
Fig. 1 |. Clinical overview.
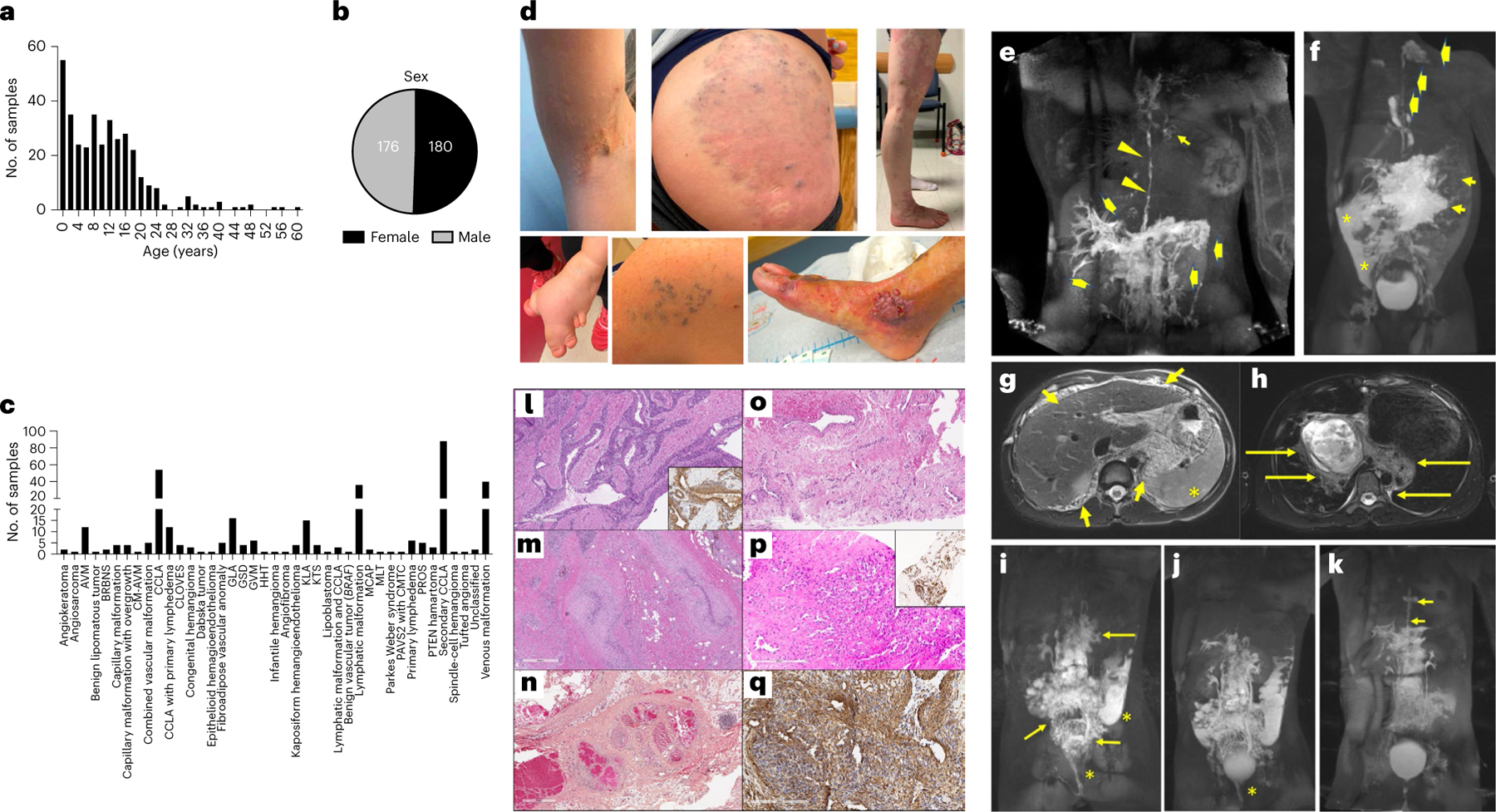
a,b, Age and sex of participants. c, Number of samples per ISSVA diagnosis. d, Example images of different participants that show microcystic lymphatic malformation, venous malformation and KTS (top panel, left to right); and syn-macrodactyly in a participant with CLOVES, GVM, and AVM (bottom panel, left to right). e, MR image of a participant with MAP2K1-CCLA (CLA135). Maximum intensity projection (MIP) after inguinal lymph node injection showing dilated and irregular thoracic duct (arrowheads), mediastinal lymphatic perfusion (short arrow) and retrograde flow in the liver and intestinal lymphatics (thick arrows). f, MR image of a participant with BRAF-GLA (CVA119). MIP from inguinal lymph node injection showing opacification of abdominal lymphatic malformation (short arrows), perfusion of cervical lymphatic malformation by a left-sided thoracic duct (thick arrows) and peritoneal lymphatic leak (asterisks). g,h, MR images of a 12-year-old male participant with PIK3CA-KLA and massive portal vein thrombosis (CVA52). Diffuse microcystic lymphatic malformation in the abdomen (short arrows) and cysts in the spleen (asterisk) (g) and lymphatic malformation involving the posterior mediastinum and hila (long arrows) (h). i,j, MR images of a participant with PIK3CA-CCLA (CVA65). MIP after injection of mesenteric (i) and liver (j) lymphatic vessels showing perfusion of the confluent abdominopelvic lymphatic malformation (long arrows) and leak of contrast into the sigmoid colon and vagina (asterisk). k, For CVA65 (same participant as in i,j), DCMRL images obtained 3 months after initiation of alpelisib and pelvic lymphovenous anastomosis showing reduced perfusion of pelvic lymphatics, resolved leak and dilated and tortuous thoracic duct (short arrows). l, Clinical histology showing dilated, tortuous venous channels with thickened smooth muscle coats containing multiple layers of perivascular cells similar to GVM due to a mosaic PDGFRB variant. Smooth muscle actin (inset) stains the smooth muscle and perivascular component (CVA172). m, Clinical histology showing tortuous and thickened or fibrotic compressed venous channels within a fibrous stroma containing fat, lymphocytes and hemosiderin due to a mosaic TEK variant (CVA19). n, Clinical histology showing a mixed vascular lesion containing dilated venous channels with ‘mulberry’ arrangement, thickened arterioles as well as nerve and abundant mature adipose tissue, consistent with PTEN hamartoma of soft tissue (CVA223). o, Clinical histology showing combined venous-capillary malformation due to a mosaic RASA1 (CVA05). p,q, Clinical histology of an unclassified vascular lesion with slit-like CD31+ (p, inset) endothelial cells and foci of surrounding cells positive for smooth muscle actin due to a mosaic GNAQ (CVA02) (q). For l–q, clinical histology was performed once with adequate positive and negative controls.