

Key Points
Question
What are the outcomes of treatment with neoadjuvant-intent cemiplimab or pembrolizumab for patients with locoregionally advanced cutaneous squamous cell carcinoma (cSCC) in a clinical setting?
Findings
In this cohort study of 27 patients with cSCC, the pathologic response rate was 47.4% (9 of 19 evaluable patients), and the radiologic response rate was 50.0% (8 of 16 evaluable patients).
Meaning
This study found that approximately half of patients with locoregionally advanced cSCC had a favorable response to preoperative immunotherapy, and clinical responders sometimes opted to forgo planned surgery.
Abstract
Importance
In clinical trials, preoperative immune checkpoint inhibitors (ICIs) have shown clinical activity in advanced cutaneous squamous cell carcinoma (cSCC). However, these studies excluded patients with relevant comorbidities.
Objective
To evaluate radiologic and pathologic response rates to neoadjuvant-intent programed cell death protein 1 (PD-1) ICIs in a clinical population.
Design, Setting, and Participants
This cohort study of patients who were treated with neoadjuvant cemiplimab or pembrolizumab for advanced cSCC from January 2018 to January 2023 was conducted at 2 academic institutions in Boston, Massachusetts. Median follow-up was 9.5 months (range, 1.2-40.5).
Exposures
Cemiplimab or pembrolizumab.
Main Outcomes and Measures
Primary outcomes were radiologic and pathologic response rates. Secondary outcomes were 1-year recurrence-free survival, progression-free survival, disease-specific survival, and overall survival.
Results
This cohort study included 27 patients (including 9 patients [33.3%] with a history of lymphoma). Most patients were male (18 of 27 [66.7%]), with a median age of 72 years (range, 53-87 years). Most primary tumors were located on the head/neck (21 of 27 [77.8%]). There were no unexpected delays in surgery. The median number of doses before surgery was 3.5 (range, 1.0-10.0). Five patients (18.5%) ultimately declined to undergo planned surgery due to clinical responses or stability, and 1 (3.7%) did not undergo surgery due to progressive disease. The overall pathologic response rate (pathological complete response [pCR] or major pathological response) was 47.4% (9 of 19), and the overall radiologic response rate (radiologic complete response or partial response) was 50.0% (8 of 16). The pCR rate (7 of 19 [36.8%]) was higher than the radiologic complete response rate (2 of 16 [12.5%]). The pCR rate among patients with cSCC and concomitant lymphoma was 25.0%. The 1-year recurrence-free survival rate was 90.9% (95% CI, 50.8%-98.7%), progression-free survival was 83.3% (95% CI, 27.3%-97.5%), disease-specific survival was 91.7% (95% CI, 53.9%-98.8%), and overall survival was 84.6% (95% CI, 51.2%-95.9%).
Conclusions and Relevance
The results of this cohort study support the reproducibility of neoadjuvant-intent immunotherapy for cSCC in the clinical setting, including for patients with a history of lymphoma. Outside of clinical trials, it is not infrequent for patients to opt out of surgery for regressing tumors. The inclusion of higher-risk patients and preference for nonsurgical treatment are 2 factors that might explain the numerically lower pathologic response rate in this institutional experience.
This cohort study examines treatment with neoadjuvant-intent cemiplimab or pembrolizumab for patients with locoregionally advanced cutaneous squamous cell carcinoma in a clinical setting.
Introduction
Cutaneous squamous cell carcinoma (cSCC) is the second most common nonmelanoma skin cancer after basal cell carcinoma, has a rising incidence, and accounts for approximately 20% of nonmelanoma skin cancers.1,2 The most important risk factor for cSCC is cumulative UV exposure.3,4 Other risk factors include older age and immunosuppression.5
Surgery with or without adjuvant radiation therapy (RT) has been the standard of treatment for cSCC for decades. However, it can have suboptimal functional and cosmetic outcomes, and the risk of recurrence is still substantial for high-risk subgroups.3 Advanced cSCC is a term used to describe tumors with local invasion, in-transit metastasis (ITM), nodal metastasis, or distant metastases and often cannot be cured by local therapies alone.6 It is a life-threatening condition and has been reported to be responsible for an estimated 3900 to 8700 US deaths in 1 year.2 Cemiplimab and pembrolizumab are high-affinity human monoclonal immune checkpoint inhibitor (ICI) antibodies against programmed cell death protein 1 (PD-1) that have been approved by the US Food and Drug Administration for treating locally advanced or metastatic cSCC in patients ineligible for curative surgery or RT.7,8
Recently, neoadjuvant cemiplimab has been shown to be highly effective for locoregionally advanced but resectable cSCC in immunocompetent patients. In a pilot study of 20 patients who received up to 2 doses of cemiplimab, a pathologic response rate of 70% was observed.3 Then, in a follow-up multisite study, 79 patients received up to 4 doses of cemiplimab, and 70 patients underwent surgery. The reported overall pathologic response rate was 63.3%, including 50.6% with complete pathologic response.9 Patients with concurrent immunosuppression, such as a hematologic cancer, were excluded from these trials; thus, there is a lack of data on neoadjuvant immunotherapy in these patients, who may have a decreased response to ICIs.10
The primary purpose of this study was to evaluate radiologic and pathological responses to neoadjuvant immunotherapy for advanced but resectable cSCC in a population that included relevant comorbidities at 2 tertiary care institutions. Secondary end points included safety, 1-year recurrence-free survival (RFS), disease-free survival (DFS), disease-specific survival (DSS), and overall survival (OS).
Methods
Study Design and Population
All patients who received neoadjuvant cemiplimab or pembrolizumab for advanced cSCC at 2 reference academic institutions from January 1, 2018, to January 13, 2023, were included in the study. The patient selection process is outlined in Figure 1. The Oncology Data Retrieval System and research patient data registry were used at both institutions to query for all patients who received cemiplimab or pembrolizumab for advanced cSCC (n = 289). Exclusion criteria included treatment with palliative immunotherapy for distant metastatic disease or unresectable local or regional tumors (n = 244); treatment with adjuvant-only immunotherapy (n = 3); participation in a clinical trial for neoadjuvant cemiplimab (n = 13); or nonevaluable status for pathologic and radiologic response (n = 2). Neoadjuvant-intent was defined as treatment with immunotherapy before planned surgery. This study was approved by the institutional review board of Mass General Brigham. Written consent was waived because the study was conducted as a retrospective health record review and involved no more than minimal risk.
Figure 1. Consort Diagram of the Patient Selection Process at 2 Academic Institutions.

Of 291 patients treated with an anti–programmed cell death 1 (PD-1) immune checkpoint inhibitor (ICI) for cutaneous squamous cell carcinoma (cSCC), 27 (9.3%) were ultimately included, 16 (59.3%) of whom were evaluable for radiologic response and 19 (70.4%) of whom were evaluable for pathologic response.
Treatment
All patients saw a surgeon in consultation and were intended to undergo planned surgery after 2 to 4 doses of upfront immunotherapy. Patients received at least 1 dose of cemiplimab administered intravenously at a dose of 350 mg every 3 weeks, or pembrolizumab administered intravenously at a dose of 200 mg every 3 weeks or 400 mg every 6 weeks. The exact timing between dosing may have slightly varied due to individual patient circumstances and the ability to adhere to a strict dosing regimen.
Outcomes
Using Response Evaluation Criteria in Solid Tumours (RECIST), version 1.1, investigators (A.W.S. and S.Z.S.) retrospectively assessed radiologic response for patients who had measurable disease on imaging results within 8 weeks before (median, 2.9 weeks; IQR, 1.8-4.6 weeks) and up to 6 months after ICI initiation. Radiologic responses were categorized as radiologic complete response (rCR; 100% decrease in the sum of target-lesion diameters), partial response (rPR; ≥30% decrease in the sum of target-lesion diameters), stable disease (rSD; neither rPR nor rPD), or progressive disease (rPD; ≥20% increase in the sum of target-lesion diameters).11 Patients who underwent surgery as planned after neoadjuvant ICI had pathologic responses reevaluated by a board-certified dermatopathologist and reported as percentage residual viable tumor (% RVT) and categorized as pathologic complete response (pCR; 0% RVT, absence of viable tumor cells in the surgical specimen), major pathologic response (MPR; 0% to ≤10% RVT), pathologic partial response (pPR; >10% but ≤50% RVT), and pathologic nonresponse (pNR; >50% RVT).12 Radiologic and pathologic responses were further evaluated in patients who had a codiagnosis of lymphoma compared with those who did not (eFigure 1 in Supplement 1) and in patients who reported inflammatory symptoms compared with those who did not (eFigure 2 in Supplement 1).
RFS for patients who received surgery was defined as the time interval between the date of surgery and date of recurrence and was censored at the last follow-up for patients who did not experience recurrence. Progression-free survival (PFS) for patients who did not receive surgery was defined as the time interval between initiation of immunotherapy and disease progression. DSS was defined as the time between the date of initiation of neoadjuvant immunotherapy and the date of death due to cSCC or cSCC-related causes. OS was defined as the time between the date of initiation of immunotherapy and date of death of any cause. Data for patients who did not experience any event were censored at the date of last follow-up.
Biomarker Analyses
A potential association between programmed cell death ligand 1 (PD-L1) expression and treatment response was explored. Immunohistochemical quantitative analysis for PD-L1 on the formalin-fixed, paraffin-embedded surgical specimens with at least 100 viable tumor cells was performed (rabbit monoclonal, Cell Signaling Technology; clone E1L3N) on the DAKO Link 48 platform (Agilent Technologies) and reported as a combined positive score (range, 0-100). For each case, the value was categorized as either PD-L1 negative (defined as PD-L1 expression in <1% tumor cells) or PD-L1 positive (defined as PD-L1 expression in ≥1% of tumor cells).
Results
Patients
Of 291 patients who were treated with anti–PD-1 ICIs (cemiplimab or pembrolizumab) for advanced cSCC between 2018 and 2023, 27 (9.3%) treated with neoadjuvant intent were included in our study (Figure 1). Patient, tumor, and treatment characteristics at the time of ICI initiation are outlined in Table 1. The median age was 72 years (range, 53-87 years). Ultimately, 27 patients who received at least 1 dose of cemiplimab or pembrolizumab with neoadjuvant intent as determined by the oncologists’ progress notes were included. Most patients were male (18 of 27 [66.7%]) and had an Eastern Cooperative Oncology Group performance status score of 1 (19 of 27 [70.4%]). Nine patients (33.3%) had a concomitant diagnosis of lymphoma, of whom 4 had active lymphoma and 5 had a history of lymphoma that was successfully treated with curative intent. Most primary tumors were located on the head and neck (21 of 27 [77.8%]). Most patients had T2b disease by the Brigham and Women’s Hospital staging system (15 of 27 [55.6%]) or T3 disease by the American Joint Committee on Cancer (AJCC) Staging Manual, eighth edition (10 of 27 [37.0%]).13 Most patients had overall stage 3 (13 of 27 [48.2%]) or M0 only stage 4 (12 of 27 [44.4%]) disease.13 Twenty patients (74.1%) had recurrent disease. Eight patients (29.6%) had a localized tumor only without ITM or nodal disease. Fifteen patients had nodal metastases (55.6%), and 7 had ITM (25.9%). Most of the patients with recurrence had previously undergone surgery for their tumors before recurrence (18 of 27 [66.7%]). Two patients (7.4%) had been previously treated with cisplatin and/or cetuximab for a separate primary cSCC. No patients had been previously treated with an ICI for cSCC. Twenty-two patients (81.5%) received cemiplimab, and 5 (18.5%) received pembrolizumab. The median number of doses before surgery was 3.5 (range, 1-10). The median length of follow-up, from initiation of ICI to the last visit before the data cutoff date, was 9.5 months (range, 1.2-40.5 months).
Table 1. Patient, Tumor, and Treatment Characteristics at Time of First Dose.
| Characteristic | No./total No. (%) |
|---|---|
| Age, median (range), y | 72 (53-87) |
| Female | 9/27 (33.3) |
| Male | 18/27 (66.7) |
| ECOG performance status | |
| 0 | 8/27 (29.6) |
| 1 | 19/27 (70.) |
| Hematologic cancer | 9/27 (33.3%) |
| Primary tumor location | |
| Head/neck | 21/27 (77.8) |
| Trunk/extremities | 6/27 (22.2) |
| Previous treatmenta | |
| Surgery | 18/27 (66.7) |
| Radiation | 7/27 (25.9) |
| Cisplatin or cetuximab (for different primary cSCC) | 2/27 (7.4) |
| None | 9/27 (33.3) |
| Staging group (AJCC 8) | |
| I | 1/27 (3.7) |
| II | 1/27 (3.7) |
| III | 13/27 (48.2) |
| IV | 12/27 (44.4) |
| Tumor stage (AJCC 8) | |
| TX | 3/27 (11.1) |
| T1 | 7/27 (25.9) |
| T2 | 5/27 (18.5) |
| T3 | 10/27 (37.0) |
| T4 | 2/27 (7.4) |
| Tumor stage (BWH) | |
| T1 | 2/27 (7.4) |
| T2a | 3/27 (11.1) |
| T2b | 15/27 (55.6) |
| T3 | 2/27 (7.4) |
| Not evaluable | 5/27 (18.5) |
| Node stage (AJCC 8) | |
| N0 | 12/27 (44.4) |
| N1 | 5/27 (18.5) |
| N2b | 5/27 (18.) |
| N3a | 1/27 (3.7) |
| N3b | 4/27 (14.8) |
| In-transit metastases | 7/27 (25.9) |
| Localized tumor only | 8/27 (29.6) |
| Recurrent disease | 20/27 (74.1) |
| Treatment | |
| Cemiplimab | 22/27 (81.5) |
| Pembrolizumab | 5/27 (18.5) |
Abbreviations: AJCC 8, American Joint Committee on Cancer Staging Manual, eighth edition; BWH, Brigham and Women’s Hospital tumor staging; cSCC, cutaneous squamous cell carcinoma; ECOG, Eastern Cooperative Oncology Group.
Numbers add to more than 100 because patients may contribute to more than 1 category.
Although all 27 patients were treated with neoadjuvant-intent ICI before planned surgery, 6 patients (22.2%) ultimately abstained from surgery; 5 (18.5%) of these were due to clinical response or stability, and 1 (3.7%) due to progressive disease that was no longer resectable. Of 21 patients (77.8%) who underwent planned surgery, 19 had pathologic responses reevaluated by a board-certified dermatopathologist. The remaining 2 patients who underwent surgery were pathologically nonevaluable: 1 patient received additional treatment with cetuximab after radiologic evaluation but before surgery due to progression while receiving a neoadjuvant-intent ICI, and the other initiated treatment with an ICI for 2 lesions, only 1 of which was excised due to the complete clinical response of the other. Of 21 patients who received surgery, 6 patients (28.5%) received postoperative RT only; 3 (14.3%) continued to receive immunotherapy only; 1 (4.8%) received postoperative immunotherapy, cetuximab, and RT; and 11 (52.4%) received observation only. All 6 patients who abstained from planned surgery were observed without RT after their last dose of ICI.
Outcomes
Twenty-seven patients received at least 1 cycle of neoadjuvant-intent cemiplimab or pembrolizumab. Twenty-five patients had a pre-ICI scan (computed tomography, positron emission/computed tomography, or magnetic resonance imaging), and 22 had a post-ICI scan. The median time to posttreatment scan after ICI initiation was 11.7 weeks (range, 5.0-20.4 weeks). Sixteen patients were evaluable for radiologic response. Two of these patients (12.5%) had rCR, 6 (37.5%) had rPR, 3 (18.7%) had rSD, and 5 (31.3%) had rPD for an overall radiologic objective response rate (rCR or rPR) of 50.0% (Figure 2).
Figure 2. Pathologic and Radiologic Responses in 27 Patients Who Received Neoadjuvant Cemiplimab or Pembrolizumab for Advanced but Resectable Cutaneous Squamous Cell Carcinoma.

The blue dashed lines indicate pathology-based criteria for complete response (pCR; 100% nonviable tumor), major pathologic response (MPR; ≥90% but <100% nonviable tumor), pathologic partial response (pPR; ≥50% but ≤90% nonviable tumor), and pathologic nonresponse (pNR; <50% nonviable tumor). The black dashed lines indicate imaging-based criteria for radiologic complete response (rCR; 100% decrease in the sum of target-lesion diameters), partial response (rPR; ≥30% decrease in the sum of target-lesion diameters), stable disease (rSD; neither rPR nor rPD), or progressive disease (rPD; ≥20% increase in the sum of target-lesion diameters) per RECIST, version 1.1.
aPatients who declined planned surgery due to clinical response or stability.
bOne patient who had progressive disease precluding surgery.
c0% Nonviable tumor (pNR) on pathologic evaluation.
Ultimately, 19 patients were evaluable for pathologic response. Of these, 7 patients (36.8%) had pCR, 2 (10.5%) had MPR, and 10 (52.6%) had pNR (Figure 2). Pathologic and radiologic responses are summarized in Table 2. No unexpected delays in surgery occurred, with a median (IQR) of 20 (14-29) days from last ICI dose to surgery. All reported adverse effects were as expected for treatment with anti–PD-1 immunotherapy, and no patients discontinued therapy due to adverse effects.
Table 2. Radiologic and Pathologic Tumor Response to Neoadjuvant Cemiplimab or Pembrolizumab.
| Response | No./total No. (%) |
|---|---|
| Radiologic | |
| Complete response: disappearance of all target lesions | 2/16 (12.5) |
| rPR: ≥30% decrease in sum of longest diameter of target lesions | 6/16 (37.5) |
| Stable disease: neither rPR nor rPD | 3/16 (18.7) |
| rPD: ≥20% increase in sum of longest diameters of target lesions | 5/16 (31.3) |
| Not evaluable | 11/27 (40.7) |
| Pathologic | |
| Pathologic complete response: absence of RVT | 7/19 (36.8) |
| Pathologic major response: ≤10% RVT | 2/19 (10.5) |
| Pathologic nonresponse: >50% RVT | 10/19 (52.6) |
| Not evaluable | 8/27 (29.6) |
Abbreviations: rPD, progressive disease; rPR, partial response; RVT, residual viable tumor.
Of the 4 patients with active lymphoma at the time of treatment, 1 had a pCR and 3 had pNR, for a pathological response rate of 25%. Of 5 patients with inactive lymphoma at the time of treatment, 4 were pathologically evaluable. Among these 4 patients, the pathologic response rate was 50% (1 pCR and 1 MPR) (eFigure 1 in Supplement 1). Among patients without comorbid lymphoma, 11 patients had pathologic evaluations, and 5 (45.5%) had pCR, 1 (9.0%) had MPR, and 5 (45.5%) had pNR, for an overall pathologic response rate of 6 of 11 (54.5%).
Clinical courses for all patients are depicted in Figure 3. At 12 months, the RFS rate was 90.9% (95% CI, 50.8%-98.7%), the PFS rate was 83.3 (95% CI, 27.3-97.5), the DSS rate was 91.7% (95% CI, 53.9%-98.8%), and the OS rate was 84.6% (95% CI, 51.2%-95.9%).
Figure 3. Clinical Courses for 27 Patients Who Received Neoadjuvant Cemiplimab or Pembrolizumab for Locoregionally Advanced but Resectable Cutaneous Squamous Cell Carcinoma.
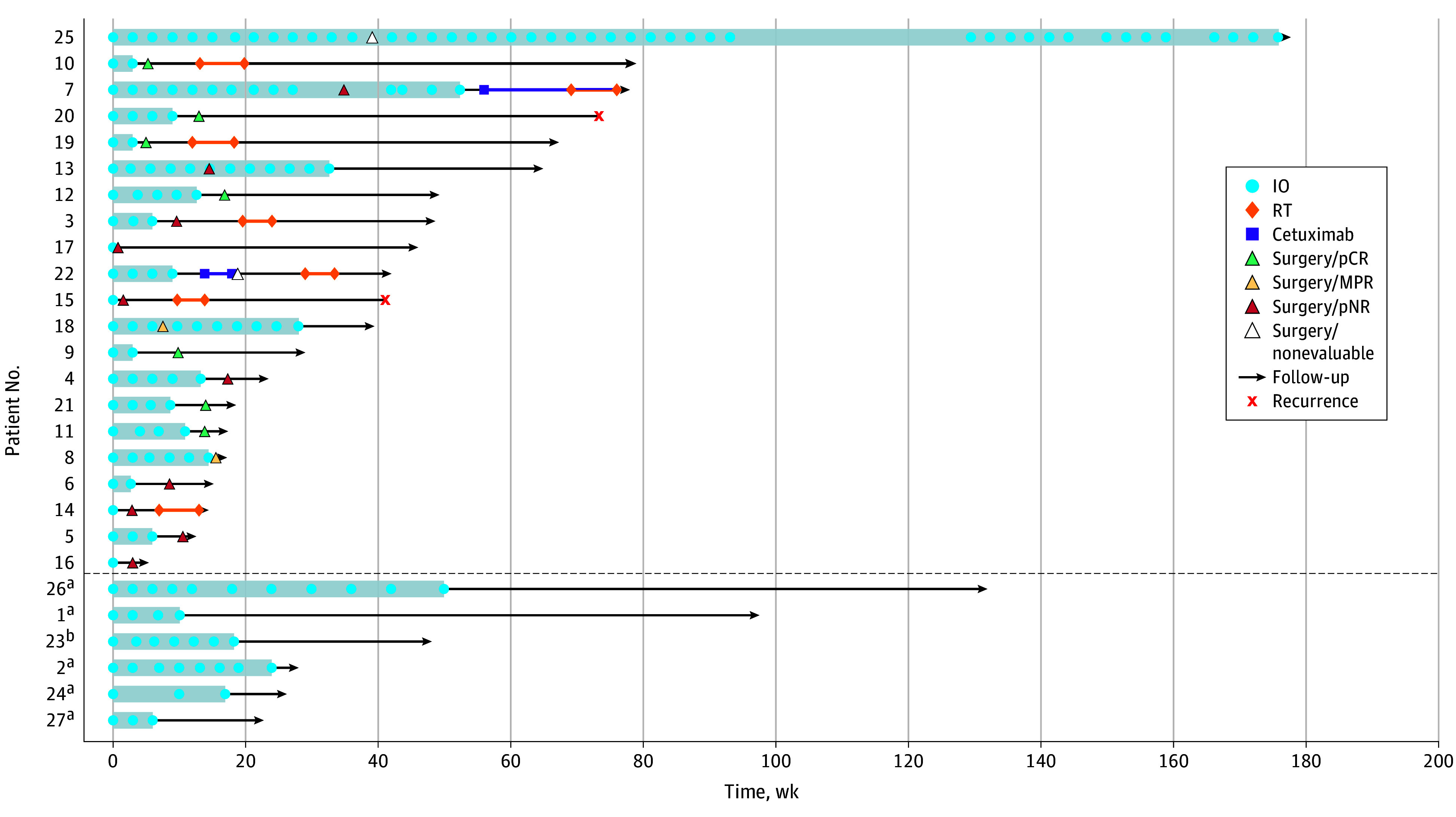
MPR indicates major pathologic response; pCR, pathologic complete response; pNR, pathologic nonresponse; RT, radiotherapy.
aPatients who declined planned surgery due to clinical response or stability.
bOne patient who had progressive disease precluding surgery. The dotted line separates patients who did not undergo surgery (below line) from patients who did undergo surgery (above line).
Clinical and Tumor-Based Biomarkers
Ten of 27 patients (37.0%) contacted their clinician to report inflammatory symptoms of redness, swelling, warmth, pain, and/or discomfort at the tumor site within the first 1 to 10 days after the first dose of immunotherapy that subsequently resolved without steroids. Among patients with self-reported inflammation at the tumor site, 3 of 7 evaluable patients (42.8%) had an objective radiologic response, and 5 of 9 evaluable patients (55.5%) had an objective pathologic response. Overall, 7 of 10 patients (70%) had either a radiologic and/or a pathologic response (eFigure 2 in Supplement 1). Ten patients had samples that could be assessed for PD-L1 combined positive score, 9 of whom had PD-L1 expression in 1% or more of tumor cells, and 1 who was negative for PD-L1 expression; thus, the potential association with PD-L1 expression and treatment response could not be analyzed.
Discussion
In our institutional experience, approximately half of patients with advanced but resectable cSCC had a favorable response to neoadjuvant PD-1 ICI. This supports previous observations in the literature that radiologic response underestimates pathologic response.3,9,14 While most patients who had pNR had disease progression on imaging, 2 patients with pNR did have an apparent radiologic response, suggesting that the current radiologic response evaluation system may not be optimal for capturing treatment response in this setting.
Overall, the pathologic response rate reported in this article was numerically lower than those reported in clinical trials; 2 phase 2 studies reported overall pathologic response rates of 63.3% and 70.0% in immunocompetent patients receiving neoadjuvant immunotherapy for advanced cSCC.3,9 The patients in our study presented with advanced disease and represent a higher-risk population. Before treatment initiation, 55.6% of patients had nodal involvement, and 25.9% had ITM. The presence of ITM has been shown to be a poor prognostic factor, with DSS outcomes equivalent to that of nodal or distant metastases.6 Second, a third of the patients in the data presented in this article would have been excluded from prior clinical trials for neoadjuvant immunotherapy due to history of active or previously treated lymphoma, which may help account for discrepancies in treatment response.10 Additionally, of 4 patients who received only 1 dose of ICI, all had pNR, suggesting that more than 1 dose is likely required for a response. Finally, we included all patients treated with neoadjuvant-intent immunotherapy to determine the surgical opt-out rate and the reasons why patients did not undergo surgery. The pathologic outcomes of patients who opted out of surgery were censored, which was associated with a decrease in the pathologic response rate.
In the multisite study, only 4 of 79 patients (5.0%) forwent surgery due to favorable clinical response.9 In contrast, in our institutional experience, 5 of 27 patients (18.5%) ultimately abstained from planned surgery due to clinical response or stable disease. This surgical opt-out rate was similar to that reported in the MATISSE trial, in which 9 of 50 patients (18.0%) declined planned surgery.15 Notably, all patients in the MATISSE trial who declined surgery were cancer free at a median follow-up of 12 months (range, 4-27) with superior quality of life measures compared with those receiving the planned trial intervention.15 In our cohort, the age of patients who rejected surgery was older, with a median age of 84 (range, 72-89 years), compared with the median age of 72 (range, 53-87 years) of the entire cohort. This age difference may reflect a group who prefers to live with controlled disease rather than undergo an operation. These results support the observation that response rates to ICIs may be low in patients with a history of hematologic cancer, particularly for patients with active lymphoma, which has implications for exclusion criteria for future clinical trials.10
In this study cohort, 2 patients developed a recurrence after surgery. Both had stage IV disease with ITM before treatment initiation. One patient had pNR and received postoperative RT. The other had pCR but underwent postoperative observation only; notably, they had active lymphoma at the time of treatment. Recurrence after a pathologic response seems to be rare, as recent long-term data from pilot trials suggest that pathologic response is a surrogate end point for long-term outcomes in cSCC.16,17 The first pilot study reported that none of the 15 patients who had a response (pCR or MPR) had a recurrence at a median follow-up of 42.3 months.16 The multicenter phase 2 trial reported that none of 40 patients who had a pCR and 1 of 10 patients (10%) with MPR had recurrence at a median follow-up of 18.7 months. There was heterogeneity in the postoperative management of participants in these trials, which confounds the interpretation of the reported long-term outcomes.
Responses were frequent among the patients who contacted the clinic to report mild to moderate tumor inflammation symptoms during the days following the initiation of immunotherapy. Seven of the 10 patients achieved pathologic and/or radiographic responses, suggesting that an inflammatory reaction at the tumor site early in treatment initiation may portend a favorable response. These temporary symptoms (pain, redness, and swelling) were treated with supportive care only (analgesics and ice). Clinicians should counsel patients that symptoms from tumor inflammation after the first infusion are common and generally resolve within a few days.
Limitations
Limitations to this study included the small sample size, patients based in a geographically limited area, and relatively short median follow-up period. Because this study presented results from clinical practice, inherent limitations include the absence of randomization, a control group, and uniform assessment with pre-ICI and post-ICI scans across all patients. Additionally, all patients included were referred to the medical oncology department at a tertiary care center due to the complexity of their cases; thus, referral bias may be a factor that was associated with our clinical outcomes. While optional adjuvant RT or continued immunotherapy was administered based on the treating physician’s discretion, this study did not aim to assess adjuvant treatment outcomes. The plurality of patients who had pNR were treated with postoperative RT. Most patients did not receive postoperative immunotherapy.
Conclusions
In this cohort study, the data in the neoadjuvant-intent setting support the existing literature but highlight lower responses in patients with relevant comorbidities, such as active lymphoma. In addition, our observations add to the existing literature by providing insights into patient selection, interpretation of inflammatory symptoms at the tumor site, and patient preference regarding the avoidance of surgery. Larger studies with longer follow-up periods are needed to guide key decisions, such as duration of preoperative ICI treatment, the role of early reimaging while receiving treatment with ICIs, choice of response-adapted surgical margins, and adoption of response-adapted indications for postoperative RT.
eFigure 1. Waterfall plot depicting pathologic and radiologic responses to neoadjuvant-intent cemiplimab or pembrolizumab for advanced cSCC in patients with concurrent active or inactive lymphoma, or no history of lymphoma
eFigure 2. Waterfall plot depicting pathologic and radiologic responses to neoadjuvant-intent cemiplimab or pembrolizumab for cSCC in patients who reported inflammatory symptoms after starting treatment compared to those who did not
Data sharing statement
References
- 1.Rogers HW, Weinstock MA, Feldman SR, Coldiron BM. Incidence estimate of nonmelanoma skin cancer (keratinocyte carcinomas) in the US population, 2012. JAMA Dermatol. 2015;151(10):1081-1086. doi: 10.1001/jamadermatol.2015.1187 [DOI] [PubMed] [Google Scholar]
- 2.Karia PS, Han J, Schmults CD. Cutaneous squamous cell carcinoma: estimated incidence of disease, nodal metastasis, and deaths from disease in the United States, 2012. J Am Acad Dermatol. 2013;68(6):957-966. doi: 10.1016/j.jaad.2012.11.037 [DOI] [PubMed] [Google Scholar]
- 3.Ferrarotto R, Amit M, Nagarajan P, et al. Pilot phase II trial of neoadjuvant immunotherapy in locoregionally advanced, resectable cutaneous squamous cell carcinoma of the head and neck. Clin Cancer Res. 2021;27(16):4557-4565. doi: 10.1158/1078-0432.CCR-21-0585 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Armstrong BK, Kricker A. The epidemiology of UV induced skin cancer. J Photochem Photobiol B. 2001;63(1-3):8-18. doi: 10.1016/S1011-1344(01)00198-1 [DOI] [PubMed] [Google Scholar]
- 5.Alam M, Ratner D. Cutaneous squamous-cell carcinoma. N Engl J Med. 2001;344(13):975-983. doi: 10.1056/NEJM200103293441306 [DOI] [PubMed] [Google Scholar]
- 6.Smile TD, Ruiz ES, Kus KJB, et al. Implications of satellitosis or in-transit metastasis in cutaneous squamous cell carcinoma: a prognostic omission in cancer staging systems. JAMA Dermatol. 2022;158(4):390-394. doi: 10.1001/jamadermatol.2022.0001 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.US Food and Drug Administration . FDA approves cemiplimab-rwlc for metastatic or locally advanced cutaneous squamous cell carcinoma. Accessed February 23, 2023. https://www.fda.gov/drugs/drug-approvals-and-databases/fda-approves-cemiplimab-rwlc-metastatic-or-locally-advanced-cutaneous-squamous-cell-carcinoma
- 8.US Food and Drug Administration . FDA approves pembrolizumab for cutaneous squamous cell carcinoma. FDA. Accessed September 23, 2022. https://www.fda.gov/drugs/drug-approvals-and-databases/fda-approves-pembrolizumab-cutaneous-squamous-cell-carcinoma
- 9.Gross ND, Miller DM, Khushalani NI, et al. Neoadjuvant cemiplimab for stage II to IV cutaneous squamous-cell carcinoma. N Engl J Med. 2022;387(17):1557-1568. doi: 10.1056/NEJMoa2209813 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Leiter U, Loquai C, Reinhardt L, et al. Immune checkpoint inhibition therapy for advanced skin cancer in patients with concomitant hematological malignancy: a retrospective multicenter DeCOG study of 84 patients. J Immunother Cancer. 2020;8(2):e000897. doi: 10.1136/jitc-2020-000897 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Eisenhauer EA, Therasse P, Bogaerts J, et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer Oxf Engl 1990. 2009;45(2):228-247. doi: 10.1016/j.ejca.2008.10.026 [DOI] [PubMed] [Google Scholar]
- 12.Stein JE, Lipson EJ, Cottrell TR, et al. Pan-tumor pathologic scoring of response to PD-(L)1 blockade. Clin Cancer Res. 2020;26(3):545-551. doi: 10.1158/1078-0432.CCR-19-2379 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Amin MB, Edge S, Greene F, et al. , eds. AJCC cancer staging manual (8th edition). Accessed July 14, 2023. https://link.springer.com/book/9783319406176
- 14.Menzies AM, Amaria RN, Rozeman EA, et al. Pathological response and survival with neoadjuvant therapy in melanoma: a pooled analysis from the International Neoadjuvant Melanoma Consortium (INMC). Nat Med. 2021;27(2):301-309. doi: 10.1038/s41591-020-01188-3 [DOI] [PubMed] [Google Scholar]
- 15.Breukers S, Machuca-Ostos M, Boere T, et al. Towards organ preservation and cure via 2 infusions of immunotherapy only, in patients normally undergoing extensive and mutilating curative surgery for cutaneous squamous cell carcinoma: an investigator-initiated randomized phase II trial—The MATISSE trial. J Clin Oncol. Published online May 31, 2023 doi: 10.1200/JCO.2023.41.16_suppl.9507 [DOI] [Google Scholar]
- 16.Ferrarotto R, Nagarajan P, Maronge JM, et al. Outcomes of treatment with neoadjuvant cemiplimab for patients with advanced, resectable cutaneous squamous cell carcinoma of the head and neck: secondary analysis of a phase 2 clinical trial. JAMA Otolaryngol Head Neck Surg. 2023;149(9):847-849. doi: 10.1001/jamaoto.2023.1729 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Gross ND, Miller DM, Khushalani NI, et al. Neoadjuvant cemiplimab and surgery for stage II-IV cutaneous squamous-cell carcinoma: follow-up and survival outcomes of a single-arm, multicentre, phase 2 study. Lancet Oncol. 2023;24(11):1196-1205. doi: 10.1016/S1470-2045(23)00459-X [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
eFigure 1. Waterfall plot depicting pathologic and radiologic responses to neoadjuvant-intent cemiplimab or pembrolizumab for advanced cSCC in patients with concurrent active or inactive lymphoma, or no history of lymphoma
eFigure 2. Waterfall plot depicting pathologic and radiologic responses to neoadjuvant-intent cemiplimab or pembrolizumab for cSCC in patients who reported inflammatory symptoms after starting treatment compared to those who did not
Data sharing statement