
Figure 2.
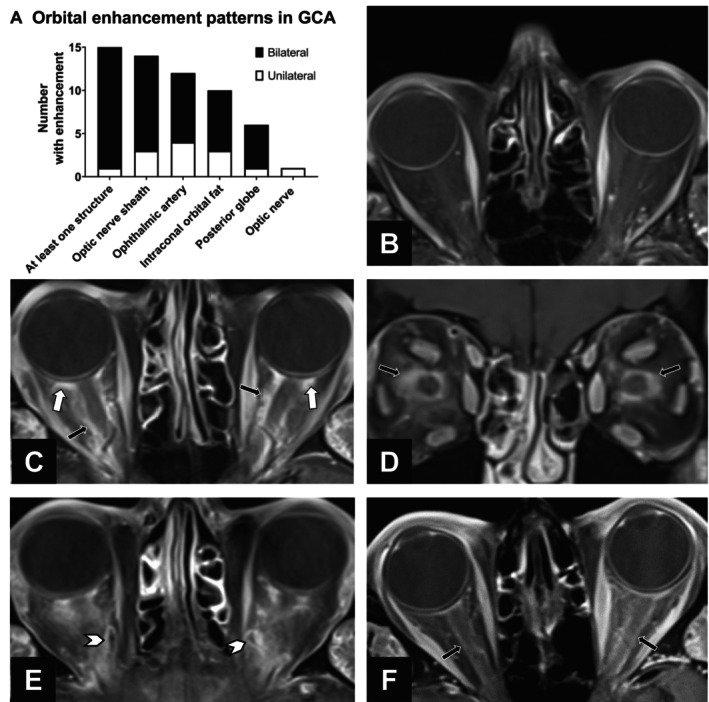
Orbital MRI enhancement in GCA. (A) Stacked bar graph of orbital structures with MRI enhancement among the 25 participants with a final clinical diagnosis of GCA. Enhancement was bilateral in a majority of cases. (B–E) Example MRIs of orbital enhancement using combined orbital and vessel wall MRI. All images are on an axial plane unless otherwise indicated. (B) Normal orbits in a patient without GCA and no visual symptoms. (C) Axial and (D) coronal images demonstrating bilateral enhancement of the optic nerve sheath and intraconal orbital fat (black arrows) and retrobulbar fat at the posterior globe (white arrows) in a patient diagnosed with GCA‐related arteritic ischemic optic neuropathy who had a positive temporal artery biopsy finding. (E) Ophthalmic vessel wall enhancement bilaterally (arrow heads) in a patient with GCA. (F) Bilateral MRI enhancement of optic nerve sheath (black arrows) in a patient with GCA. The patient presented with two weeks of diplopia, which was attributed to cranial nerve palsy, and had normal visual fields and funduscopic examination results. GCA, giant cell arteritis; MRI, magnetic resonance imaging.