
 This work is licensed under a
This work is licensed under a Figure 2.
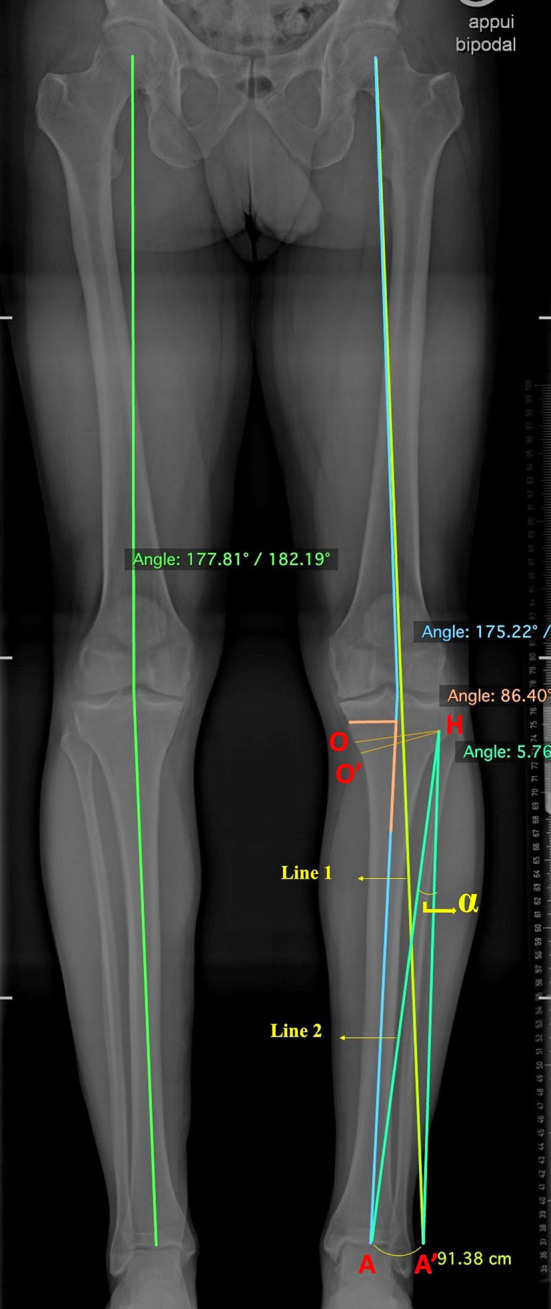
Planning OWPTO according to Miniaci’s technique using AP long-leg standing radiograph. The line 1 was drawn from the hip center through the pre-established correction point at the knee tibial plateau (this point can be positioned between 50% and 62.5% of the tibial plateau from the medial edge; the more lateral it is, the more overcorrection of the valgus axis is achieved). The hinge point H was identified, approximately 15–20 mm from the joint line and 5–10 mm from the lateral cortex. Line 2 was drawn connecting point H with the center of the ankle A. Subsequently, a circular arc was drawn with the center at point H and a radius of HA from point A to the intersection with line 1, resulting in point A′. The angle α between lines HA and HA′ represents the correction angle. Finally, a predicted osteotomy line O was drawn from point H to the predicted medial osteotomy site, approximately 40 mm inferior to the medial tibial plateau. A predicted opening line O′ was drawn from line O at the determined correction angle, and the correction gap was measured.