
Fig. 1. Examples of potential data sources for psychiatric research.
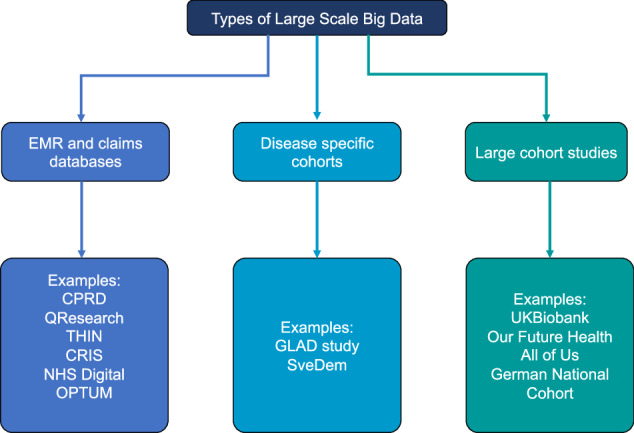
CPRD: Clinical Practice Research Datalink [174], QResearch (https://www.qresearch.org/), THIN: The health improvement network (https://www.the-health-improvement-network.com/), CRIS: Clinical Record Interactive Search, OPTUM (https://www.optum.com/), NHS Digital (https://digital.nhs.uk/), GLAD study: Genetic Links to Anxiety and Depression Study [175], SveDem: The Swedish Dementia Registry [176], UK Biobank [177], Our Future Health (https://ourfuturehealth.org.uk/), All of Us (https://allofus.nih.gov/), German National Cohort [178]. EMR and claims databases contain a variety of data formats which can be classified as structured or unstructured [69]. Structured data includes information such as age and gender, measurements such as blood pressure readings, height and also diagnosis codes, laboratory tests and medication prescribing. Whereas unstructured text includes narrative data such as clinical notes (e.g. biopsychosocial formulations, differential diagnoses, mental state examinations and risk formulations). Compared to narrative, unstructured data, structured data is easier to process with little pre-processing because it is stored in a standardised format. EHR and claims databases have vast patient numbers covering all diseases and disorders, giving the opportunity to look at psychiatric conditions and their comorbid diseases.