
Figure 2.
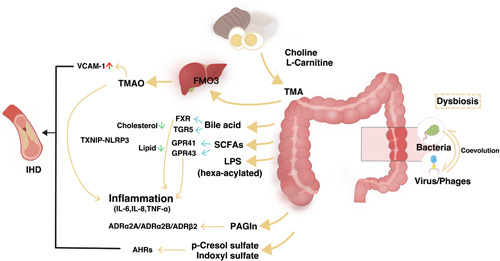
Gut‐heart axis: the potential mechanisms. An overview of some of the microbially produced compounds affecting the well‐being of cardiometabolic homeostasis during the dysbiosis associated with ischemic heart disease (IHD). Dietary l‐carnitine is metabolized by gut microbiota producing trimethylamine (TMA), which is subsequently N‐oxidized by liver flavin‐containing monooxygenases (FMOs) and producing trimethylamine N‐oxide (TMAO). TMAO has been recognized as an important contributor to atherosclerotic consequences. Secondary bile acids (BAs), synthesized from primary BAs by the intestinal microbiota, act through farnesoid X receptor (FXR) and Takeda G‐protein‐coupled receptor‐5 (TGR5) (also known as G protein‐coupled BA receptor 1 [Gpbar1]) receptors to reduce inflammation, thereby counteracting atherosclerosis. Short‐chain fatty acids (SCFAs) produced by gut microbiota through G‐protein receptor (GPR) 41/43 regulating systematic inflammation. Lipopolysaccharides (LPS), a class of pro‐inflammatory compounds, act on Toll‐like receptors, thereby activating atherosclerogenesis. Adrenoceptors have been identified as binding receptors for microbiota‐synthesized phenylacetylglutamine (PAGln). The Aryl hydrocarbon receptors (AHRs) plays crucial roles in mediating impact of two uremic toxins, p‐cresol sulfate and indoxyl sulfate, on cardiovascular system. IL, interleukin; NLRP3, NLR family pyrin domain containing 3; TNF‐α, tumor necrosis factor‐α; TXNIP, thioredoxin interacting protein; VCAM‐1, vascular cell adhesion molecule 1.