
Figure 6. Proteomic dissection of bio‐banked coronary aspirates from patients with STEMI segregated on the basis of long‐term clinical outcomes (vulnerable versus resilient).
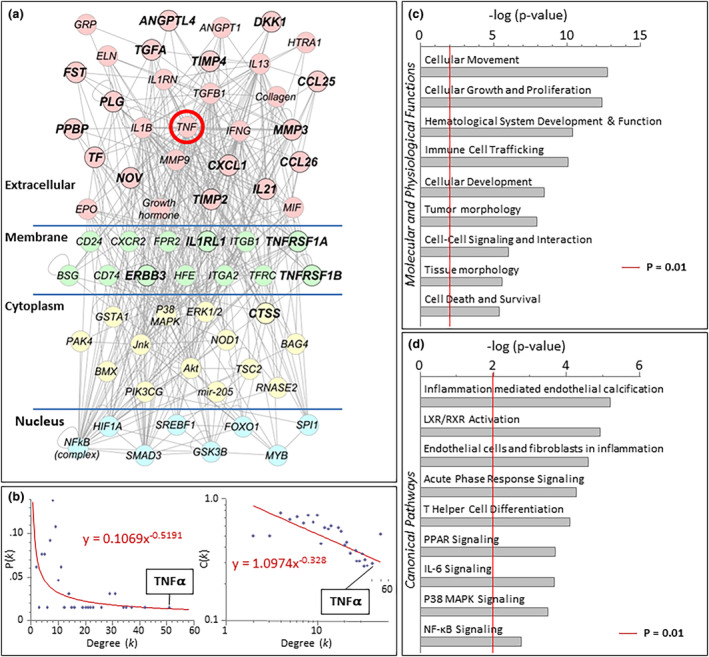
Analysis was performed with Ingenuity Pathways Knowledge Base (Ingenuity Systems, Redwood City, California). A, A TNF⍺‐centric network mediating worse outcomes was revealed. B, Following ingenuity pathway analysis, network topology ranked TNF⍺ as the most highly connected factor. Degree (k) is the number of connections that a node possesses, which can be plotted against either the proportion of total nodes with a specific degree [P(k)] to derive the degree distribution of the network or plotted against the clustering coefficient for nodes with degree k [C(k)] to derive the clustering coefficient for the network. The first graph [k vs P(k)] indicates whether a network possesses scale‐free topology, while the second graph [k vs C(k)] indicates whether the network possesses a hierarchical architecture. Cytoscape's Network Analyzer tool was used to derive the degree of distribution and clustering coefficient. C, Evaluation of overrepresented molecular and physiologic functions revealed cellular movement, cellular growth and proliferation, and hematological system development and function as the most highly overrepresented pathways (D) and inflammation of endothelium as the most highly ranked canonical pathway. Significance of P<0.01 is demonstrated by the red line in panels C and D. IL‐6 indicates interleukin‐6; LXR, liver X receptor; MAPK, mitogen‐activated protein kinase; NF‐κB, nuclear factor kappa‐light‐chain enhancer of activated B cells; PPAR, peroxisome proliferator‐activated receptor; RXR, retinoid X receptor; STEMI, ST‐segment–elevation myocardial infarction; and TNFα, tumor necrosis factor‐α.