

Abstract
Background
Chronic rhinosinusitis (CRS) is a heterogeneous disorder with a wide range of validated subjective and objective assessment tools to assess disease severity. However, a comprehensive and easy‐to‐use tool that integrates these measures for determining disease severity and response to treatment is still obscure. The objective of this study was to develop a standardized assessment tool that facilitates diagnosis, uniform patient monitoring, and comparison of treatment outcomes between different centers both in routine clinical practice and in research.
Methods
To develop this tool, published literature on assessment tools was searched on various databases. A panel of 12 steering committee members conducted an advisory board meeting to review the findings. Specific outcome measures to be included in a comprehensive assessment tool and follow‐up sheet were then collated following consensus approval from the panel. The tool was further validated for content and revised with expert recommendations to arrive at the finalized Nasal Polyp Patient Assessment Scoring Sheet (N‐PASS) tool.
Results
The N‐PASS tool was developed by integrating the subjective and objective measures for CRS assessment. Based on expert opinions, N‐PASS was revised to be used as an easy‐to‐use guidance tool that captures patient‐reported and physician‐assessed components for comprehensively assessing disease status and response to treatment.
Conclusion
The N‐PASS tool can be used to aid in the diagnosis and management of CRS cases with nasal polyps. The tool would also aid in improved monitoring of patients and pave the way for an international disease registry.
Level of evidence
Oxford Level 3.
Keywords: assessment, biologics, consensus, control, diagnosis, eosinophilic, EPOS, nasal polyps, outcome measure, rhinosinusitis, scoring sheet, sinusitis, SinoNasal Outcome Test, type 2
Nasal Polyp Patient Assessment Scoring Sheet (N‐PASS) was developed as an integrated tool for assessing chronic rhinosinusitis (CRS) severity and treatment response. Refined through expert validation, N‐PASS serves as a user‐friendly guide, capturing both patient‐reported and physician‐assessed components for comprehensive CRS diagnosis and management.
1. INTRODUCTION
Chronic rhinosinusitis (CRS) is an inflammatory disorder of the paranasal sinuses, attributed to multiple underlying factors and often leading to chronic sinonasal manifestations. 1 , 2 The presence of two or more cardinal symptoms, such as nasal obstruction, facial pain/pressure, thick nasal discharge, reduced or loss of sense of smell (LoS), and an inflamed sinus that last for at least 12 weeks, is diagnostic of CRS. 3
Traditionally, CRS is classified based on the presence or absence of nasal polyps (NP) as CRS with NP (CRSwNP) and CRS without NP (CRSsNP). 4 Typically, CRSwNP patients manifest comorbid conditions such as asthma, allergic rhinitis, and aspirin‐exacerbated respiratory disease. 5 More recently CRS has been classified as primary and secondary. Based on the endotype dominance, primary CRS is further classified as type 2 or non‐type 2, whereas secondary CRS is classified based on local pathology, mechanical, inflammatory, and immunological factors. 3
It is estimated that symptomatic CRS affects nearly 2.1% of the population in the United States and nearly 2%–4% of the European population, of which 18%–30% are diagnosed with CRSwNP. 6 , 7 , 8 , 9 Interestingly, the Middle East region has demonstrated a very high (20%–49%) prevalence of CRS compared to other populations. 10 , 11 , 12 The global prevalence of CRS varies significantly, essentially due to variances in the diagnostic measures used. 13
As CRSwNP significantly impacts patients' quality of life (QoL) and is a substantial clinical and economic burden, 14 astute diagnosis is crucial for improving patient care and deciding between low‐ and high‐value interventions. 13 Development and utilization of relevant and accurate assessment tools are critical to this end.
For CRSwNP evaluation, there are a variety of outcome measures, including objective endpoints such as the University of Pennsylvania Smell Identification Test, the nasal polyp score (NPS), 15 , 16 and the Lund–Mackay computed tomography (LMK‐CT) score, 17 and patient‐reported endpoints such as nasal congestion score, the LoS, 18 22‐item SinoNasal Outcome Test (SNOT‐22) 19 , 20 Rhinosinusitis Disability Index, 21 visual analog scale (VAS), 3 and total symptom score. 18 Additionally, there are a wide range of validated, subjective, and objective CRS assessment tools. 22
There is a consensus among contemporary guidelines for the value of nasal endoscopy, CT imaging, and allergy testing for evaluation. 23 Whereas objective measures are important, subjective patient‐reported outcomes have recently gained much attention as an important contributor to the measurement of outcomes. 24
Though several treatment options are available, the lack of clear criteria regarding the choice of treatment for individual patients remains a concern when attempting to optimize outcomes and reduce unnecessary risk.
A recent study emphasized the need to overcome heterogeneity in outcome measures and the need to have core outcomes such as disease‐specific QoL, NPS, evaluation of sense of smell alongside the need for oral corticosteroids, and surgical treatment and complications from the disease or treatment. 25
A comprehensive tool that consolidates both objective and patient‐reported data will assist in patient selection and also aid in patient education regarding treatment options. This study describes the development and usefulness of a novel instrument, the Nasal Polyp Patient Assessment Scoring Sheet (N‐PASS) tool, to comprehensively assess CRSwNP patients in routine clinical practice and to enable decisions on the treatment modalities that are best suited.
2. METHODOLOGY
A comprehensive literature search assessed CRSwNP management and available assessment tools using publications up to July 2021 from databases like Medline, Scopus, Embase, ScienceDirect, Clinical Key, and Cochrane. A 12‐member panel of steering committee members (SCMs) from the field of otorhinolaryngology participated in an initial advisory board meeting (ABM) to review and discuss the evidence from the literature search, including existing guidelines, for CRSwNP treatment and monitoring. The SCMs involved in developing the N‐PASS tool were selected based on clinical and research experience. In the ABM, the experts reviewed all the subjective and objective outcome measures used for CRSwNP assessment and graded them as “most relevant,” “less relevant,” and “least relevant.” Through multiple discussions on virtual platforms, the SCMs collated the “most relevant” specific outcome measures into a comprehensive CRSwNP assessment tool, deliberated further based on their clinical expertise, and finally added these into the N‐PASS tool. Consensus approval was then sought among this panel, and a high agreement was defined as an agreement among more than 75% of the SCMs. Where agreement could not be reached, further discussions and deliberations were held to either include or exclude the components based on the degree of agreement.
The tool was then validated for content by a group of five international experts from the field of otorhinolaryngology. Content validity is the degree to which a tool measures the intended constructs. Using ratings of item relevance (4‐point ordinal scale) by content experts, the item and scale content validity index (CVI) was calculated. 26 , 27
The tool was revised based on expert recommendations. Additionally, the key domains and items recommended in core outcome sets of CRS (CHROME) were duly considered in the development of this tool. 28 The revised tool was circulated among the initial panel of 12 SCMs. Agreement from all SCMs led to the finalization of the tool (Figure 1).
FIGURE 1.
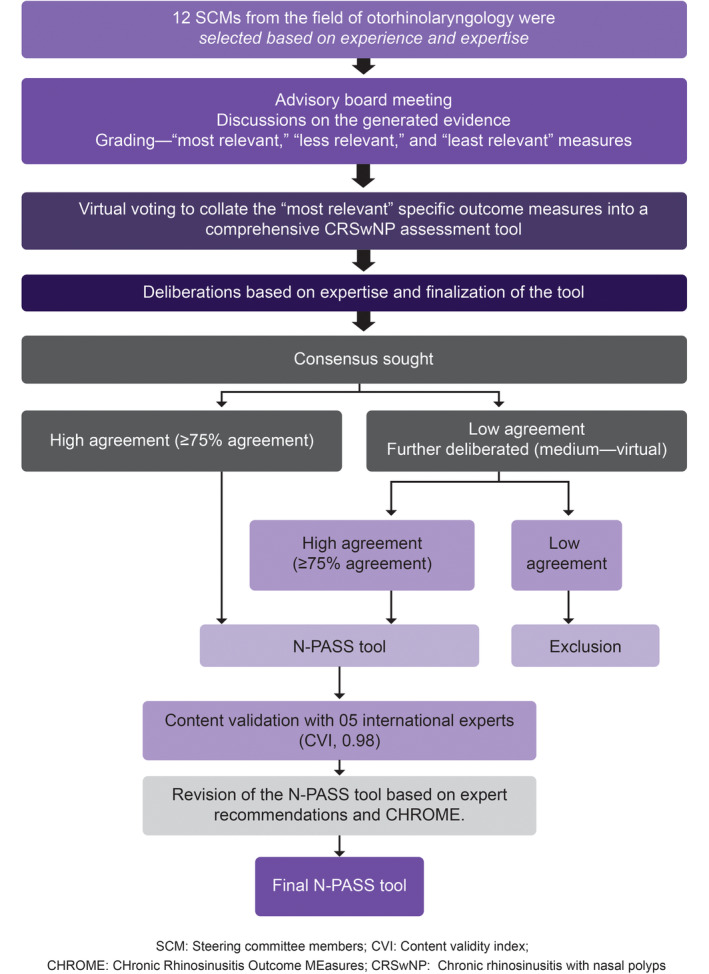
Flow diagram to depict the process of N‐PASS tool development. N‐PASS, Nasal Polyp Patient Assessment Scoring Sheet.
3. RESULTS
All available outcome measures that the expert panel considered most relevant in the assessment of patients with CRSwNP were critiqued and are presented in Table 1 and Table 2. Table 3 presents the excluded parameters that could not reach a high agreement.
TABLE 1.
Components of the N‐PASS evaluation sheet (high agreement parameters).
| Domain evaluated | Components | Variables | Remarks |
|---|---|---|---|
| Medical history | A 10‐point self‐reported VAS 3 |
Severity of symptoms: 0 = Not at all troublesome 10 = Extremely troublesome
|
Grading: Not bothersome: <5 Present/impaired: >5 |
| ESS surgery |
|
||
| Courses of systemic corticosteroid in the last 6 months |
|
||
| Relevant comorbidities |
|
||
| Investigations | Laboratory evaluation |
|
Blood eosinophils can be influenced by the use of systemic steroids |
| Assessment of disease severity | Endoscopic NPS 15 , 16 |
|
The maximum score is 8 (4 points per nasal cavity) |
| Lund–Mackay CT scoring system 17 |
|
Grading of each sinus: 0 = absence (no mucosal thickening) 1 = partial opacification 2 = complete opacification The osteomeatal complex is graded as follows: 0 = not occluded 2 = occluded, deriving a maximum score of 12 per side |
|
| SNOT‐22 19 |
|
The range of the SNOT‐22 score is 0–110, where lower scores indicate less impact. The score is classified as follows: 8–20: Mild 21–50: Moderate >50: Severe |
|
| Treatment decision |
|
Treatment is at the discretion of the physician. Physicians are encouraged to use the follow‐up sheet with all interventions. |
Abbreviations: AMT, appropriate medical therapy; CT, computed tomography; ESS, endoscopic sinus surgery; IgE, immunoglobulin E; N‐PASS, nasal polyp patient assessment scoring sheet; NPS, nasal polyp score; NSAID‐ERD/AERD: nonsteroidal anti‐inflammatory drug‐exacerbated respiratory disease/aspirin‐exacerbated respiratory disease; SNOT, SinoNasal Outcome Test; VAS, visual analog scale.
TABLE 2.
Components of the N‐PASS follow‐up sheet (high agreement parameters).
| Domain evaluated | Components | Variables | Remarks |
|---|---|---|---|
| Medical history | If started on biologics |
|
|
| A 10‐point self‐reported VAS 3 |
Severity of symptoms: 0 = not at all troublesome 10 = extremely troublesome
|
Grading: Not bothersome: <5 Present/impaired: >5 |
|
| VAS score of medication adherence in the last month 29 |
|
||
| Rescue treatment needed in the last 6 months |
|
||
| Improvement in relevant comorbidities |
|
||
| Assessment of disease severity | Endoscopic NPS 15 , 16 |
|
The maximum score is 8 (4 points per nasal cavity) |
| SNOT‐22 19 |
|
The range of the SNOT‐22 score is 0–110, where lower scores indicate less impact. The score is classified as follows:
|
|
| Treatment | Decision |
|
At the discretion of the treating physician |
| Adverse effects | Recording any possible complications or side effects that may occur during the treatment |
Abbreviations: AMT, appropriate medical treatment; N‐PASS, nasal polyp patient assessment scoring sheet; NPS, nasal polyp score; NSAID‐ERD/AERD, nonsteroidal anti‐inflammatory drug‐exacerbated respiratory disease/aspirin‐exacerbated respiratory disease; SNOT, SinoNasal Outcome Test; VAS, Visual analog scale.
TABLE 3.
Outcome measures excluded from the tool (low agreement).
| Outcome measure | |
|---|---|
| PROMs | Global
|
Disease‐specific
| |
| Psychophysical olfactory testing |
|
| Investigations |
|
Abbreviations: ECP, eosinophil cationic protein; IL, interleukin; LoS, loss of smell; LMK, Lund–Mackay; NCS, nasal congestion score; RSDI, Rhinosinusitis Disability Index; SF‐36, 36 Item Short Form Survey; UPSIT, University of Pennsylvania Smell Identification Test.
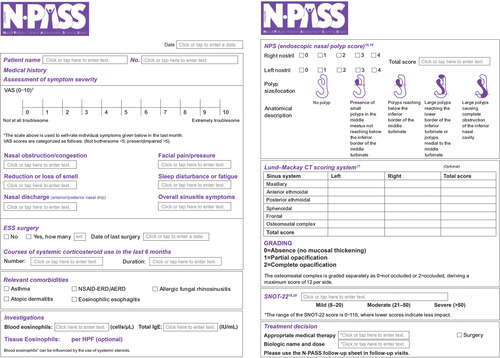
The final tool (Figure 2) included six evaluation domains: cardinal symptoms (through VAS), relevant comorbidities, investigations, previous interventions, QoL affection (through SNOT‐22), and nasal polyposis assessment (through NPS and/or LMK).
FIGURE 2.
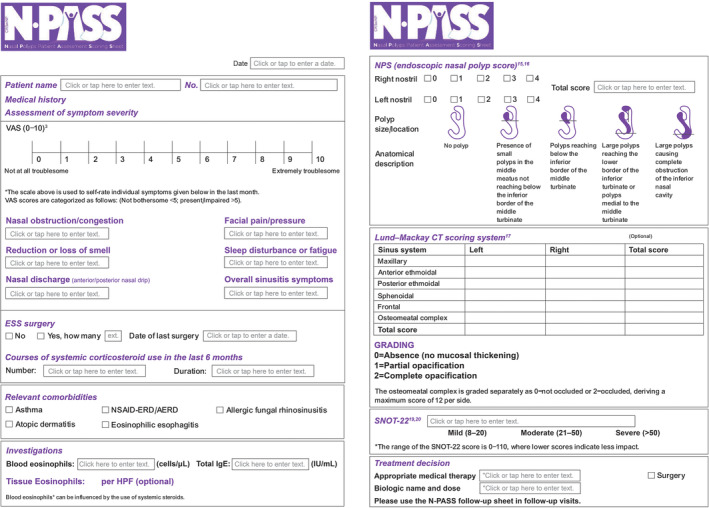
The N‐PASS tool. N‐PASS, Nasal Polyp Patient Assessment Scoring Sheet.
Whereas a high agreement was arrived at for all domains, discussions led to the decision that the LMK‐CT scoring system in the N‐PASS tool should be an optional measure. Arguments for this modification include feasibility issues in different countries and insurance approvals. Concerns about radiation exposure limit its use for all patients and discourage repeated application. Hence, despite a high agreement to include this scoring system, it was decided to make the measure optional. Due to safety and radiation exposure concerns, there was little agreement to include the LMK score in the follow‐up sheet, leading to its exclusion. Similarly, tissue eosinophil count was added as an optional measure.
After initial development, the N‐PASS tool underwent content validation (overall CVI, 0.98). The item CVI score for all items was at or above 0.8, except for one item (date of diagnosis of NPs) that reached a score of 0.6. Considering this, the item was excluded from the final tool. Additionally, recommendations from the experts that included the addition of overall sinusitis symptoms VAS score, modification in the duration of rescue treatment, adherence to medications VAS score, 29 and improving the general flow of the tool were incorporated into the tool and recirculated among the SCMs for their approval.
3.1. N‐PASS tool as a diagnostic aid and a measure of disease control
3.1.1. The N‐PASS main form
Adequate evaluation of CRSwNP requires a comprehensive clinical history, including symptoms, their severity and duration, investigations, allergy evaluation, previous medical treatments, and surgical intervention. In addition to the four cardinal symptoms (nasal obstruction, LoS, facial pain, and nasal discharge), patients may present with headache, fatigue, cough, sleep deprivation, earache, or dysphonia. 3 , 30 However, none of these symptoms are specific enough to arrive at a diagnosis. A symptom‐based definition alone has a specificity of just 12% and a positive predictive value of only 40%. Therefore, the European position paper on rhinosinusitis and nasal polyps (EPOS) 2012 advised physicians to assess the severity of symptoms through the patient‐reported VAS scale with a measurable continuum of 0–10. VAS is easy to use by patients and physicians alike, and a recent systematic review reported that VAS had been the most commonly adopted measure for nasal obstruction and olfactory loss. 31 Considering the critical value of the VAS score as a validated patient‐reported tool to evaluate symptom severity, it has been incorporated into the N‐PASS tool. A VAS score of “less than five” indicates symptoms that are “not bothersome,” whereas a VAS score of “greater than five” suggests the “presence of symptoms or impaired functioning” 3 (Data S1). As such, VAS scores easily monitor the change in CRS symptoms and disease severity, which would translate into improved clinical decision‐making. 22 The strongest patient‐reported outcome measure is the SNOT‐22, a validated CRS health‐related QoL measure and a helpful tool for quantifying changes in symptoms, which can be used to predict the extent of postoperative improvement. 32 Additionally, the tool assesses the history of endoscopic sinus surgery and rescue treatment with a course of corticosteroids in the past 6 months as recommended by EPOS 2020 in the assessment of clinical control of CRS. 3 The details of SNOT‐22 are described in Data S1.
Multiple studies have demonstrated a relationship between tissue eosinophilia and blood eosinophil count. 33 , 34 , 35 In contrast, the benefit of serum immunoglobulin E (IgE) remains unclear; however, in a recent prospective study, IgE levels were significantly higher in eosinophilic CRSwNP patients. 36 EPOS 2020 defined cutoff points of serological absolute eosinophil count ≥250 μ/L, total IgE ≥100 IU/mL, or tissue eosinophils ≥10/HPF as indicators for type 2 inflammation. 3 The N‐PASS tool incorporates blood eosinophil count, tissue eosinophil count (as an option), and total IgE level as indicators of type 2 inflammation within CRSwNP patients. Additionally, it is important to consider the previous use of oral corticosteroids as they may suppress blood eosinophil count. 37
The assessment of disease severity also includes objective evidence of mucosal inflammation through direct endoscopic examination or CT imaging. 38 At this stage, clinicians often employ the NPS for polyp size assessment with a maximum score of 8 with 4 points each for the nasal cavity and LMK score for assessing the maxillary, anterior or posterior ethmoidal, sphenoidal, frontal, and osteomeatal complex. Grading for each sinus will be zero if there is no mucosal thickening, 1 for partial, and 2 for total opacification. In addition, the osteomeatal complex is graded separately as zero if not occluded or 2 if occluded, deriving a maximum score of 12 per side (Data S1).
3.1.2. N‐PASS follow‐up form
A follow‐up form was developed to collect patients' data after any medical or surgical intervention (Figure 3). The follow‐up sheet focuses on the number of therapies, possible adverse effects of the treatment, and improvements in the subjective and objective scores of the CRSwNP patients (Table 2). It records the name and number of weeks of biologics used, when applicable. Symptom severity was recorded with the help of a VAS score (as mentioned above in the main sheet). VAS score of medication adherence was recorded as 0%—“I never take medications” and 100%—“I take all the prescribed medications.” Due to the lack of CRS‐specific compliance measures, a simple VAS score of medication adherence was incorporated into the follow‐up sheet. 29 A record of rescue treatment in the last 6 months such as oral corticosteroids or the need for surgery was also included. Improvement in relevant comorbidities, SNOT‐22 score, and NPS scores was additionally recorded. Adverse events of therapies are also recorded.
FIGURE 3.
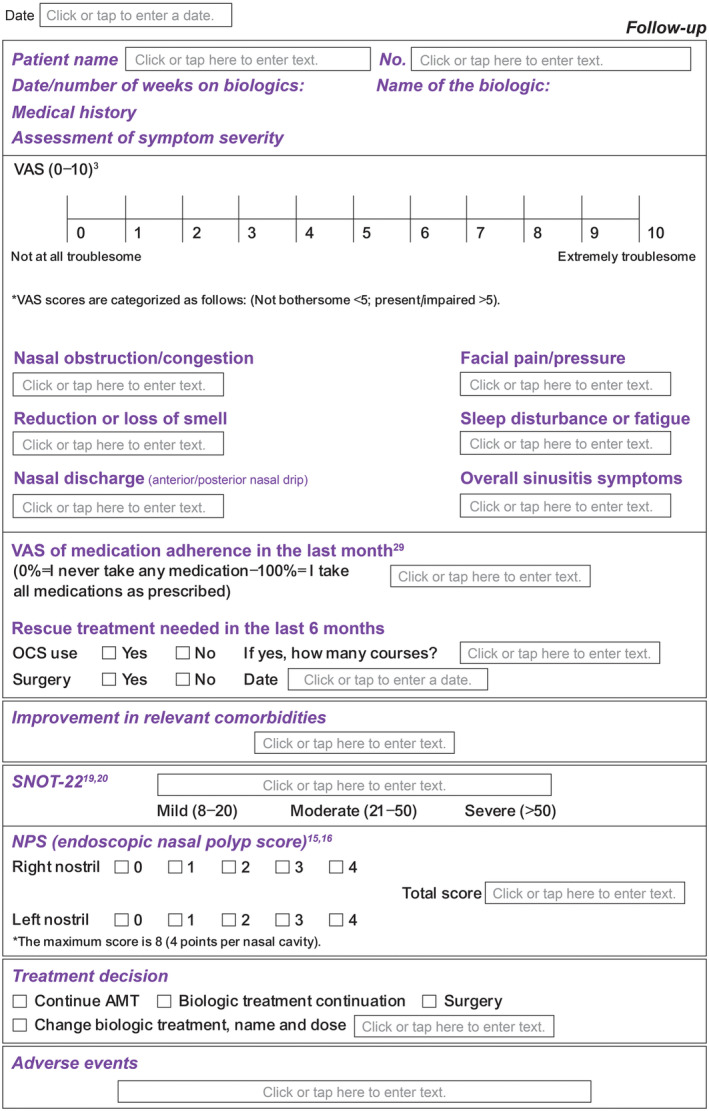
The N‐PASS follow up tool. N‐PASS, Nasal Polyp Patient Assessment Scoring Sheet.
3.1.3. Patient response form
Self‐reported patient outcome measures such as VAS and SNOT 22 were recorded by patients in this response form (Forms “A and B”). This allowed for effective use of the patient–physician time in the clinic and quick recording of the remaining outcome measures by the physician. In the follow‐up visit, the patient recorded medication adherence VAS score as well (Figure 4A,B).
FIGURE 4.
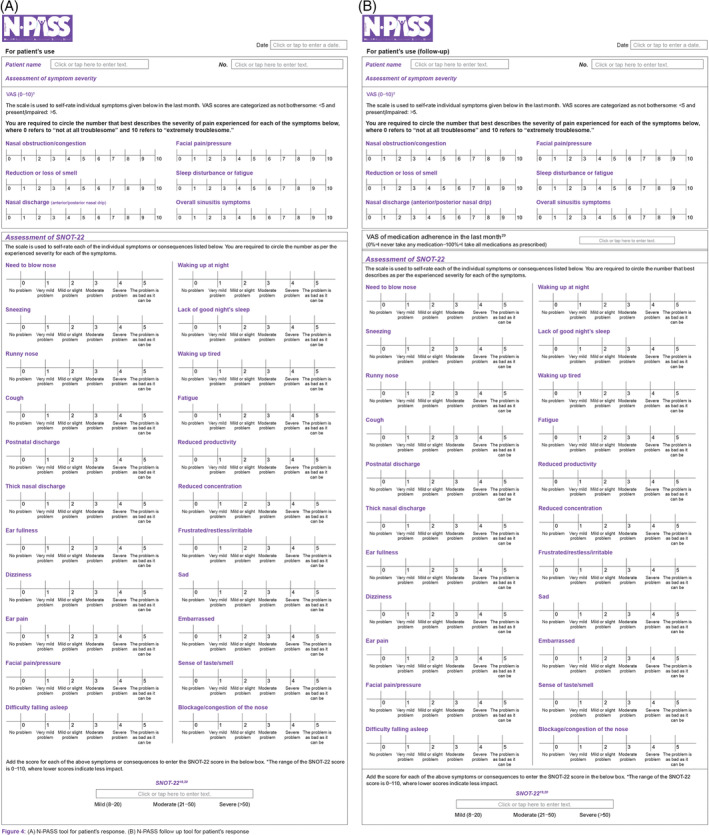
(A) The N‐PASS tool for patient's response. (B) The N‐PASS follow up tool for patient's response. N‐PASS, Nasal Polyp Patient Assessment Scoring Sheet.
4. DISCUSSION
The N‐PASS tool aims to streamline the diagnosis process, ensure consistent patient monitoring, and enable the comparison of treatment results across various centers, both in clinical and research settings. Physicians can assess the severity of the disease and response to treatment by examining the subjective and objective validated scores integrated into the N‐PASS tool, based on published recommendations. The follow‐up form will aid in comparing outcomes across various management options, which will be determined according to specified cutoff points.
Response criteria for biologic treatment in patients with CRSwNP as proposed by the multidisciplinary EUFOREA Expert Board Meeting included a reduction in NP size, reduced need for systemic corticosteroids, improved QoL, improved sense of smell, and reduced impact of comorbidities. 39 The follow‐up tool enabled the assessment of all of these five response criteria effectively. The process of the follow‐up sheet enables its user to arrive at a treatment decision as a continuation of appropriate medical therapy (AMT), continuation or change in biologic treatment, or surgery.
Anterior or posterior nasal discharge, nasal congestion, facial pain or pressure, and LoS that last for over 12 weeks define patients with CRSwNP. Many of these findings overlap with CRSsNP, making the diagnosis by these outcomes less sensitive and confusing. This overlap has led researchers to explore the cohort of CRS patients closely to identify any findings that specifically define CRSwNP and CRSsNP or distinguish between the two conditions. However, the commonality between the two conditions being considered, the need for more specific diagnostic criteria is imperative. 40 , 41 It is also reported that patients with CRSwNP may be more sensitive to symptoms of CRS, prompting researchers and physicians to explore the severity of specific symptoms in facilitating diagnosis. 42
Once diagnosed, the management of this condition occurs at three levels. The first level of management is AMT, the second level is endoscopic sinus surgery, and the third is the use of biologic therapy. When AMT fails to provide relief, surgery is considered an option. When symptoms are severe and neither AMT nor surgery provides proper control of the disease, biologic therapy is considered. 43 Additionally, recent guidelines recommend considering the use of biologics as a treatment option in severe CRSwNP patients. EUFOREA 2019 guidelines recommended the use of biologics in patients with bilateral NPs with either history of surgery or no history of surgery. They further laid down the following criteria—evidence of type 2 inflammation, need for at least two courses of systemic in the past year, significant impaired QoL, significant LoS, and diagnosis of comorbid asthma. Patients with a history of surgery were required to additionally meet any three criteria, whereas those with no history were required to meet four of the above criteria. 44 EPOS 2020 made stringent modifications to the recommendations of EUFOREA 2019 and concluded that biologics are indicated in patients with bilateral polyps, who had had sinus surgery or were not fit for surgery, and who had three of the following characteristics: evidence of type 2 disease (tissue eosinophils ≥10/HPF or blood eosinophils ≥250 μ/L or total IgE ≥100 IU/mL), need for at least two courses of systemic medication as a second line of treatment if surgery is contraindicated, or upon meeting prescribed criteria. 3
Biologics should be considered in severe uncontrolled CRSwNP patients despite at least one previous endoscopic sinus surgery. 45 A study comparing omalizumab with sinus surgery in grade 3 CRSwNP patients concluded equal effectiveness in reducing the SNOT‐22 scores. 46 With the available evidence, biologics show a modest reduction in polyp size. As revision surgeries cannot prevent recurrence in these patients with type 2 inflammation, it may be likely that biologics will become an alternative therapeutic option to sinus surgery in the future. 44
When treating, patient selection is critical for reducing direct costs of health care, without negatively impacting clinical outcomes. The selection of treatment has a direct financial impact on the health care system. Additionally, when patients are suggested a treatment strategy that is backed by fulfilled EPOS criteria, there is a greater chance for support from insurance companies. 45 Hence, it may be inferred that systematic diagnosis allows for criteria of guidelines such as EPOS to be assessed and fulfilled, and a suitable treatment plan is the need of the hour.
Aboud et al. reported that objective outcome measures such as changes in nasal endoscopy scores only partially explained the changes in the QoL scores of patients (subjective score). 47 Kennedy et al. reported that symptom improvement does not correlate with the endoscopic resolution of mucosal abnormalities. 48 It is now understood that both subjective and objective symptoms are important in diagnosing CRS patients, but there is not a single diagnostic test that can collect this information. 13 Hopkins et al. concluded that symptom‐based outcome measures are the most important when evaluating any intervention; nevertheless, there is a need for including objective measures in the evaluation process. 49 Indeed, all reviews published since 2011 have included symptomatic improvement as the primary outcome. 49 The tool allowed for the measurement of disease control. With the aid of this tool, the treating physician can assess the status as controlled, partially controlled, or uncontrolled CRS as per the EPOS 2020 guidelines. 3
The N‐PASS tool was developed keeping in mind these gaps reported in the literature. It is designed to provide a comprehensive assessment of all relevant outcome measures (both subjective and objective), which are extensively used, widely endorsed, and known in the literature, yet remain to be consolidated. Additionally, it focuses on the severity of symptoms.
4.1. N‐PASS tool in the clinical setting
The treating practitioner is encouraged to perform his clinical assessment in a systematic and phased manner with the N‐PASS tool, which will allow for a clinical decision to be made based on both objective and patient‐reported outcomes.
Although objective measures are important, subjective patient‐reported outcomes have recently gained attention as an important contributor to the measurement of outcomes. 24 A study on patient‐reported and practitioner‐reported outcomes for CRS concluded that 3% of responses generated were objective measures, whereas the majority were subjective, thus highlighting that primary outcomes in future reviews should focus on subjective outcomes in rhinosinusitis‐related research. 28 , 45 , 49
The definition of CRS outlined by national guidelines and other national medical societies is often poorly followed by physicians. 50 As a result, heterogeneity in the outcomes is possible. The N‐PASS tool facilitates the standardized measurement of disease and its control. With the aid of this tool, the treating physician can assess the status as controlled, partially controlled, or uncontrolled CRS. 3 In 2017, the CHROME study defined four key domains of CRS, which have been considered in this tool. These aid in the standardized recording, diagnosis, and follow‐up of CRSwNP patients.
4.2. Influence of the N‐PASS tool‐based evaluation on treatment selection
Despite clinical heterogeneity, until recently, treatment options for patients with CRS were generally AMT or sinus surgery. In 2019, the first biologic approved in the United States for the treatment of CRSwNP was a monoclonal antibody targeting the alpha‐chain of the interleukin 4 (IL‐4) receptor that blocks both IL‐4‐ and IL‐13‐mediated signals. Other biologics, including anti‐IgE therapeutic antibodies and anti‐IL‐5 antibodies, were approved subsequently. The presence of type 2 inflammation is a strong indicator for the possible use of type 2 biologics such as dupilumab (anti‐IL‐4 receptor alpha), omalizumab (anti‐IgE), and mepolizumab. The N‐PASS tool developed by the panel of experts is expected to aid clinicians in customizing treatment modalities for individual patients. CRSwNP patients will be assessed through these widely endorsed components of the tool. Based on subjective and objective outcomes of the tool components, the clinician would be able to devise a suitable treatment plan. Furthermore, the follow‐up tool will allow for monitoring of the prognosis and modification of the treatment plan if required. The response criteria for biologics as defined by the EUFOREA Expert Board Meeting are assessed easily by this tool, which paves the way for therapy‐related decision‐making.
4.3. Strengths and limitations
The N‐PASS tool has several strengths. It is built of various recognized tools that assist physicians in decision‐making in the management of CRSwNP. This tool may act as a reference guide, providing its users information necessary for diagnosing, and thereafter planning treatment options.
The N‐PASS tool helps in identifying those criteria that facilitate decision‐making and follow‐up with regard to biologic treatment (assessment includes identifying the presence of type 2 inflammation, need for systemic corticosteroids, significantly impaired QoL, significant LoS, and diagnosis of comorbid asthma) and the response criteria for biologic treatment (including evaluation to assess reduced NP size, reduced need for systemic corticosteroids, improved QoL, improved sense of smell, and reduced impact of comorbidities) in patients with CRSwNP as per EUFOREA Expert Board Meeting and EPOS 2020. 3 , 44 It can be appreciated that both these evaluations are easy with the N‐PASS tool, which in turn allows for treatment planning that is backed by expert recommendations and guidelines. Additionally, the presence of a follow‐up sheet allows for documentation of the improvement or deterioration of symptoms during treatment.
Experts have opined that several treatment options are available without clear criteria regarding patient selection for specific biologic therapy in the local clinical setting. The N‐PASS tool is easy to use in routine clinical practice, and it enables its user to assess the patient systematically and comprehensively, which further facilitates treatment planning. The patient's response to treatment can also be recorded, guiding further management.
All SCMs belonged to the Middle East region to facilitate in‐person deliberations and for logistic convenience. We attempted to achieve a larger geographic representation and perspective by performing content validation with five international academic clinicians with vast expertise and experience in this domain.
5. CONCLUSION
The N‐PASS (main and follow‐up sheet) tool has incorporated important and commonly used assessment tools for easy reference of physicians. The tool, integrating both subjective and objective outcome measures, assists physicians with documentation and close follow‐up of symptoms and with treatment planning. The N‐PASS tool can substantially aid in the standardized evaluation of CRSwNP patients.
CONFLICT OF INTEREST
Saad Alsaleh received honoraria from Sanofi and GSK for lectures and advisory board activities. Nehal Kamal, BS Pharm, is an employee of Sanofi and may hold shares and/or stock options in the company. Claire Hopkins has done advisory board work for Sanofi, GSK, Lilly, and Astra Zeneca. Omar Abu Suliman has been involved in advisory board work for Sanofi and GSK. Naif H. Al‐Otaibi has received advisory board fees and honoraria for lectures from Sanofi and GSK. Joseph K. Han is a research consultant for Sanofi Regeneron GSK AZ and Genentech. Amin Javer is a speaker/consultant for GSK, Sanofi Regeneron, iView Therapeutics, and SaNOtize. Ahmad R. Sedaghat has been involved in research funding and advisory board participation for Sanofi/Regeneron and GSK. Philippe Gevaert declares he has received lecture fees and/or participation at expert board meetings from ALK‐Abelló, Argenx, AstraZeneca, Genentech, GlaxoSmithKline, Novartis, Regeneron, Roche, Sanofi, and Stallergenes Greer. The remaining authors declare no conflicts of interest.
Supporting information
Data S1. Supporting information.
ACKNOWLEDGMENTS
This research did not receive any specific grant from funding agencies in the public, commercial, or not‐for‐profit sectors. Medical writing/editorial assistance for the preparation of this manuscript was provided by BioQuest Solutions, which was funded by Sanofi. The primary meeting while developing the tool was logistically supported by Sanofi.
Alsaleh S, Kamal N, Hopkins C, et al. Assessment of chronic rhinosinusitis with nasal polyps: Development of the Nasal Polyp Patient Assessment Scoring Sheet tool. Laryngoscope Investigative Otolaryngology. 2024;9(3):e1277. doi: 10.1002/lio2.1277
REFERENCES
- 1. Sedaghat AR. Chronic rhinosinusitis. Am Fam Physician. 2017;96(8):500‐506. [PubMed] [Google Scholar]
- 2. Viskens AS, Wils T, Van Bulck P, Cools L, Vanderveken O, Hellings PW. Multiple reasons underlaying uncontrolled disease in the majority of chronic rhinosinusitis patients. Front Allergy. 2022;3:1048385. doi: 10.3389/falgy.2022.1048385 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Fokkens WJ, Lund VJ, Hopkins C, et al. European position paper on rhinosinusitis and nasal polyps 2020. Rhinology. 2020;58(suppl S29):1‐464. [DOI] [PubMed] [Google Scholar]
- 4. Fokkens WJ, Lund VJ, Mullol J, et al. European position paper on rhinosinusitis and nasal polyps 2012. Rhinol Suppl. 2012;23:3‐298. [PubMed] [Google Scholar]
- 5. Oykhman P, Paramo FA, Bousquet J, Kennedy DW, Brignardello‐Petersen R, Chu DK. Comparative efficacy and safety of monoclonal antibodies and aspirin desensitization for chronic rhinosinusitis with nasal polyposis: a systematic review and network meta‐analysis. J Allergy Clin Immunol. 2022;149(4):1286‐1295. doi: 10.1016/j.jaci.2021.09.009 [DOI] [PubMed] [Google Scholar]
- 6. Bachert C, Bhattacharyya N, Desrosiers M, Khan AH. Burden of disease in chronic rhinosinusitis with nasal polyps. J Asthma Allergy. 2021;14:127‐134. doi: 10.2147/JAA.S290424 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Benjamin MR, Stevens WW, Li N, et al. Clinical characteristics of patients with chronic rhinosinusitis without nasal polyps in an academic setting. J Allergy Clin Immunol Pract. 2019;7(3):1010‐1016. doi: 10.1016/j.jaip.2018.10.014 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Khan A, Vandeplas G, Huynh TMT, et al. The Global Allergy and Asthma European Network (GALEN) rhinosinusitis cohort: a large European cross‐sectional study of chronic rhinosinusitis patients with and without nasal polyps. Rhinology. 2019;57(1):32‐42. doi: 10.4193/Rhin17.255 [DOI] [PubMed] [Google Scholar]
- 9. Sedaghat AR, Kuan EC, Scadding GK. Epidemiology of chronic rhinosinusitis: prevalence and risk factors. J Allergy Clin Immunol Pract. 2022;10(6):1395‐1403. doi: 10.1016/j.jaip.2022.01.016 [DOI] [PubMed] [Google Scholar]
- 10. Abualnasr SA, Alattas AM, Abualnasr AA, Alsrisri HA, Aljeraisi T. Prevalence of chronic rhino sinusitis and it's recurrent after treatment compare to its recurrent after surgery at Saudi Arabia, 2016. Int J Adv Res. 2017;5:2310‐2318. [Google Scholar]
- 11. Verim A, Cebeci F, Başer E, Çalim ÖF, Kadioğlu D, Kocagöz GD. Prevalence of chronic rhinosinusitis in the setting of Behçet disease. J Craniofac Surg. 2015;26(1):186‐190. doi: 10.1097/SCS.0000000000001202 [DOI] [PubMed] [Google Scholar]
- 12. Homood MA, Alkhayrat SM, Kulaybi KM. Prevalence and risk factors of chronic sinusitis among people in Jazan region’ KSA. Egypt J Hosp Med. 2017;69(5):2463‐2468. doi: 10.12816/0041695 [DOI] [Google Scholar]
- 13. Rudmik L. Economics of chronic rhinosinusitis. Curr Allergy Asthma Rep. 2017;17(4):20. doi: 10.1007/s11882-017-0690-5 [DOI] [PubMed] [Google Scholar]
- 14. Klonaris D, Doulaptsi M, Karatzanis A, Velegrakis S, Milioni A, Prokopakis E. Assessing quality of life and burden of disease in chronic rhinosinusitis: a review. Rhinol Online. 2019;2(2):6‐13. doi: 10.4193/RHINOL/18.067 [DOI] [Google Scholar]
- 15. Gevaert P, Lang‐Loidolt D, Lackner A, et al. Nasal IL‐5 levels determine the response to anti‐IL‐5 treatment in patients with nasal polyps. J Allergy Clin Immunol. 2006;118(5):1133‐1141. doi: 10.1016/j.jaci.2006.05.031 [DOI] [PubMed] [Google Scholar]
- 16. Gevaert P, De Craemer J, Bachert C, et al. European Academy of Allergy and Clinical Immunology position paper on endoscopic scoring of nasal polyposis. Allergy. 2023;78(4):912‐922. doi: 10.1111/all.15650 [DOI] [PubMed] [Google Scholar]
- 17. Lund VJ, Mackay IS. Staging in rhinosinusitus. Rhinology. 1993;31(4):183‐184. [PubMed] [Google Scholar]
- 18. Fokkens W, Lund V, Mullol J, European Position Paper on Rhinosinusitis and Nasal Polyps group . European position paper on rhinosinusitis and nasal polyps 2007. Rhinol Suppl. 2007;20:1‐136. [PubMed] [Google Scholar]
- 19. Hopkins C, Gillett S, Slack R, Lund VJ, Browne JP. Psychometric validity of the 22‐item Sinonasal Outcome Test. Clin Otolaryngol. 2009;34(5):447‐454. doi: 10.1111/j.1749-4486.2009.01995.x [DOI] [PubMed] [Google Scholar]
- 20. Toma S, Hopkins C. Stratification of SNOT‐22 scores into mild, moderate or severe and relationship with other subjective instruments. Rhinology. 2016;54(2):129‐133. doi: 10.4193/Rhino15.072 [DOI] [PubMed] [Google Scholar]
- 21. Benninger MS, Senior BA. The development of the rhinosinusitis disability index. Arch Otolaryngol Head Neck Surg. 1997;123(11):1175‐1179. doi: 10.1001/archotol.1997.01900110025004 [DOI] [PubMed] [Google Scholar]
- 22. Han JK, Bachert C, Lee SE, et al. Estimating clinically meaningful change of efficacy outcomes in inadequately controlled chronic rhinosinusitis with nasal polyposis. Laryngoscope. 2022;132(2):265‐271. doi: 10.1002/lary.29888 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Kaper NM, van der Heijden GJMG, Cuijpers SH, Stokroos RJ, Aarts MCJ. A comparison of international clinical practice guidelines on adult chronic rhinosinusitis shows considerable variability of recommendations for diagnosis and treatment. Eur Arch Otorhinolaryngol. 2020;277(3):659‐668. doi: 10.1007/s00405-019-05752-7 [DOI] [PubMed] [Google Scholar]
- 24. Ting F, Hopkins C. Outcome measures in chronic rhinosinusitis. Curr Otorhinolaryngol Rep. 2018;6(3):271‐275. doi: 10.1007/s40136-018-0215-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Abdulghany A, Surda P, Hopkins C. Core outcome measures in chronic rhinosinusitis with nasal polyps: in practice and research. Am J Rhinol Allergy. 2023;37(2):232‐239. doi: 10.1177/19458924231154070 [DOI] [PubMed] [Google Scholar]
- 26. Polit DF, Beck CT, Owen SV. Is the CVI an acceptable indicator of content validity? Appraisal and recommendations. Res Nurs Health. 2007;30(4):459‐467. doi: 10.1002/nur.20199 PMID: 17654487. [DOI] [PubMed] [Google Scholar]
- 27. Kipli M, Khairani AZ. Content validity index: an application of validating CIPP instrument for programme evaluation. IMRJ. 2020;2(4):31‐40. doi: 10.54476/iimrj313 [DOI] [Google Scholar]
- 28. Hopkins C, Hettige R, Soni‐Jaiswal A, et al. CHronic Rhinosinusitis Outcome MEasures (CHROME), developing a core outcome set for trials of interventions in chronic rhinosinusitis. Rhinology. 2018;56(1):22‐32. doi: 10.4193/Rhin17.247 [DOI] [PubMed] [Google Scholar]
- 29. Zeller A, Ramseier E, Teagtmeyer A, Battegay E. Patients' self‐reported adherence to cardiovascular medication using electronic monitors as comparators. Hypertens Res. 2008;31(11):2037‐2043. doi: 10.1291/hypres.31.2037 [DOI] [PubMed] [Google Scholar]
- 30. Rosenfeld RM, Andes D, Bhattacharyya N, et al. Clinical practice guideline: adult sinusitis. Otolaryngol Head Neck Surg. 2007;137(3 suppl):S1‐S31. doi: 10.1016/j.otohns.2007.06.726 [DOI] [PubMed] [Google Scholar]
- 31. Ta NH, Gao J, Philpott C. A systematic review to examine the relationship between objective and patient‐reported outcome measures in sinonasal disorders: recommendations for use in research and clinical practice. Int Forum Allergy Rhinol. 2021;11(5):910‐923. doi: 10.1002/alr.22744 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Khan AH, Reaney M, Guillemin I, et al. Development of Sinonasal Outcome Test (SNOT‐22) domains in chronic rhinosinusitis with nasal polyps. Laryngoscope. 2022;132(5):933‐941. doi: 10.1002/lary.29766 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Bryson JM, Tasca RA, Rowe‐Jones JM. Local and systemic eosinophilia in patients undergoing endoscopic sinus surgery for chronic rhinosinusitis with and without polyposis. Clin Otolaryngol Allied Sci. 2003;28(1):55‐58. doi: 10.1046/j.1365-2273.2003.00666.x [DOI] [PubMed] [Google Scholar]
- 34. Sakuma Y, Ishitoya J, Komatsu M, et al. New clinical diagnostic criteria for eosinophilic chronic rhinosinusitis. Auris Nasus Larynx. 2011;38(5):583‐588. doi: 10.1016/j.anl.2011.01.007 [DOI] [PubMed] [Google Scholar]
- 35. Hu Y, Cao PP, Liang GT, Cui YH, Liu Z. Diagnostic significance of blood eosinophil count in eosinophilic chronic rhinosinusitis with nasal polyps in Chinese adults. Laryngoscope. 2012;122(3):498‐503. doi: 10.1002/lary.22507 [DOI] [PubMed] [Google Scholar]
- 36. Sheng H, Yao X, Wang X, Wang Y, Liu X, Zhang L. Prevalence and clinical implications of bronchiectasis in patients with overlapping asthma and chronic rhinosinusitis: a single‐center prospective study. BMC Pulm Med. 2021;21(1):211. doi: 10.1186/s12890-021-01575-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37. Ortega H, Llanos JP, Lafeuille MH, et al. Effects of systemic corticosteroids on blood eosinophil counts in asthma: real‐world data. J Asthma. 2019;56(8):808‐815. doi: 10.1080/02770903.2018.1502301 [DOI] [PubMed] [Google Scholar]
- 38. Rosenfeld RM, Piccirillo JF, Chandrasekhar SS, et al. Clinical practice guideline (update): adult sinusitis. Otolaryngol Head Neck Surg. 2015;152(2 suppl):S1‐S39. doi: 10.1177/0194599815572097 [DOI] [PubMed] [Google Scholar]
- 39. Bachert C, Han JK, Wagenmann M, et al. EUFOREA expert board meeting on uncontrolled severe chronic rhinosinusitis with nasal polyps (CRSwNP) and biologics: definitions and management. J Allergy Clin Immunol. 2021;147(1):29‐36. doi: 10.1016/j.jaci.2020.11.013 [DOI] [PubMed] [Google Scholar]
- 40. Stevens WW, Schleimer RP, Kern RC. Chronic rhinosinusitis with nasal polyps. J Allergy Clin Immunol Pract. 2016;4(4):565‐572. doi: 10.1016/j.jaip.2016.04.012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41. Dietz de Loos DA, Hopkins C, Fokkens WJ. Symptoms in chronic rhinosinusitis with and without nasal polyps. Laryngoscope. 2013;123(1):57‐63. doi: 10.1002/lary.23671 [DOI] [PubMed] [Google Scholar]
- 42. Talat R, Speth MM, Gengler I, et al. Chronic rhinosinusitis patients with and without polyps experience different symptom perception and quality of life burdens. Am J Rhinol Allergy. 2020;34(6):742‐750. doi: 10.1177/1945892420927244 [DOI] [PubMed] [Google Scholar]
- 43. Morse JC, Miller C, Senior B. Management of chronic rhinosinusitis with nasal polyposis in the era of biologics. J Asthma Allergy. 2021;14:873‐882. doi: 10.2147/JAA.S258438 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44. Fokkens WJ, Lund V, Bachert C, et al. EUFOREA consensus on biologics for CRSwNP with or without asthma. Allergy. 2019;74(12):2312‐2319. doi: 10.1111/all.13875 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45. Al‐Ahmad M, Alsaleh S, Al‐Reefy H, et al. Expert opinion on biological treatment of chronic rhinosinusitis with nasal polyps in the Gulf region. J Asthma Allergy. 2022;15:1‐12. doi: 10.2147/JAA.S321017 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46. Bidder T, Sahota J, Rennie C, Lund VJ, Robinson DS, Kariyawasam HH. Omalizumab treats chronic rhinosinusitis with nasal polyps and asthma together—a real life study. Rhinology. 2018;56(1):42‐45. doi: 10.4193/Rhino17.139 [DOI] [PubMed] [Google Scholar]
- 47. Aboud SK, Husain S, Gendeh BS. Comparison between endonasal endoscopic polyp size scores and quality of life outcome after optimal medical treatment. Rhinology. 2014;52(4):334‐340. doi: 10.4193/Rhino14.029 [DOI] [PubMed] [Google Scholar]
- 48. Kennedy DW, Wright ED, Goldberg AN. Objective and subjective outcomes in surgery for chronic sinusitis. Laryngoscope. 2000;110(S94):29‐31. doi: 10.1097/00005537-200003002-00008 [DOI] [PubMed] [Google Scholar]
- 49. Hopkins C, Philpott C, Crowe S, et al. Identifying the most important outcomes for systematic reviews of interventions for rhinosinusitis in adults: working with patients, public and practitioners. Rhinology. 2016;54(1):20‐26. doi: 10.4193/Rhino15.199 [DOI] [PubMed] [Google Scholar]
- 50. Xiao CC, Anderson M, Harless LD, Liang J. Shortcomings in the diagnosis of chronic rhinosinusitis: evaluating diagnosis by otolaryngologists and primary care physicians. Int Forum Allergy Rhinol. 2018;8(10):1107‐1113. doi: 10.1002/alr.22165 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data S1. Supporting information.