

Abstract
Introduction:
Spending a few hours to cool down in a cooling center reduces the impact of heat on health. But limited or lack of accessibility of these facilities is often a barrier to their utilization. The objective of this study was to assess accessibility of the cooling centers to heat-vulnerable populations in New York State (NYS) by various modes of transportation.
Methods:
We estimate the proximity of 377 cooling centers to general and heat-vulnerable populations in NYS (excluding New York City (NYC)) and determine their accessibility via walking, public transportation and driving. Distances between tract populations and nearest cooling center, and between cooling centers and public transportation stops were estimated. Accessibility in four metropolitan regions was determined via public transportation while accessibility in heat-vulnerable rural areas was estimated via driving.
Results:
Distances to nearest cooling center ranged from 0 to 53.2 miles with only a third of NYS population within walking distance (0.5 miles) of a cooling center. About 51% of heat-vulnerable tracts were within 0.5 miles, with an average distance of 2.4 miles to the nearest cooling center. Within the four metro politan regions 80% of cooling centers within 0.5 miles of a public transportation stop. All cooling centers in heat-vulnerable tracts were accessible via public transportation. In rural heat-vulnerable tracts, driving distances averaged at about 18 miles.
Conclusions:
In urban areas many residents were not within walking distance of a cooling center, but most, and nearly all in the most heat-vulnerable areas, were within walking distance of public transportation to a cooling center. In rural locations distances were longer, and accessibility is a greater issue. Cooling centers can be a valuable resource for general and heat-vulnerable populations during an extreme heat event. When planning and implementing cooling centers, it is therefore important to improve accessibility and address other barriers that can hamper their utilization.
1. Introduction
Average temperatures in New York State (NYS) have been increasing in recent years (Horton et al., 2014; Rosenzweig et al., 2011; New York State Department of Health, 2018) and are predicted to continue to increase during the 21st century along with the number of extreme hot days (individual days of maximum temperatures at or above 90 °F) (Horton et al., 2014). With these rises in summertime temperatures and heat events in NYS, we may see an increase in heat-related morbidity and mortality, especially among heat-vulnerable populations, as a greater number of extreme heat events (EHEs) and a rapidly aging population can offset a relative decline in vulnerability to heat (Sheridan and Allen, 2018). Over the past three decades, heat-related fatalities have exceeded all other causes of weather-related fatalities (United States Environmental Protection Agency, 2016; United States Natural Hazard Statistics, 2017a) in the United States (US) and since 2005, 25–58% of these deaths each year were attributed to extended exposure to outdoor heat or having little or no air-conditioning (A/C) (United States Natural Hazard Statistics, 2017b). Effects of extreme heat are largely preventable and spending a few hours in a cool or air-conditioned environment during EHEs can prevent or significantly reduce the impact of heat on health (Madrigano et al., 2000; Rosenthal et al., 2014; Uejio et al., 2011; Ostro et al., 2010). About 20% of homes in NYS do not have A/C and among those that have A/C about 10% do not use it (US Energy Information Administration, 2009). Residents of NYS including New York City (NYC) who opt not to use A/C most often cite costs of the equipment and utility bills as deterrents from purchase and utilization (Lane et al., 2014; Lu et al., 2017). The lack or under-utilization of A/C at home can affect an individual’s ability to avoid adverse health effects of heat, especially if they are already vulnerable to heat (Madrigano et al., 2000; Nayak et al., 2018). To provide communities with a place to cool down during hot summer days, local agencies set up cooling centers, which are usually publicly available air-conditioned or cool recreation spaces (Nayak et al., 2017).
Cooling centers can be a valuable resource for heat-vulnerable populations without access to A/C or those who cannot afford them (Widerynski et al., 2017). This intervention is typically implemented as part of a larger heat response plan which can consist of a variety of activities such as health hot lines, a warning communication system (alerts and advisories), and emergency measures customized for a community or region (Toloo et al., 2013). Cooling centers are considered a relatively low-cost strategy to help reduce the impact of heat on health. They are intended to provide shelter to large groups of people during an EHE and can be easily implemented by local agencies and stakeholders using existing infrastructure and personnel.
Usually there is no single agency or organization that sets up cooling centers in a community; instead, a variety of stakeholders play a role in planning and implementing cooling centers. In NYS, several local agencies (municipalities, fire departments, library systems, county agencies and non-profit organizations like the American Red Cross) have set-up cooling centers over the past few years, as a heat-adaptation resource for their residents (Nayak et al., 2017; New York State Department of Health, 2017). Cooling centers are usually set up in/at facilities that are accessible to the public and can include libraries, senior and community centers, fairgrounds, recreation parks, malls and grocery stores. NYS counties without cooling centers have cited numerous reasons for not prioritizing cooling centers including the absence of heat events over the past several years, sparse population, understaffed or underfunded programs, and the availability of adequate green space and natural cool down resources (Nayak et al., 2017).
An assessment of the accessibility of cooling centers could provide local agencies with important information to help guide their heat adaptation planning in their jurisdictions (Widerynski et al., 2017). To our knowledge, there has been no previous effort to assess accessibility of cooling centers in NYS. Transportation-related factors have often been cited as barriers to visiting cooling centers (Lane et al., 2014; Toronto Public Health, 2011; Sampson et al., 2013). For instance, while urban areas have frequent and reliable public transportation that facilitate access to cooling centers, many smaller towns and rural areas have limited or no public transportation, thus limiting accessibility (American Public Transportation Association, 2017). Availability of transportation has been noted to impact utilization of health care services and frequency of visits to healthcare providers (Nemet and Bailey, 1982; Arcury et al., 2005; Mattson, 2011). Similarly, we believe that distance and availability of transportation to cooling centers can impact their utilization, as well as a community’s ability to adapt to heat and prevent heat-related illness. Therefore, our primary objective in this study was to assess the accessibility of the cooling centers to general and heat-vulnerable populations in rural and urban areas of NYS by various modes of transportation including walking, public transportation, and driving. Results from this study will be shared with local agencies to help inform them on the accessibility of cooling centers in the context of heat vulnerability and help make decisions when setting up cooling centers in preparation for future EHEs.
2. Methods
We assessed cooling center accessibility in terms of their proximity to the general and heat-vulnerable populations (Nayak et al., 2018) by various modes of transportation in New York State (excluding NYC). Based on the 2010 US Census Bureau data (United States Census Bureau, 2010), the study area included a population of 11,148,037 residents.
2.1. Data sources
Cooling center locations were obtained from information collected by a previous study (Nayak et al., 2017) surveying county health and emergency management offices across 57 NYS counties. Information included name, type, operational hours, physical address, and geographical coordinates of 377 reported cooling centers. Population estimates including population counts, geographical boundaries and centroid coordinates for census tracts in NYS (excluding NYC) were obtained from the 2010 US Census Bureau data (United States Census Bureau, 2010). Urbanicity of census tracts was defined based on secondary codes of the 2010 Rural-Urban Commuting Area (RUCA) (United States Department of Agriculture - Economic Research Service, 2016) Codes developed by the United States Department of Agriculture and the Categorization C method developed by WWAMI Rural Health Research Center (RHRC) (WWAMI RUCA Rural Health Research Center, 2004). Heat-vulnerable tracts were identified from the NYS Heat Vulnerability Index (HVI) developed by the New York State Department of Health (NYSDOH) (Nayak et al., 2018). To map vulnerability to heat, the census tract level HVI was constructed using socio-demographic variables including proportion of population that were elderly, elderly and living alone, unemployed, with a disability, foreign born, of low English proficiency, racial and ethnic minorities, with household income below poverty level, living in older homes, and environmental variables including housing density, proportion of tract area with high building intensity and open green space. Using principal component analysis, the variables were reduced into four components: social/language vulnerability, socioeconomic vulnerability, environmental/urban vulnerability, and elderly/elderly isolation. Component scores for each census tract ranged from 1 to 6, while the cumulative HVI scores ranged from 9 to 24. For our current accessibility analysis, heat-vulnerable tracts were defined by cumulative HVI scores of 15 and more. Public transportation data were obtained through the NYS Association of Metropolitan Planning Organizations (MPOs) (Hansen et al., 2011). Four NYS MPOs provided complete and geocoded data for the year 2014 including the Greater Buffalo-Niagara Regional Transportation Council; Syracuse Metropolitan Transportation Council; Capital District Transportation Committee and the Genesee Transportation Council. The data consisted of street address or street intersections and geographic coordinates of bus and ferry stops, and subway stations. Driving distances were computed using Google’s Distance Matrix Application Programming Interface (API) (Google Developers, 2017). The API is a web service that provides travel distance between multiple origins and destinations for a given mode of travel as calculated by Google Maps.
2.2. Study design and methods
In this cross-sectional study, we estimate the proximity of cooling centers to general and vulnerable populations and determine their accessibility via walking, public transit/transportation and driving. We used Occupational Safety and Health Administration’s (OSHA) Wet Bulb Globe Temperature (WBGT) calculator (Occupational Safety and Health Administration, 2016) to define accessible walking distance on an extreme hot day. Using the WBGT calculator for a sunny, summer day with air temperatures of 90 °F to 95 °F and relative humidity of 50%, OSHA recommends 25% work and 75% rest for a light work load, which translates to 15 min light work and 45 min rest per hour. OSHA’s ‘light’ work category is equivalent to a casual walking pace of 2 miles an hour (Occupational Safety and Health Administration), or 0.5 miles in the recommended 15 min. We therefore defined accessibility for general populations as 0.5 miles (walking distance) suggesting that ideally one should not have to walk more than 0.5 miles (15 min) to get to a cooling center or a public transportation stop.
Using census block population data, we determined geographical coordinates of population-weighted tract centroids that represent a point within the census tract where majority of the population resides. This point served as an aggregate approximation (Judge et al., 2012; Boscoe et al., 2012; Bliss et al., 2012) for residential addresses, so all residents within a tract will share the centroid coordinates as their residential location. Geocoded cooling center locations were mapped to overlay 2010 US Census tracts using MapInfo© v15.2. General population proximity was determined using the MapInfo© 15.2 Distance Calculator tool to estimate 1) distance between census tract centroid and nearest cooling center; and 2) percent of census tract population within walking-distance (0.5 miles) of a cooling center. Similarly, proximity to heat-vulnerable populations was measured by distance between heat-vulnerable tract centroids and the nearest cooling center.
We classified census tracts of NYS (excluding NYC) into urban and rural groups based on their RUCA codes (United States Department of Agriculture - Economic Research Service, 2016) and the Categorization C method developed by WWAMI (WWAMI RUCA Rural Health Research Center, 2004). By this classification, approximately 90% of NYS census tracts were classified as “Urban”. The remainder of tracts were categorized as “Rural” and consisted of an aggregation of large, small and small isolated rural cities and towns. This method of classification is similar to the United States Office of Management and Budget delineation that splits areas into metropolitan and micropolitan but at the sub county-level.
Accessibility by mode of travel was assessed in terms of public transportation for urban areas where transportation data was available and in terms of driving in rural areas. Public transportation is often available in urban areas, so accessibility to cooling centers in these areas was assessed by their proximity to public transportation stops. The stops in the four MPO regions were geocoded at street level and accessibility via public transportation was determined by distance between cooling centers and the nearest public transportation stop. Straight-line or Euclidean distance calculations between population centroids, public transportation stops, and cooling centers were computed using the distance calculator tool on MapInfo© 15.2. We used straight-line distance for this assessment as it has been found to correspond closely to travel distance in urban areas (Boscoe et al., 2012; Bliss et al., 2012; Jones et al., 2010)and difference between straight-line and driving estimates are generally inconsequential for non-emergency travel (Boscoe et al., 2012).
Driving distances were computed to assess accessibility of cooling centers in rural areas where public transportation can be infrequent or unavailable. Distances between the population-weighted, heat-vulnerable rural census tract centroids and the nearest cooling center were calculated using SAS 9.4 (Zdeb, 2010) and the Google Distance Matrix API (Google Developers, 2017). According to the US Census Bureau 2009–2013 American Community Survey, average daily commuting time in metro- and micropolitan areas of NYS ranges from 19 to 36 min. This averages to 18 miles (at a speed of 45 mph) which we used to define as accessible distance for cooling centers in rural areas. Distances were computed between noon and 6 p.m., which is when people are more likely to visit a cooling center (Maricopa County Department of Public Health, 2015). This 6-h window also overlaps with periods of expected maximum daytime temperatures in the summer (3 p.m.–6 p.m.).
Exclusions: Due to the unavailability of cooling center information for the five counties of NYC this analysis excludes NYC. Census tracts with zero population, missing HVI or component scores, and missing/unknown RUCA codes were also excluded from analysis.
3. Results
Characteristics:
Cooling centers were primarily located in urban areas (97%) and all indoor facilities had A/C. Sites that housed or served as cooling centers included public libraries (35%), followed by community and senior centers (28%), and recreational sites (11%) such as swimming pools, park and beaches. The remaining cooling centers were located in local government buildings (town halls, court houses), town fire departments, schools, shopping centers and American Red Cross offices. Around 95% of the cooling centers were open for at least 4 h between 9 a.m. and 4 p.m. from Monday to Friday with 40% having extended hours up to 6 p.m. About 1% were up to 10 p.m. and none were open overnight. About 75% of indoor facilities and 100% of outdoor facilities were open for 4 h or more on weekends.
Proximity to overall population:
Straight-line distances between census tract populations (centroids) and the nearest cooling center ranged from 0 to 53.2 miles with furthest distances observed in the northern census tracts of NYS (Fig. 1 and Table 1a). Approximately one-third of the census tracts were within a walking distance (i.e., 0.5 miles) of a cooling center (Table 1a) with average and median distances of 3.84 and 1.34 miles, respectively. About 45% of the study population were two miles or farther from the nearest cooling center.
Fig. 1.

Distance between census tracts and nearest cooling center in New York State (excluding New York City).
Table 1a.
Distance between general and vulnerable populations and nearest cooling center.
| Distance to nearest cooling center (miles) | NYS Census tractsa | Heat-Vulnerable tractsb | ||||||
|---|---|---|---|---|---|---|---|---|
|
| ||||||||
| N | Population (%) | Average Distance (miles) | Median Distance (miles) | N | Population (%) | Average Distance (miles) | Median Distance (miles) | |
|
| ||||||||
| Total | 2723 | 11,148,037 | 3.84 | 1.34 | 961 | 3,682,132 | 2.43 | 0.46 |
| < 0.1 | 475 | 1,913,326 (17.2) | 0.01 | 0 | 244 | 903,895 (24.6) | 0.01 | 0 |
| 0.1– < 0.5 | 431 | 1,613,189 (14.5) | 0.28 | 0.27 | 250 | 869,196 (23.6) | 0.28 | 0.27 |
| 0.5– < 1.0 | 311 | 1,245,506 (11.2) | 0.71 | 0.70 | 119 | 431,943 (11.7) | 0.70 | 0.68 |
| 1– < 2 | 338 | 1,401,588 (12.6) | 1.44 | 1.41 | 99 | 400,999 (10.9) | 1.44 | 1.43 |
| > = 2 | 1168 | 4,974,428 (44.6) | 8.24 | 5.03 | 249 | 1,076,099 (29.2) | 8.16 | 4.11 |
NYS population excluding NYC.
Heat-vulnerable tracts: Heat vulnerability Index (HVI) Score ≥ 15.
Proximity to heat-vulnerable populations:
Approximately one-third of NYS population excluding NYC live in the 961 heat-vulnerable census tracts (HVI scores ≥ 15). As seen in Table 1a, over 50% of heat-vulnerable tracts were within walking distance of a cooling center, with more than half of these tracts within 0.1 miles. The farthest distances to cooling centers were seen in heat-vulnerable tracts in northern NYS with maximum distance of 53.2 miles. About 26% of heat-vulnerable tracts were 2 miles or farther from a cooling center. Comparison of distances across vulnerability components showed that approximately 34–42% of population in vulnerable tracts (component scores ≥ 4) were within 0.5 miles of a cooling center (Table 1b). Census tracts where vulnerability to heat was due to high proportions of elderly populations and socio-economically disadvantaged populations were observed with larger distances (4.5–4.7 miles) in comparison to tracts vulnerable to heat due to characteristics of urbanicity (open green space, building intensity, housing density and age of home) that were observed to average less than 2 miles.
Table 1b.
Distance between vulnerable tracts by vulnerability component.
| Heat Vulnerability Index (HVI) and Components | Heat-vulnerable tractsa | Vulnerable Tracts < 0.5 miles, N (%) | Total Population | Percent Population < 0.5 miles | Distance to nearest cooling center (miles) | |
|---|---|---|---|---|---|---|
|
|
||||||
| Average | Median | |||||
|
| ||||||
| Cumulative HVI | 961 | 494 (51.4%) | 3,682,132 | 48.2 | 2.43 | 0.46 |
| Factor 1-Language | 898 | 366 (40.8%) | 3,997,812 | 38.0 | 2.83 | 0.87 |
| Factor 2-Socio-economic | 1096 | 480 (43.8%) | 4,010,092 | 41.9 | 4.71 | 0.74 |
| Factor 3-Urban | 1367 | 596 (43.6%) | 5,374,005 | 40.2 | 1.94 | 0.70 |
| Factor 4-Elderly | 1209 | 419 (34.6%) | 4,797,244 | 34.2 | 4.47 | 1.18 |
Heat-vulnerable tracts defined as tracts with Cumulative HVI Score ≥ 15 or Component scores ≥ 4.
Proximity by urbanicity:
Table 2 summarizes the distance between urban and rural census tracts and the nearest cooling center. Average and median distances from urban tracts to cooling centers were 2.93 miles and 1.17 miles (range 0–53.2 miles) while average and median distance from rural tracts were 11.63 miles and 5.38 miles (range 0–38.8 miles). About 35% of urban and 21% of rural census tracts were within 0.5 miles of a cooling center. Chi-square test showed the proportion of urban tracts were significantly higher than proportions that of rural tracts in distance categories within 2 miles of a cooling center (results not shown). Larger proportions of rural residents (66%) live 2 or more miles from a cooling center in comparison to urban residents (42%).
Table 2.
Distance (miles) between urban and rural populations and nearest cooling center.
| Distance to nearest cooling center (miles) | Urban tractsa | Rural tractsa | ||||||
|---|---|---|---|---|---|---|---|---|
|
| ||||||||
| N | Population (%) | Average Distance (miles) | Median Distance (miles) | N | Population (%) | Average Distance (miles) | Median Distance (miles) | |
|
| ||||||||
| Total | 2425 | 10,033,179 | 2.93 | 1.17 | 286 | 1,059,559 | 11.63 | 5.32 |
| < 0.1 | 438 | 1,776,708 (17.7%) | 0.01 | 0 | 35 | 129,285 (12.2%) | 0.02 | 0 |
| 0.1– < 0.5 | 406 | 1,510,222 (15.1%) | 0.28 | 0.28 | 24 | 98,961 (9.3%) | 0.26 | 0.22 |
| 0.5– < 1.0 | 294 | 1,179,350 (11.8%) | 0.71 | 0.69 | 15 | 54,540 (5.2%) | 0.76 | 0.78 |
| 1– < 2 | 313 | 1,316,310 (13.1%) | 1.44 | 1.39 | 24 | 84,594 (7.9%) | 1.58 | 1.57 |
| > = 2 | 974 | 4,250,589 (42.4%) | 6.50 | 4.67 | 188 | 692,179 (65.3%) | 17.39 | 11.38 |
As defined by WWAMI Rural Health Research Center Categorization C.
Urban Area Cooling Center Accessibility via Public Transportation:
Over 22,000 public transportation stops were geocoded in the four MPOs covering 16 largely urban NYS counties (1031 census tracts). Fig. 2 displays the mapped public transportation stops and cooling centers (n = 170) overlaying 399 heat-vulnerable tracts in the four MPO regions. About 170 (45% of all) cooling centers were located in these four regions (Table 3). Distance between cooling centers and the nearest public transportation stop across these regions ranged from 0 to 13.1 miles with an average distance of 1.1 miles. Approximately 80% of the cooling centers were within walking distance of a public transportation stop, furthest distance was seen in the Greater Buffalo-Niagara Regional Transportation Council (GBNRTC). Distances computed from cooling centers in heat-vulnerable tracts to public transportation stops showed that 100% of the cooling centers were within walking distance of a public transportation stop.
Fig. 2.
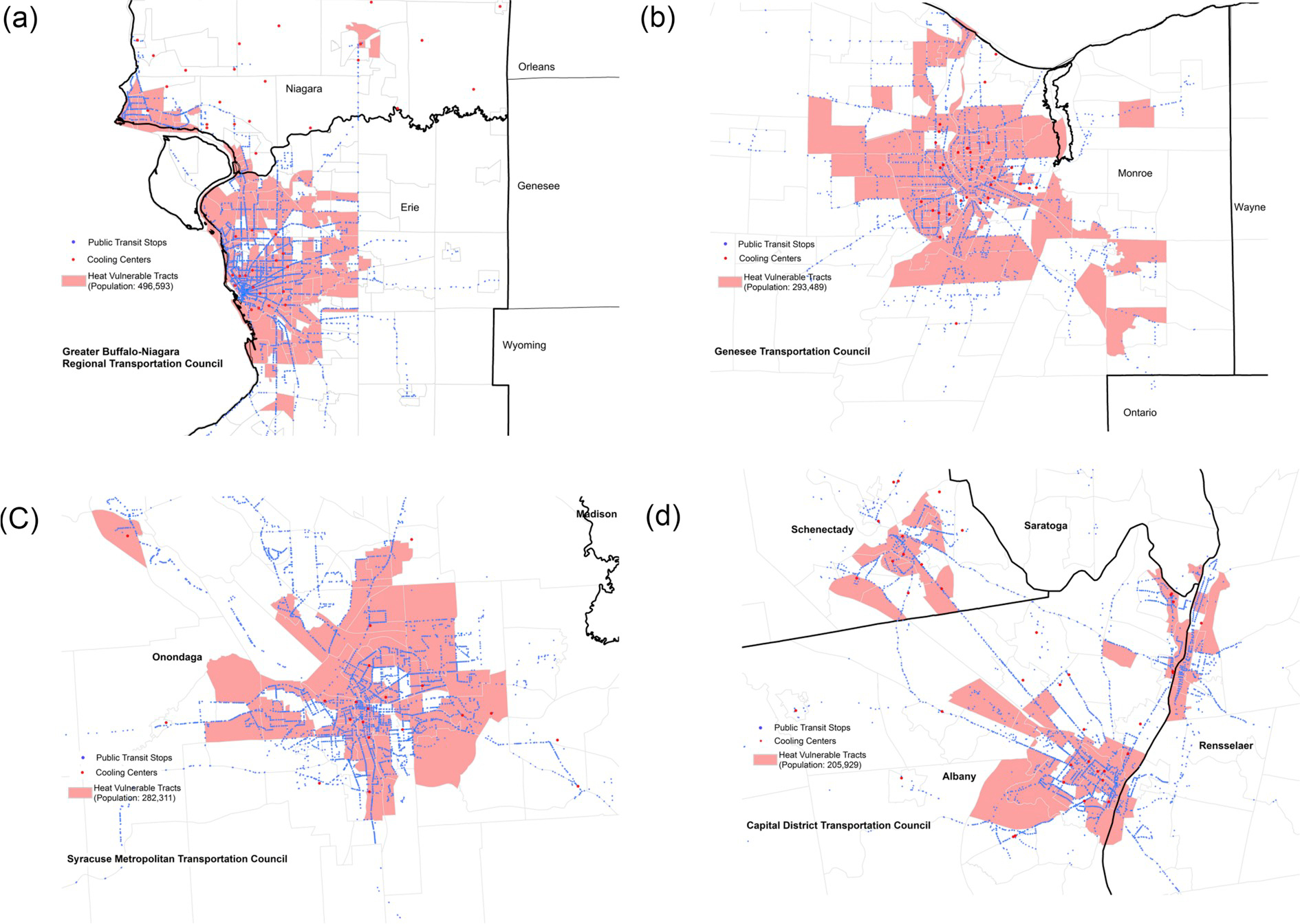
a–d. Heat-vulnerable tracts, cooling centers and public transportation stops in Metropolitan Planning Organization (MPO) regions in NYS.
Table 3.
Distance between tracts, cooling centers and nearest public transportation stop in the 4 Metropolitan Planning Organization (MPO) regions.
| Greater Buffalo-Niagara Regional TCa | Genesee TCa | Syracuse Metropolitan TCa | Capital District TCa | |
|---|---|---|---|---|
|
| ||||
| Population in MPO | 1,135,971 | 942,726 | 906,204 | 893,972 |
| Population in heat-vulnerable tracts | 43.7% | 31.1% | 31.2% | 23.0% |
| Accessibility of cooling centers via public transportation | ||||
| Number of cooling centers | 52 | 38 | 34 | 46 |
| Distance (miles) from cooling centers to nearest public transportation stop | ||||
| Mean (Range) | 2.78 (0, 13.1) | 0.16 (0, 2.3) | 0.50 (0, 11.7) | 0.39 (0, 4.9) |
| Median | 0.4 | 0.07 | 0.03 | 0.05 |
| Number of cooling centers by distance to nearest public transportation stop N (%) | ||||
| 0 to < 0.5 miles | 26 (50.0) | 36 (94.7) | 31 (91.2) | 42 (91.3) |
| 0.5 to < 1 mile | 4 (7.7) | 1 (2.6) | 1 (2.9) | 1 (2.2) |
| > = 1 mile | 22 (42.3) | 1 (2.6) | 2 (5.9) | 3 (6.5) |
| Number of cooling centers in heat-vulnerable tracts by distance to nearest public transportation stop N (%) | ||||
| 0 to < 0.5 miles | 19 (100) | 22 (100) | 20 (100) | 19 (100) |
| Public transportation accessibility to census tracts | ||||
| Number of census tracts | 294 | 238 | 260 | 226 |
| Census tracts by distance (miles) to nearest public transportation stop | ||||
| Mean (Range) | 0.49 (0, 12.4) | 0.51 (0, 12.3) | 1.04 (0, 16.5) | 0.66 (0, 18.2) |
| Median | 0 | 0 | 0 | 0 |
| Number of heat-vulnerable tracts by distance to nearest public transportation Stop N (%) | ||||
| 0 to < 0.5 miles | 148 (98.7) | 93 (100) | 94 (98.9) | 61 (100) |
| 0.5 to < 1 mile | 1 (0.7) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| > = 1 mile | 1 (0.7) | 0 (0.0) | 1 (1.1) | 0 (0.0) |
TC = Transportation Council.
Distances from census tracts in the four MPO regions to the nearest public transportation stop showed average distances of 0.49–0.66 miles (Range: 0 to 18.2 miles) (Table 3). About 60% of census tracts and nearly all heat-vulnerable tracts (99–100%) in the four metro regions were within walking distance of a public transportation stop, with distance averaging at 0.04 miles (Range: 0 to 9.82 miles, data not shown).
Rural Area Cooling Center Accessibility via driving:
Forty-two census tracts across 20 counties were identified as rural tracts that were heat-vulnerable (Nayak et al., 2018). Straight-line distances ranged from 0 to 38.8 miles while driving distances were observed to range from 0.6 to 58.7 miles (median = 9.85; mean = 18.3 miles) (Table 4) with less than 10% of the rural heat-vulnerable census tracts within 2 miles driving distance and about 56% within the study-defined accessible driving distance of 18 miles of a rural heat-vulnerable census tract. Driving distance computations showed that the nearest identified cooling center by driving was also the nearest cooling center identified by straight-line distance. However, driving distances were of a significantly larger magnitude and these differences ranged from 0.6 to 27.2 miles. Largest differences between the two measures were seen in the most rural areas of Essex and Warren counties.
Table 4.
Comparison of Straight-line and Driving distances in Rural Heat-vulnerable Tracts.
| Driving distance (miles) | Straight-line distance (miles) | |
|---|---|---|
|
| ||
| Range | 0.6 to 58.7 | 0 to 38.8 |
| Median (IQR) | 9.85 (20.80) | 7.18 (19.07) |
| Mean (SD) | 18.28 (17.08) | 11.73 (12.54) |
| <=18 miles | 25 (56%) | 31 (71%) |
| Difference between distance measurements (miles) | ||
| Mean Difference (SD) | 7.17 (6.36) | |
| Median Difference (IQR) | 5.18 (6.95) | |
| Rural heat-vulnerable tracts (%) | ||
| < 3 miles difference | 12 (28.6) | |
| 3–6 miles difference | 12 (28.6) | |
| > 6 miles difference | 18 (42.8) | |
4. Discussion
In this study, we estimated cooling center accessibility in terms of distance from urban, rural and heat-vulnerable NYS residents to the nearest cooling center by walking, public transportation, or driving.
Cooling centers were observed to be primarily located in urban areas. Despite the largely urban distribution of cooling centers, only about one-third of NYS population (excluding NYC) was within walking distance of a cooling center. However, accessibility of cooling centers from heat-vulnerable tracts was considerably higher with almost 50% of heat-vulnerable population within walking distance of a cooling center. About 20% of homes in NYS do not have A/C (US Energy Information Administration, 2009) so accessibility to cooling centers during EHEs could significantly reduce the impact of heat in vulnerable populations, especially among those who do not have access to A/C.
In the four metropolitan areas that provided transportation data, about 80% of cooling centers overall, and 100% of those in heat-vulnerable tracts were within walking distance of a public transportation stop. In addition, almost all heat-vulnerable tracts had a public transportation stop within walking distance, showing that cooling center accessibility improved once public transportation was considered in these four metropolitan areas. Urban areas tend to have high building density and less green space so accessibility to A/C and cooling centers could be crucial in protecting urban populations. It is therefore noteworthy that cooling centers in our study are largely accessible by walking or public transportation to those residing in heat-vulnerable tracts in urban areas. We also observed that cooling centers in Niagara county within the GBNRTC had the longest distances from public transportation and the smallest proportion of cooling centers that were accessible via public transportation. Our findings are consistent with the Western New York Community Health Needs Assessment which found that public transit was weak or non-existent outside of major cities in that region (New York State Department of Health Centers for Medicare and Medicaid Services, 2014). Lack of transportation has often been cited as a barrier to visiting cooling centers (Lane et al., 2014; Toronto Public Health, 2011; Sampson et al., 2013). If provision of public transportation encourages use of cooling centers, as found in studies assessing the role of transportation in healthcare service utilization (Mattson, 2011), communities could potentially see a reduction in heat distress calls with a corresponding cost benefit from reduced heat-related hospitalizations. While many jurisdictions across the state provide transportation or ensure public transportation is available to cooling centers during heat events (Nayak et al., 2017), there is currently no information on use of transportation to get to cooling centers in NYS. Other states and local agencies providing transportation to cooling centers have noted that factors like cost of bus fare, having to wait at a bus stop, absence of A/C during the ride, long distances, and prolonged time due to multiple stops can be deterrents from using public transportation to visit cooling centers (Sampson et al., 2013; New York State Department of Health Centers for Medicare and Medicaid Services, 2014; Berisha et al., 2016; White-Newsome et al., 2014). One study noted that even though public transportation was available, the cooling centers were not on the direct route (White-Newsome et al., 2014). Therefore, besides the availability of transportation, these are important considerations to address towards improving cooling center utilization during a heat event. Unawareness of cooling center locations and public transportation schedules can hinder utilization. Therefore, to help the public find a cooling center near them, the NYSDOH has developed an interactive mapping application (New York State Department of Health, 2014) which allows residents to locate cooling centers near them during the summer. The mapping application provides the user with cooling center contact information, street address, directions (walking and driving), as well as timing and route information of the next scheduled bus where transportation is available.
Far fewer rural residents live within accessible distance of a cooling center than urban residents. Driving distance to cooling centers as we observed can be longer than in urban areas and public transportation could be limited (American Public Transportation Association, 2017). Our finding is consistent with rural area studies where long distances to access to healthcare and benefits is a major concern as population density decreases and geographic isolation increases (New York State Department of Health Centers for Medicare and Medicaid Services, 2014; Jones et al., 2009; Stanford Medicine). Although the overall rural population in the US is declining, ridership via public transportation in rural areas has increased (American Public Transportation Association, 2017). However, only a handful of counties (13%) in NYS have reported provision of public transportation to cooling centers (Nayak et al., 2017) so, increasing availability and frequency of transportation to cooling centers during hot days can help improve accessibility in these areas. Rural areas often do not have air-conditioned homes (Matz et al., 2015) or cooling centers for numerous reasons including the rarity of EHEs in these areas (Nayak et al., 2017). These upstate areas in NYS experience lower baseline temperatures relative to other areas in the state (Horton et al., 2014; Rosenzweig et al., 2011) and although rare, in the event of an EHE, rural residents may not be prepared to handle the heat. However, it is likely that these areas have other resources like local and state parks where people can cool off. Although rural area residents are likely to own a vehicle, local agencies are encouraged to provide rural area residents with cool-down resources in the community and provide transportation to these resources to maximize their use. Air-conditioned transportation could serve as both a means to get to a cooling center as well as a means to cool down while doing so. This could also considerably improve access among individuals that have limited mobility or no other means of transportation.
To the best of our knowledge, this is the only study that has assessed cooling center accessibility in terms of heat-vulnerable populations and modes of transportation in NYS. However, there are some limitations in our study. We restricted our analysis to cooling centers that were reported by local agencies at the start of the warmer season in NYS. Our database therefore does not include additional locations that were set up as cooling centers briefly for the duration of an EHE. This leads to the possibility of some overestimation of distance to nearest cooling center but we do not expect significant differences as we have not been notified of many changes in the locations during the summer season in NYS (New York State Department of Health, 2014). Estimating distances from census tract centroids instead of specific residential addresses could be considered as another limitation of this study. But centroids are commonly used as an aggregate approximation of residential addresses (Judge et al., 2012; Boscoe et al., 2012; Bliss et al., 2012). To further improve proximity to residential population we used population-weighted centroids, which take account of population location and can give a more relevant measurement of distance (Luo and Wang, 2003; Hwang and Rollow, 2000). Another limitation in distance calculations may be the use of straight-line measurements. Although ideal, driving distance estimations from the approximately 8.1 million housing units in NYS are resource- and time-intensive. Straight-line distance estimations in urban areas have been found to be reasonable proxies for walking distance and have been noted to be relatively comparable to distance computed via Google Maps (Boscoe et al., 2012; Bliss et al., 2012). We noted larger differences in distances computations in rural areas, but our findings by both methods demonstrate that only a small proportion of the population was within accessible distance of a cooling center. We were unable to determine accessibility of cooling centers via other transportation options including ride-shares, taxis and community shuttles due to the lack of data on schedules and utilization of these services for individual requests. Such data would be difficult to obtain from private taxi companies and the only recently available ride-share services across the state. Results from a survey of local agencies in NYS (Nayak et al., 2017) showed that some cooling centers provide shuttle services on request or as needed during a heat event. Pick up locations and frequency of shuttles would depend on requests the cooling center receives and that could vary daily. But even in these instances, data are difficult to obtain. We believe that exclusion of these data does not affect our study findings as we are estimating accessibility in terms of distance, and there would be no difference between owner-driven or taxis or ride-share vehicles.
To prevent heat-related illness, a common recommendation for immediate heat relief is to spend a few hours in an air-conditioned place. Towards this recommendation, the NYS Office of Temporary Disability Assistance offers cooling assistance benefits to enable eligible NYS residents to obtain an air-conditioner unit or fan during the summer to cool down their homes (Office of Temporary and Disability Assistance (OTDA), 2018). But many households may not be aware of the program or may not meet the eligibility criteria. Therefore, setting up cooling centers during EHEs can be an effective strategy to reduce or prevent heat-related morbidities and mortalities, specifically among heat-vulnerable populations with limited access to A/C (Widerynski et al., 2017). While existing air-conditioned facilities such as shopping malls or libraries can easily be utilized as cooling centers and impose minimal economic burden on individuals, accessibility factors including distance from cooling centers and lack of transport can influence utilization of these resources (Sampson et al., 2013; Berisha et al., 2016; White-Newsome et al., 2014; Sheridan, 2007). The provision of safe, reliable and affordable transportation to cooling centers during hot days and heat events can overcome these barriers (Widerynski et al., 2017). A simple preventive measure such as spending a few hours in an air-conditioned environment such as a cooling center or even air-conditioned transportation can provide reprieve from the heat outdoors and result in a significant reduction in heat-related emergency room visits and hospitalizations in a community (Madrigano et al., 2000; Rosenthal et al., 2014; Uejio et al., 2011; Ostro et al., 2010; Widerynski et al., 2017; Sampson et al., 2013). This accessibility assessment was performed with the goal to provide health officials with information needed for heat preparedness plans. Knowledge about vulnerable populations that may have difficulty accessing cooling centers due to restricted mobility, vehicle ownership, distance issues or lack of public transportation can aid local health officials in program planning during EHEs. In these situations, cooling centers can be set up in heat-vulnerable areas, and free or affordable transportation can be provided as needed.
In this study, we assessed accessibility in terms of geographic proximity to cooling centers but there are several other reasons why they may not be accessible or utilized. People may prefer to cool off at places that are not official cooling centers like a local eatery or a relative’s house, but we are unable to capture this information without a survey tool. Utilization of a cooling center or reasons for non-utilization, will be explored as a next step, using a survey instrument that can help understand these and other behavioral aspects not explored in this study.
5. Conclusions
The accessibility assessment in this study focused on cooling center proximity to general and heat-vulnerable populations and accessibility via different modes of transportation in NYS. Spatial patterns of accessibility varied substantially across the state. Within the four metropolitan areas, while many residents are not within walking distance of a cooling center, most, and nearly all in the most heat-vulnerable areas, are within walking distance of public transportation to a cooling center. In rural locations, where there may be less of a critical need for cooling centers due to other options for cooling off, distances are longer, and accessibility is a greater issue. Availability and awareness of affordable, reliable and convenient transportation that integrate accommodation for people with disabilities play key roles in cooling center utilization and can thereby significantly reduce the impact of heat on health in the state. This said, there are several other factors that influence the utilization of these facilities during heat events including poor health, disability, unawareness of risk, unavailability of transportation and the preference to stay at home even though it’s hot. In many of these situations, having A/C at homes can help residents find relief from the heat, even at night, when cooling centers are not open. But as the next best alternative to A/C at home, the benefits of cooling centers should be maximized to the public. Recognizing that lack of awareness of cooling centers and transportation can impede utilization, to help prevent and reduce heat-related illness, the NYSDOH developed the interactive mapping application for NYS residents to locate cooling centers near them and obtain timing and route information of the next scheduled public transportation where available. While cooling centers are an important component of heat adaptation, they are most effective to vulnerable populations when implemented along with other components of heat response including transportation, heat alerts, and cooling assistance programs. Overall, it is therefore, important for health officials to address barriers to cooling center utilization in their heat preparedness plans, by considering the HVI as a factor in where cooling centers should be, as well as improving cooling center accessibility for heat-vulnerable populations.
Acknowledgements
We would like to thank four transportation councils of the New York State Association of Metropolitan Planning Organizations including the Greater Buffalo-Niagara Regional Transportation Council (GBNRTC); Syracuse Metropolitan Transportation Council (SMTC); Capital District Transportation Committee (CDTC) and the Genesee Transportation Council (GTC) for their valuable assistance with public transportation data.
Funding information
Work on this project was supported in part by grants from the New York State Energy Research and Development Authority and the National Environmental Public Health Tracking Program, Centers for Disease Control and Prevention
Footnotes
Conflict of interest
The authors declare that they have no conflict of interest.
IRB approval
IRB approval was obtained through New York State Department of Health Institutional Review Board, Albany, NY as per organizational protocol. No confidential information was collected during this study.
References
- American Public Transportation Association, 2017. Public Transportation’s Impact on Rural and Small Towns. A Vital Mobility Link. American Public Transportation Association (APTA). [Google Scholar]
- Arcury TA, Preisser JS, Gesler WM, Powers JM, 2005. Access to transportation and health care utilization in a rural region. J. Rural Health : official journal of the American Rural Health Association and the National Rural Health Care Association 21, 31–38. [DOI] [PubMed] [Google Scholar]
- Berisha V, Hondula D, Roach M, White JR, McKinney B, Bentz D, Mohamed A, Uebelherr J, Goodin K, 2016. Assessing adaptation strategies for extreme heat: a public health evaluation of cooling centers in maricopa county, Arizona. Weather, Climate, and Society 9, 71–80. 10.1175/WCAS-D-16-0033.1. [DOI] [Google Scholar]
- Bliss RL, Katz JN, Wright EA, Losina E, 2012. Estimating Proximity to Care: are straight line and zipcode centroid distances acceptable proxy measures? Med. Care 50, 99–106. 10.1097/MLR.0b013e31822944d1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Boscoe FP, Henry KA, Zdeb MS, 2012. A nationwide comparison of driving distance versus straight-line distance to hospitals. Prof. Geogr. : the journal of the Association of American Geographers 64. 10.1080/00330124.2011.583586. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Google Developers, 2017. Google distance Matrix API-Developers guide. 2018. https://developers.google.com/maps/documentation/distance-matrix/start.
- Hansen A, et al. , 2011. Perceptions of heat-susceptibility in older persons: barriers to adaptation. Int. J. Environ. Res. Public Health 8, 4714–4728. 10.3390/ijerph8124714. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Horton RM, Bader DA, Rosenzweig C, DeGaetano AT, Solecki W, 2014. Climate Change in New York State: Updating the 2011 ClimAID Climate Risk Information Supplement to NYSERDA Report 11–18. (Responding to Climate Change in New York State). [Google Scholar]
- Hwang H-L, Rollow J, 2000. Data Processing Procedures and Methodology for Estimating Trip Distances for the 1995 American Travel Survey (ATS).
- Jones CA, Parker TS, Ahearn M, Mishra AK, Variyam JN, 2009. Health Status and Health Care Access of Farm and Rural Populations. U.S. Dept. of Agri., Econ. Res. Serv. [Google Scholar]
- Jones SG, Ashby AJ, Momin SR, Naidoo A, 2010. Spatial implications associated with using euclidean distance measurements and geographic centroid imputation in health care Research. Health Serv. Res. 45, 316–327. 10.1111/j.1475-6773.2009.01044.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Judge A, et al. , 2012. Inequalities in rates of renal replacement therapy in England: does it matter who you are or where you live? Nephrol. Dial. Transplant. 27, 1598–1607. 10.1093/ndt/gfr466. [DOI] [PubMed] [Google Scholar]
- Lane K, et al. , 2014. Extreme heat awareness and protective behaviors in New York City. J. Urban Health : Bull. N. Y. Acad. Med. 91, 403–414. 10.1007/s11524-013-9850-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lu Y, Lin S, Sheridan S, Radigan A, Nguyen T, Nayak SG, 2017. Society for Epidemiologic Research, Seattle, WA. [Google Scholar]
- Luo W, Wang F, 2003. Measures of spatial accessibility to health care in a GIS environment: synthesis and a case study in the chicago region. Environ. Plan. Plan. Des. 30, 865–884. 10.1068/b29120. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Madrigano J, Ito K, Johnson S, Kinney PL & Matte T A case-only study of vulnerability to heat wave-related mortality in New York city (2000–2011). Environ. Health Perspect. 123, 672–678, doi: 10.1289/ehp.1408178 (2015). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Maricopa County Department of Public Health, 2015. Facility Manager Survey Results in Maricopa County Cooling Center Evaluation Project in Collaboration with Arizona State. University and Arizona Department of Health Services. [Google Scholar]
- Mattson J, 2011. Transportation, distance, and health care utilization for older adults in rural and small urban areas. Transportation Research record. Journal of the Transportation Research Board 2265, 192–199. 10.3141/2265-22. [DOI] [Google Scholar]
- Matz CJ, Stieb DM, Brion O, 2015. Urban-rural differences in daily time-activity patterns, occupational activity and housing characteristics. Environ. Health 14, 88. 10.1186/s12940-015-0075-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nayak SG, et al. , August 2018. Development of a heat vulnerability index for New York State. Publ. Health 161, 127–137. 10.1016/j.puhe.2017.09.006. [DOI] [PubMed] [Google Scholar]
- Nayak SG, et al. , 2017. Surveying local health departments and county emergency management offices on cooling centers as a heat adaptation resource in New York state. J. Community Health 42, 43–50. 10.1007/s10900-016-0224-4. [DOI] [PubMed] [Google Scholar]
- Nemet GF, Bailey AJ, 1982. Distance and health care utilization among the rural elderly. Soc. Sci. Med. 50, 1197–1208 2000. [DOI] [PubMed] [Google Scholar]
- New York State Department of Health, 2017. Cooling centers. https://apps.health.ny.gov/statistics/environmental/public_health_tracking/tracker/#/CCMap.
- New York State Department of Health, 2018. County Heat and Health Profile Reports. New York State Department of Health., Albany, NY. [Google Scholar]
- New York State Department of Health Centers for Medicare and Medicaid Services, 2014. Western New York Community Health Needs Assessment. (Delivery System Reform Incentive Payment (DSRIP) Program. [Google Scholar]
- Occupational Safety and Health Administration. Using the Heat Index: A Guide for Employers.
- Occupational Safety and Health Administration, 2016. OSHA technical manual. Heat stress. Heat hazard assessment. https://www.osha.gov/dts/osta/otm/otm_iii/otm_iii_4.html#step1_optionb. [Google Scholar]
- Office of Temporary and Disability Assistance (OTDA), 2018. Home Energy assistance program (HEAP) cooling assistance benefit. https://otda.ny.gov/programs/heap/#cooling-assistance.
- Ostro B, Rauch S, Green R, Malig B, Basu R, 2010. The effects of temperature and use of air conditioning on hospitalizations. Am. J. Epidemiol. 172, 1053–1061. 10.1093/aje/kwq231. [DOI] [PubMed] [Google Scholar]
- Rosenthal JK, Kinney PL, Metzger KB, 2014. Intra-urban Vulnerability to Heat-Related Mortality in New York City, 1997–2006, vol. 30. Health & place, pp. 45–60. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rosenzweig C, et al. , 2011. Responding to Climate Change in New York State: the ClimAID Integrated Assessment for Effective Climate Change Adaptation. Albany, New York. [DOI] [PubMed] [Google Scholar]
- Sampson NR, et al. , 2013. Staying cool in a changing climate: reaching vulnerable populations during heat events. Glob. Environ. Chang. : human and policy dimensions 23, 475–484. 10.1016/j.gloenvcha.2012.12.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sheridan SC, 2007. A survey of public perception and response to heat warnings across four North American cities: an evaluation of municipal effectiveness. Int. J. Biometeorol. 52, 3–15. 10.1007/s00484-006-0052-9. [DOI] [PubMed] [Google Scholar]
- Sheridan SC, Allen MJ, 2018. Temporal trends in human vulnerability to excessive heat. Environ. Res. Lett. 13 043001. [Google Scholar]
- Stanford Medicine. Healthcare Disparities & Barriers to Healthcare, Accessed 2018.
- Toloo GS, FitzGerald G, Aitken P, Verrall K, Tong S, 2013. Are heat warning systems effective? Environ. Health 12, 27. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Toronto Public Health, 2011. Protecting vulnerable people from health impacts of extreme heat. https://www.toronto.ca/legdocs/mmis/2011/hl/bgrd/backgroundfile-39469.pdf.
- Uejio CK, et al. , 2011. Intra-urban societal vulnerability to extreme heat: the role of heat exposure and the built environment, socioeconomics, and neighborhood stability. Health Place 17, 498–507. 10.1016/j.healthplace.2010.12.005. [DOI] [PubMed] [Google Scholar]
- United States Census Bureau, 2010. Summary file. 2006 – 2010 American community survey. https://www.census.gov/2010census/data/.
- United States Department of Agriculture - Economic Research Service, 2016. Rural-urban commuting area codes. https://www.ers.usda.gov/data-products/rural-urban-commuting-area-codes/.
- United States Environmental Protection Agency, 2016. Climate Change Indicators in the United States. Heat-Related Deaths, vols. 60–64 U.S. EPA. [Google Scholar]
- United States Natural Hazard Statistics, 2017a. Weather fatalities 2017. http://www.nws.noaa.gov/om/hazstats.shtml.
- United States Natural Hazard Statistics, 2017b. Heat related fatalities. http://www.nws.noaa.gov/os/hazstats/heat05.pdftohttp://www.nws.noaa.gov/os/hazstats/heat16.pdf.
- US Energy Information Administration, 2009. Household Energy Use in New York. US Energy Information Administration, Washington DC. [Google Scholar]
- White-Newsome JL, et al. , 2014. Strategies to reduce the harmful effects of extreme heat events: a four-city study. Int. J. Environ. Res. Public Health 11, 1960–1988. 10.3390/ijerph110201960. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Widerynski S, et al. , 2017. The Use of Cooling Centers to Prevent Heat-Related Illness: Summary of Evidence and Strategies for Implementation. Centers for Disease Control and Prevention. [Google Scholar]
- WWAMI RUCA Rural Health Research Center, 2004. RUCA data: using RUCA data. http://depts.washington.edu/uwruca/ruca-uses.php.
- Zdeb M, 2010. Driving distances and times using SAS® and Google maps. http://support.sas.com/resources/papers/proceedings10/050-2010.pdf.