
Figure 1.
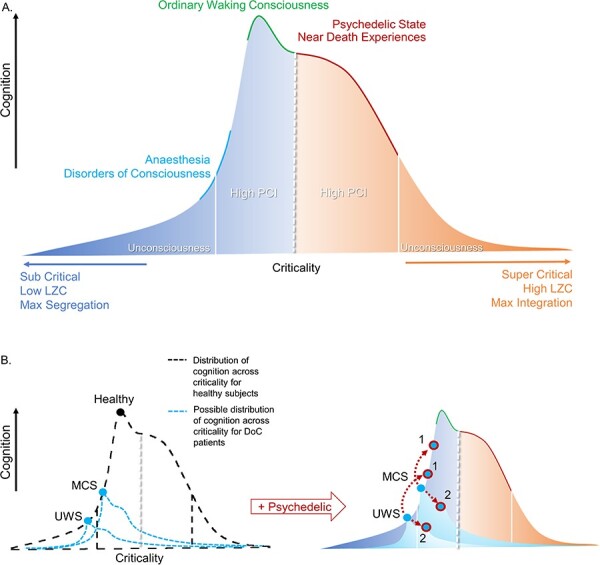
DoC = disorders of consciousness; PCI = perturbational complexity index; LZC = Lempel-Ziv complexity. Colours: orange = super-critical area; dark blue = sub-critical area.
(a) Global states without perturbation. Speculative schematic showing a landscape of states of consciousness and their cognitive capacities in accordance with the criticality of underlying networks in the brain. At each pole, both sub-critical and super-critical, a threshold represented by white lines represents unconsciousness and low PCI. Normal waking consciousness occupies a slightly sub-critical zone, where cognition is optimised at the local maximum. Psychedelic states and some other non-ordinary states of consciousness occupy a super-critical zone where cognition is forfeited for maximal sensitivity to internal and/or external stimuli. DoC and anaesthesia occupy a sub-critical zone that spans over unconscious states and states in which we are unsure as to the level of residual consciousness. (b) Pharmacological perturbation of DoC patients. Left, distribution of criticality for healthy subjects in black. In blue are possible distributions of cognition across levels of criticality for example UWS and MCS patients. The injured structural connectivity of DoC patients could result in deviations of the distribution of possible cognition across levels of criticality from that of healthy subjects. The circles represent the current level of cognition at a given moment. Right, upper. A speculative schematic prediction of an example UWS and MCS patient (baseline, light blue point) that receives a psychedelic to augment the complexity (blue points, circled in red). We display two possible scenarios. In Scenario 1, the patient follows the same distribution of healthy subjects, and their consciousness and related cognition increases (higher cognition, higher red outlined blue dot). Scenario 2 illustrates the idea that due to the damaged structural connectivity of the patients, the distribution of possible states changes so that the augmentation in complexity would be detrimental to residual cognitive capacities, as they already would occupy the point of optimal complexity for their given structure. Here, the point shifts from the local maximum of possible cognition (lower cognition, lower red outlined blue dot)