
Fig. 1.
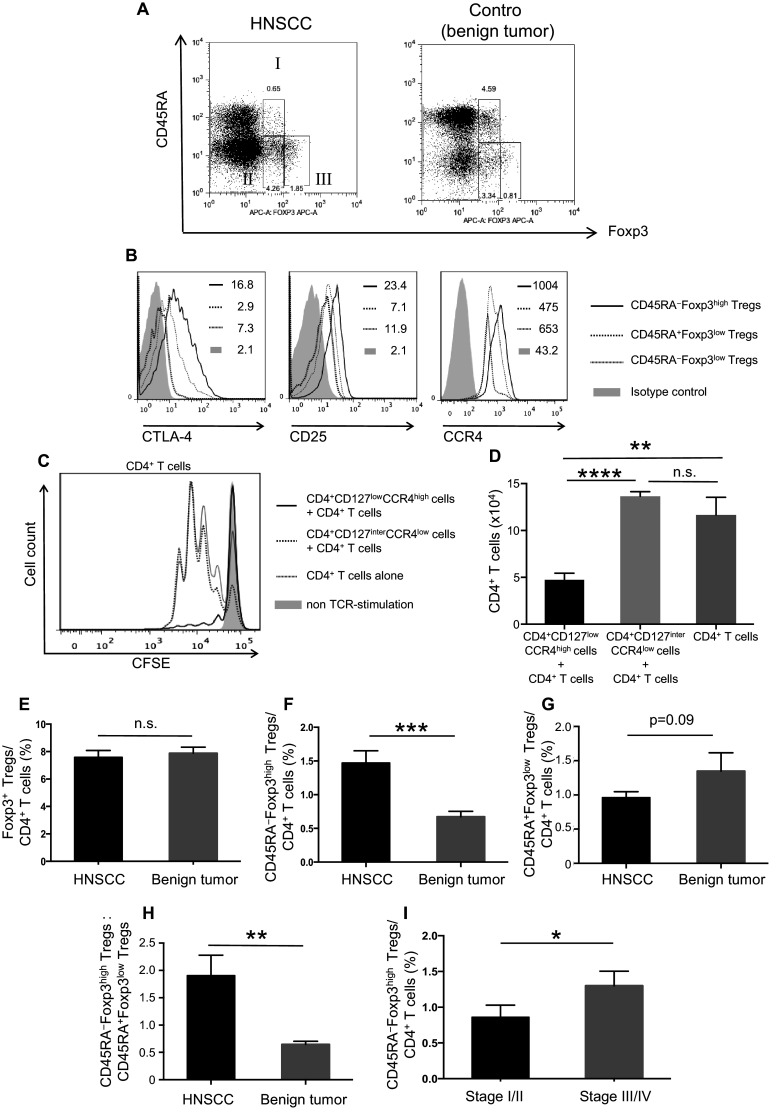
Frequency and characteristics of Treg subsets in patients with HNSCC and in those with benign tumors. The gating strategies for Treg subsets in the PBMCs of patients with HNSCC or benign tumors. I: CD45RA+Foxp3low, II: CD45RA−Foxp3low, and III: CD45RA−Foxp3high (a). The expression of CTLA-4, CD25, and CCR4 on Treg subsets in a representative patient with HNSCC (b). Mean fluorescence intensities (MFI) are indicated in the upper right quadrant. CFSE dilutions of proliferated CD4+ T cells were assessed after 72 h of TCR stimulation with or without indicated Treg subsets at a 1:1 ratio (c), and the number of proliferated CD4+ T cells after the co-culture are shown (d). The percentage of Foxp3+ cells in CD4+ T cells (e), CD45RA−Foxp3high Tregs in CD4+ T cells (F), CD45RA+Foxp3low Tregs in CD4+ T cells (g) and the ratio of CD45RA−Foxp3high Tregs to CD45RA+Foxp3low Tregs (h) in PBMCs of patients with HNSCC (n = 46) and benign tumors (n = 23) before treatment. The percentage of CD45RA−Foxp3high Tregs and the ratio of CD45RA−Foxp3high Tregs to CD45RA+Foxp3low Tregs were increased according to clinical stage (i). Statistical comparisons were performed using the parametric unpaired t test. *p < 0.05, **p < 0.01, ***p < 0.001, ****p < 0.0001. n.s. not significant, HNSCC head and neck squamous cell carcinoma, CTLA-4 cytotoxic T-lymphocyte antigen 4, CCR CC chemokine receptor, CFSE carboxyfluorescein diacetate succinimidyl ester, TCR T cell receptor