | Revision to a CoC articulation with a same 32 mm sized ceramic head |
| 5 | Valentini et al. [18] | 2020 | M/58 | CoP |
Trauma during skiing Traumatic event |
Revision to a CoP articulation with a same 36 mm sized ceramic head |
| 6 | Duensing et al. [16] | 2021 | M/83 | CoP | Atraumatic/no obvious mechanism | Revision to a CoP articulation with a same 40 mm sized ceramic head |
| 7 | Reategui et al. [28] | 2013 | M/35 | CoC | Atraumatic/no obvious mechanism | Revision to MoP articulation |
| 8 | Morlock et al. [26] | 2014 | M/29 | CoC | Ceramic liner mal-seating/ceramic liner fracture and head wear | Revision to a CoC articulation with a same 36 mm sized option ceramic head |
CoP ceramic-on-polyethylene, CoC ceramic-on-ceramic, MoP metal-on-polyethylene
The articular cartilage could play an essential role in shock absorption effects [20]. Cartilaginous sparing and the introduction of a high-density polyethylene liner might afford additional shock-absorbing effects in bipolar hemiarthroplasty (HA), even though this is only recommended for elderly patients and those with a lower predicted life expectancy [21]. For this reason, the shock-absorbing effect of a HA consisting of acetabular cartilage, outer metal cup, and inner polyethylene liner may be greater than the sum of the total hip arthroplasty (THA) hard components. However, ceramic head fractures even in HA appear to occur when the stress from a traumatic event immediately exceeds the ceramic burst strength threshold. Crack initiation and propagation can occur if the stress exceeds the tensile strength of the material.
Bipolar hemiarthroplasty could be a treatment for the early stage of osteonecrosis of femoral head (ONFH). Some reports have indicated that hemiarthroplasty showed good clinical results in the treatment of ONFH with intact acetabular cartilage [22, 23]. However, with respect to ONFH, the survival rate of HA was lower than that of THA, and the indication of HA is narrowing [24, 25]. Ceramic head fracture after HA has not been reported, and this report is considered to be the first in bipolar HA with a ceramic on polyethylene inner liner.
Simultaneous fractures of the BIOLOX Delta ceramic head and liner are considered to be very rare. It has been reported that inner liner fracture eventually leads to wear of the ceramic head [26]. This case demonstrates that a tilted ceramic liner can eventually lead to serious wear of ceramic head. Therefore, the position of the inner liner must be checked very carefully and impacted in the right location into the acetabular shell to achieve exact fixation. The introduction of fourth-generation ceramic composite materials (BIOLOX Delta; CeramTec, CeramTec-Platz, Plochingen, Germany) reduced the risk of ceramic fracture compared to third-generation alumina ceramics (BIOLOX Forte; CeramTec, CeramTec-Platz, Plochingen, Germany) (8). In this BIOLOX Delta, the mixture of zirconia and alumina particles exhibited excellent performances in terms of wear and limited crack propagation [27]. The combination of these two outstanding materials could reduce ceramic fracture and wear rate. Only one case of both ceramic head and liner fracture was found, and this was the case of a patient using the third-generation BIOLOX Forte ceramic head and liner (Table 1) [28]. There was no report of simultaneous fracture of the head and liner when the fourth-generation delta ceramic bearing was used.
Many studies showed ceramic bearings are clearly superior to other products because they have a lower wear rate compared to polyethylene and fewer metal ions compared to metal bearings. More research is being conducted to reduce major problems, such as ceramic breakage, noise generation, liner mal-seating, and collisions, and it can be said that the development potential is high. However, when using ceramic bearings, fractures can occur at any time, so the condition of ceramic components should be carefully evaluated in symptomatic patients, especially after traumatic events.
Conclusion
When using ceramic bearings, fractures or delamination following trauma can occur at any time, confirming the need to carefully evaluate the condition of the ceramic components in symptomatic patients.
Author contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis. All authors read and approved the final manuscript.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Ethics Approval
This research has been reviewed and approved by the Institutional Review Board (IRB) of the authors’ affiliated institutions (VC22ZISI0314).
Informed Consent, Data and Code Availability
Informed consent was obtained from all individual participants included in the study.
Footnotes
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Learmonth ID, Young C, Rorabeck C. The operation of the century: Total hip replacement. Lancet. 2007;370(9597):1508–1519. doi: 10.1016/S0140-6736(07)60457-7. [DOI] [PubMed] [Google Scholar]
- 2.Bourne RB, Maloney WJ, Wright JG. An AOA critical issue. The outcome of the outcomes movement. Journal of Bone and Joint Surgery. American Volume. 2004;86(3):633–640. doi: 10.2106/00004623-200403000-00026. [DOI] [PubMed] [Google Scholar]
- 3.Milosev I, Kovac S, Trebse R, Levasic V, Pisot V. Comparison of ten-year survivorship of hip prostheses with use of conventional polyethylene, metal-on-metal, or ceramic-on-ceramic bearings. Journal of Bone and Joint Surgery. American Volume. 2012;94(19):1756–1763. doi: 10.2106/JBJS.J.01858. [DOI] [PubMed] [Google Scholar]
- 4.Lee YK, Yoon BH, Choi YS, Jo WL, Ha YC, Koo KH. Metal on metal or ceramic on ceramic for cementless total hip arthroplasty: A meta-analysis. Journal of Arthroplasty. 2016;31(11):2637–2645. doi: 10.1016/j.arth.2016.04.014. [DOI] [PubMed] [Google Scholar]
- 5.Zheng C, Xu J, Wu L, Wu Y, Liu Y, Shen B. Comparisons of different bearing surfaces in cementless total hip arthroplasty: A systematic review and Bayesian network analysis. Journal of Arthroplasty. 2022 doi: 10.1016/j.arth.2022.10.016. [DOI] [PubMed] [Google Scholar]
- 6.Bozic KJ, Kurtz S, Lau E, Ong K, Chiu V, Vail TP, et al. The epidemiology of bearing surface usage in total hip arthroplasty in the United States. Journal of Bone and Joint Surgery. American Volume. 2009;91(7):1614–1620. doi: 10.2106/JBJS.H.01220. [DOI] [PubMed] [Google Scholar]
- 7.Stanat SJ, Capozzi JD. Squeaking in third- and fourth-generation ceramic-on-ceramic total hip arthroplasty: Meta-analysis and systematic review. Journal of Arthroplasty. 2012;27(3):445–453. doi: 10.1016/j.arth.2011.04.031. [DOI] [PubMed] [Google Scholar]
- 8.Yoon BH, Park JW, Cha YH, Won SH, Lee YK, Ha YC, et al. Incidence of ceramic fracture in contemporary ceramic-on-ceramic total hip arthroplasty: A Meta-analysis of proportions. Journal of Arthroplasty. 2020;35(5):1437–1443. doi: 10.1016/j.arth.2019.12.013. [DOI] [PubMed] [Google Scholar]
- 9.Migaud H, Putman S, Kern G, Isida R, Girard J, Ramdane N, et al. Do the reasons for ceramic-on-ceramic revisions differ from other bearings in total hip arthroplasty? Clinical Orthopaedics and Related Research. 2016;474(10):2190–2199. doi: 10.1007/s11999-016-4917-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Chung KY, Cheung KW, Fan CH, Poon WC, Chiu KH, Ho KK. Long-term outcome on the mal-seating of ceramic-on-ceramic articulation in total hip arthroplasty. Journal of Arthroplasty. 2021;36(6):2100–2104. doi: 10.1016/j.arth.2021.01.024. [DOI] [PubMed] [Google Scholar]
- 11.Ishida T, Tateiwa T, Takahashi Y, Takahashi RH, Sano K, Shishido T, et al. IL-17A-mediated immune-inflammatory periarticular mass and osteolysis from impingement in ceramic-on-ceramic total hip arthroplasty. Arthroplast Today. 2021;11:15–19. doi: 10.1016/j.artd.2021.06.018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Lee S, Yoo JJ, Kim HJ. Impingement between the metal stem and the ceramic liner in total hip arthroplasty: The neck is not the only place where impingement occurs. Journal of Bone and Joint Surgery. American Volume. 2021;103(2):139–145. doi: 10.2106/JBJS.20.00354. [DOI] [PubMed] [Google Scholar]
- 13.Heiner AD, Mahoney CR. Fracture of a BIOLOX delta ceramic femoral head articulating against a polyethylene liner: A case report. JBJS Case Connector. 2014;4(4):e97. doi: 10.2106/JBJS.CC.N.00040. [DOI] [PubMed] [Google Scholar]
- 14.Tucker D, Acharya M. Unusual prosthetic femoral head fracture in total hip arthroplasty: Ceramic on polyethylene articulation. BMJ Case Reports. 2014 doi: 10.1136/bcr-2013-202685. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Pomeroy E, Rowan F, Masterson E. Atraumatic fracture of a BIOLOX delta ceramic femoral head articulating with a polyethylene liner: A case report. JBJS Case Connector. 2015;5(4):e112. doi: 10.2106/JBJS.CC.O.00146. [DOI] [PubMed] [Google Scholar]
- 16.Duensing IM, Stanley S, Bolognesi M. Fracture of a 40-mm BIOLOX Delta Femoral Head. Arthroplast Today. 2021;10:144–148. doi: 10.1016/j.artd.2021.06.021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Rankin CS, Robinson PG, Beattie N, Gaston P. Fracture of a BIOLOX delta ceramic femoral head: A CAse report and update of the literature. JBJS Case Connector. 2019;9(4):e0336. doi: 10.2106/JBJS.CC.18.00336. [DOI] [PubMed] [Google Scholar]
- 18.Valentini R, Vacchiano A, Sandri A, Regis D, Dall'Oca C, Magnan B. Fourth generation head fracture in ceramic-on-polyethylene bearing after hip revision surgery: A case report. Acta Biomedica. 2020;91(4-S):248–253. doi: 10.23750/abm.v91i4-S.9499. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Kim HS, Park JW, Ha JH, Lee YK, Ha YC, Koo KH. Third-generation ceramic-on-ceramic total hip arthroplasty in patients with osteonecrosis of the femoral head: A 10- to 16-year follow-up study. Journal of Bone and Joint Surgery. American Volume. 2022;104(Suppl 2):68–75. doi: 10.2106/JBJS.20.00720. [DOI] [PubMed] [Google Scholar]
- 20.Shaktivesh, Malekipour F, Lee PVS. Shock absorbing ability in healthy and damaged cartilage-bone under high-rate compression. Journal of the Mechanical Behavior of Biomedical Materials. 2019;90:388–394. doi: 10.1016/j.jmbbm.2018.10.023. [DOI] [PubMed] [Google Scholar]
- 21.Lewis DP, Waever D, Thorninger R, Donnelly WJ. Hemiarthroplasty vs total hip arthroplasty for the management of displaced neck of femur fractures: A systematic review and meta-analysis. Journal of Arthroplasty. 2019;34(8):1837–43 e2. doi: 10.1016/j.arth.2019.03.070. [DOI] [PubMed] [Google Scholar]
- 22.Chan YS, Shih CH. Bipolar versus total hip arthroplasty for hip osteonecrosis in the same patient. Clinical Orthopaedics and Related Research. 2000;379:169–177. doi: 10.1097/00003086-200010000-00020. [DOI] [PubMed] [Google Scholar]
- 23.Nagai I, Takatori Y, Kuruta Y, Moro T, Karita T, Mabuchi A, et al. Nonself-centering Bateman bipolar endoprosthesis for nontraumatic osteonecrosis of the femoral head: A 12- to 18-year follow-up study. Journal of Orthopaedic Science. 2002;7(1):74–78. doi: 10.1007/s776-002-8422-8. [DOI] [PubMed] [Google Scholar]
- 24.Yun AG, Martin S, Zurakowski D, Scott R. Bipolar hemiarthroplasty in juvenile rheumatoid arthritis: Long-term survivorship and outcomes. Journal of Arthroplasty. 2002;17(8):978–986. doi: 10.1054/arth.2002.35799. [DOI] [PubMed] [Google Scholar]
- 25.Pellegrini VD, Jr, Heiges BA, Bixler B, Lehman EB, Davis CM., 3rd Minimum ten-year results of primary bipolar hip arthroplasty for degenerative arthritis of the hip. Journal of Bone and Joint Surgery American. 2006;88(8):1817–1825. doi: 10.2106/JBJS.01879.pp. [DOI] [PubMed] [Google Scholar]
- 26.Morlock MM, Witt F, Bishop N, Behn R, Dalla Pria P, Barrow R, et al. Wear of a composite ceramic head caused by liner fracture. Orthopedics. 2014;37(7):e653–e656. doi: 10.3928/01477447-20140626-63. [DOI] [PubMed] [Google Scholar]
- 27.Affatato S, Goldoni M, Testoni M, Toni A. Mixed oxides prosthetic ceramic ball heads. Part 3: Effect of the ZrO2 fraction on the wear of ceramic on ceramic hip joint prostheses. A long-term in vitro wear study. Biomaterials. 2001;22(7):717–723. doi: 10.1016/s0142-9612(00)00235-0. [DOI] [PubMed] [Google Scholar]
- 28.Reategui D, Garcia S, Bori G, Gallart X. Fracture of ceramic liner and head in a total hip arthroplasty with a sandwich type cup. Case Report in Orthopedics. 2013;2013:291691. doi: 10.1155/2013/291691. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Informed consent was obtained from all individual participants included in the study.