

Abstract
Background
In upright standing, spinopelvic mismatch is compensated by hip extension. However, few studies have investigated the reciprocal relationship between the sagittal alignment of the hip joints and spinopelvic mismatch during upright standing in humans. Our study aims to investigate (I) the relationship between spinopelvic mismatch and hip extension and (II) whether insufficient hip extension against spinopelvic mismatch, i.e., pelvic incidence (PI)-lumbar lordosis (LL), affects trunk inclination in upright standing.
Methods
This study was a retrospective cross-sectional study. We included 398 consecutive female patients treated for osteoporosis at our outpatient department between November 2017 and June 2022. Patients with any of the following were excluded from the study: (I) those whose plain whole-spine radiographs did not cover the femurs, (II) those with fractures in the vertebrae or lower extremities, (III) those with a history of surgery of the spine or of the lower extremities, (IV) those with scoliosis with a Cobb angle ≥10° in the anteroposterior radiograph, and (V) those with transitional vertebrae. Sixty-two patients were divided into normal and malalignment groups based on their sagittal spinal alignment. The patients underwent plain whole-spine radiography as a routine examination. A linear approximation between the pelvic femoral angle (PFA), representing hip extension, and PI-LL was obtained in both groups. The optimal PFA of each patient was obtained by substituting the PI-LL into the linear approximation of the normal group. The difference between the optimal and measured PFA was defined as the ΔPFA for each patient. The correlation between the ΔPFA and sagittal vertical axis (SVA) was evaluated in both groups.
Results
The PFA and PI-LL were correlated in both groups. The malalignment group had a significantly greater ΔPFA than the normal group. ΔPFA was correlated with SVA only in the malalignment group.
Conclusions
The magnitude of the ΔPFA indicated insufficient hip extension to compensate for the spinopelvic mismatch during upright standing.
Keywords: Pelvic incidence (PI), lumbar lordosis (LL), spinopelvic mismatch, pelvic femoral angle (PFA), hip joint
Highlight box.
Key findings
• The sagittal alignment of hip joints, expressed by pelvic femoral angle (PFA), was correlated with spinopelvic mismatch.
• The optimal PFA was calculated based on the spinopelvic mismatch of each patient, and the difference between optimal and actual PFA was defined as ΔPFA. The magnitude of the ΔPFA indicates the insufficiency of hip extension to compensate for spinopelvic mismatch.
• The ΔPFA correlated with sagittal vertical axis in patients with spinal sagittal malalignment.
What is known and what is new?
• Spinopelvic mismatch is known to be an important driver for the recruitment of compensatory mechanisms in the lower extremities.
• This is the first report to present the concept of an optimal relationship between the spinopelvic mismatch and sagittal alignment of hip joints.
What is the implication, and what should change now?
• The relationship between the sagittal alignment of the hip joints and spinopelvic mismatch is closely related to upright standing in humans.
Introduction
Humans stand upright with their lower limbs (ankles, knees, and hips), pelvis, and spine (lumbar, thoracic, and cervical) working in harmony with each other (1). Among these segments of the human body, the relationship between the pelvis and spine has been exhaustively investigated, especially using spinopelvic parameters such as pelvic incidence (PI) and lumbar lordosis (LL) (2,3). There is no difference in PI based on gender, or if there is, it is minor (4). It has been reported that LL is greater in female than in male (5,6). An extent of discrepancy between PI and LL, known as a spinopelvic mismatch, is related to sagittal spinal malalignment and health-related quality of life scores (2). As compensation for the reduction in LL, the pelvis was retroverted. However, the pelvic tilt (PT) to PI ratio shows no difference between males and females, indicating that this compensatory mechanism is the same across genders (4). The lumbar spine and hip joints are linked; therefore, the pathology of the one affecting the other is known as hip-spine syndrome (7). However, few studies have investigated and discussed the reciprocal relationship between the sagittal alignment of the hip joints and spinopelvic mismatch during upright standing in humans (8).
The sagittal alignment of the hip joints can be expressed by the relationship between the pelvis and femur. The most commonly used radiographic parameter is the angle made by the pelvic axis, which is a line drawn from the midpoint of the bilateral femoral head centers to the midpoint of the sacral endplate and femoral shaft axis. This pelvic axis is identical to that used to measure the PI and the PT (Figure 1). This parameter expressing the sagittal alignment of the hip joints increases with hip extension and decreases with hip flexion (8). In previous studies, several names have been used to express this parameter, such as pelvic femoral angle (PFA), sacrofemoral angle, and pelvi-femoral angle (8-11). We adopted the term PFA in this study.
Figure 1.

Definition of the PFA and PT. The PFA is defined as the angle between a line drawn from the midpoint of the bilateral femoral head center to the midpoint of the sacral endplate and the proximal femoral shaft axis. The proximal femoral axis is drawn as a line connecting the midpoints of the anterior-most and posterior-most cortices of the proximal and distal portions of the femur (line A). Line B is parallel to line A and passes through the center of the femoral head. The PT is defined as the angle between the plumb line and a line drawn from the midpoint of the bilateral femoral head centers to the midpoint of the sacral endplate. PFA, pelvic femoral angle; PT, pelvic tilt.
Even among elderly patients with kyphosis, the degree of anterior trunk inclination varies. While some exhibit minimal anterior trunk inclination during walking, some demonstrate a significant anterior trunk inclination (12). Upright standing requires compensatory mechanisms of the lower extremities against spinopelvic mismatch. In other words, the spinopelvic mismatch is an important driver for the recruitment of compensatory mechanisms in the lower extremities (3). We then hypothesized that (I) spinopelvic alignment is correlated with the sagittal alignment of the hip joints, (II) there is an optimal PFA for each individual standing upright, and it is calculated based on the PFA and PI-LL, (III) the discrepancy between the optimal PFA and actual PFA correlates with the extent of anterior trunk tilt in patients with sagittal spinopelvic malalignment. We present this article in accordance with the STROBE reporting checklist (available at https://jss.amegroups.com/article/view/10.21037/jss-23-145/rc).
Methods
This study is a retrospective, cross-sectional study utilizing pre-existing radiological images. The study was conducted in accordance with the Declaration of Helsinki (as revised in 2013). The study was approved by Institutional Review Board of Tohoku University (No. 2022-1-912) and informed consent was taken from all the patients.
Study population
Subjects capable of maintaining an upright stand posture with healthier spine and lower extremity conditions were chosen for the radiographic assessment of their sagittal alignment, as described below. We included 398 consecutive female patients treated for osteoporosis and underwent plain whole-spine radiography as a routine examination at our outpatient department between November 2017 and June 2022. Patients with any of the following were excluded from the study: (I) those whose plain whole-spine radiographs did not cover the femurs, (II) those with fractures in the vertebrae or lower extremities, (III) those with a history of surgery of the spine or of the lower extremities, (IV) those with scoliosis with a Cobb angle ≥10° in the anteroposterior radiograph, and (V) those with transitional vertebrae. Specifically, criteria (II), (III), and (IV) were established to minimize biases impacting the spinal alignment, thereby ensuring the selection of subjects with near-normal profiles. As a result, a total of 62 patients were included in the study, with a mean age of 60 years (Figure 2).
Figure 2.

Flowchart of the participant selection. We screened 398 female patients who were treated for osteoporosis at our department. We excluded the following patients: 48 whose plain whole-spine radiographs did not cover the femurs, 185 with fractures or fractures of the spine or lower extremities, 100 with degenerative disease of the spine or lower extremities, one with a Cobb angle ≥10° on the anteroposterior radiograph, and two with transitional vertebra. Ultimately, 62 patients were included in this study.
Radiographic evaluation
When obtaining the lateral view of the plain whole-spine radiograph, the patients were instructed to stand naturally, with their arms raised horizontally forward at approximately 30° of flexion at the shoulder (13). Spinopelvic parameters, including the sagittal vertical axis (SVA), thoracic kyphosis (TK) at T1–12, LL at L1–S1, PI, and PT, were measured (Figure 3). PFA was defined as the angle between the line drawn from the midpoint of the bilateral femoral head center to the midpoint of the sacral endplate and the proximal femoral shaft axis. The proximal femoral shaft axis was drawn as a line connecting the midpoints of the most anterior and posterior cortices of the proximal and distal portions of the femurs (Figure 1). These parameters were compared between the normal and malalignment groups. A spine surgeon with 19 years of experience and a hip joint surgeon with 15 years of experience measured these parameters twice. To prevent recall bias, each measurement was randomly performed in more than one-month intervals. As for the interclass correlation coefficients (ICCs) of each measured parameter, [ICC (1, 1)] and [ICC (2, 1)] were calculated for intraobserver agreement and interobserver agreement, respectively, using SPSS statistics (version 21.0; IBM, Chicago, IL, USA). For interobserver agreement, the ICC (2, 1) was calculated in a round-robin manner (2 measurements × 2 examiners = 4 combinations). The values less than 0.5, between 0.5 and 0.75, between 0.75 and 0.9, and greater than 0.90 are indicative of poor, moderate, good, and excellent reliability, respectively (14).
Figure 3.
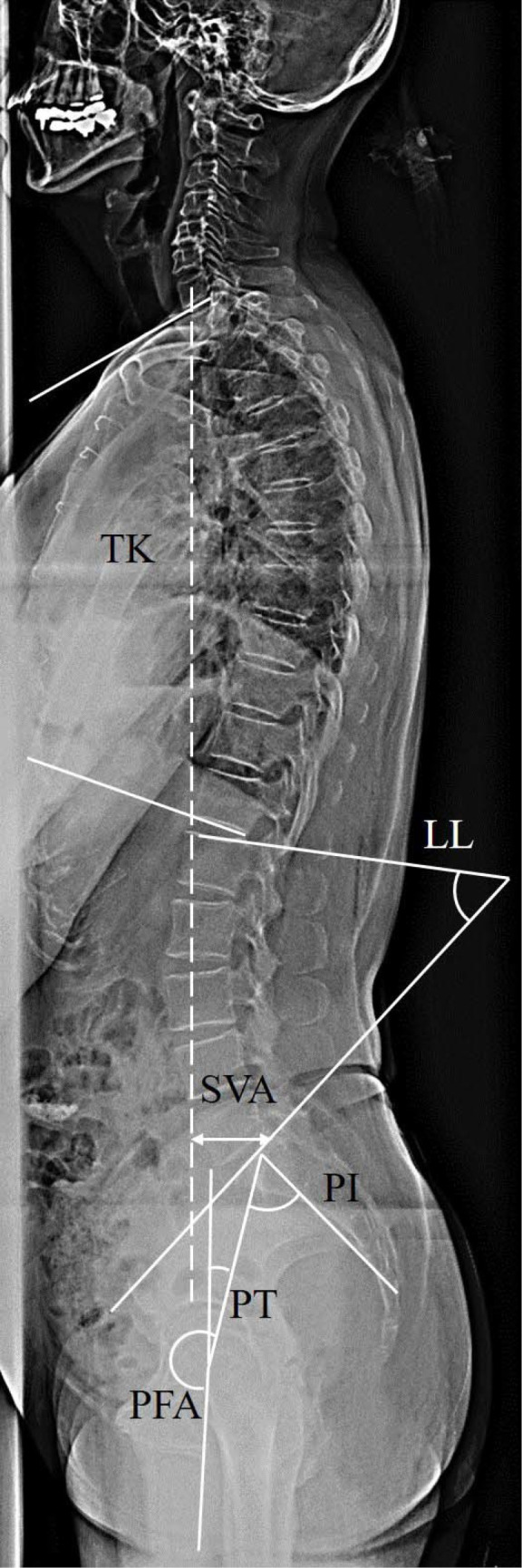
Measurement of spinopelvic parameters in the whole-spine lateral radiograph. The following parameters were measured: SVA (the distance between the plumb line passing through the center of the C7 vertebra and posterior superior corner of the sacral endplate), TK (the angle between the upper endplate of T1 and lower endplate of T12), LL (the angle between the upper endplate of L1 and the endplate of the sacrum), and PI (the angle between a line perpendicular to the endplate of the sacrum and a line drawn from the midpoint of the bilateral femoral head centers to the midpoint of the sacral endplate), PT (the angle between the plumb line and a line drawn from the midpoint of the bilateral femoral head centers to the midpoint of the sacral endplate), PFA (the angle between a line drawn from the midpoint of the bilateral femoral head centers to the midpoint of the sacral endplate, and the proximal femoral shaft axis). TK, thoracic kyphosis; LL, lumbar lordosis; SVA, sagittal vertical axis; PI, pelvic incidence; PT, pelvic tilt; PFA, pelvic femoral angle.
Patients were divided into two groups per the Scoliosis Research Society-Schwab classification of adult spinal deformity. The normal group comprised individuals whose two sagittal spinopelvic modifiers were within the normal range (PI-LL <10° and SVA <40 mm), and the malalignment group comprised individuals whose any of the two parameters was out of the normal range (PI-LL ≥10° or SVA ≥40 mm) (15). The demographic data of the spinopelvic parameters were compared, and the correlation of spinopelvic parameters was investigated between the groups. A linear correlation between the PFA and PI-LL was calculated for the normal group.
Statistical analysis
The results were presented as average ± standard deviation. The average of four measurements (performed twice by two examiners) was used for the analysis. The distribution of demographic data, including PI-LL, was assessed for normality using the Shapiro-Wilk test at the significance level of P<0.05. For the comparison of the two groups, the Student’s t-test and the Mann-Whitney U test were used for parameters with normal and non-normal distributions, respectively. For the assessment of correlation between two variables, the Pearson coefficient and the Spearman’s rank correlation were used for parameters with normal and non-normal distributions, respectively. After confirming that the distribution of PFA approximated a normal distribution using a histogram, a linear correlation equation for PFA using PI-LL was obtained from the data of the normal group. The optimal PFA was defined as the value obtained by substituting each patient’s PI-LL into the linear correlation equation. Subsequently, the difference between the optimal PFA and actual PFA measured in the same patient was calculated and defined as ΔPFA, as shown in the equation below.
| [1] |
The ΔPFA was compared between groups using the Student’s t-test. The correlation between ΔPFA and SVA in each group was assessed using Spearman’s rank correlation coefficient. A post hoc power analysis was conducted for the correlation coefficient. Statistical significance was set at P<0.05, and analyses were performed using JMP Software Version 16.2.0 (SAS Institute Japan, Tokyo, Japan).
Results
Intraobserver and Interobserver agreement
The ICCs [ICC (1, 1)] for the intraobserver agreement and [ICC (2, 1)] for the interobserver agreement ranged from 0.86 to 0.99 and 0.83 to 0.99, respectively. The average of the ICCs ranged from 0.86 to 0.99; therefore, the observer agreement levels were “good” or “excellent” (Table 1) (14).
Table 1. The interclass correlations coefficients of interobserver and intraobserver agreement.
| Variables | Interobserver agreement | Intraovserver agreement | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Ex. 1—1st vs.
Ex. 2—1st |
Ex. 1—2nd vs. Ex. 2—2nd | Ex. 1—1st vs.
Ex. 2—2nd |
Ex. 1—2nd vs. Ex. 2—1st | Average | Ex. 1—1st vs.
Ex. 1—2nd |
Ex. 2—1st vs.
Ex. 2—2nd |
Average | ||
| SVA | 0.98 | 0.98 | 0.99 | 0.99 | 0.99 | 0.98 | 0.99 | 0.99 | |
| PFA | 0.92 | 0.9 | 0.89 | 0.92 | 0.91 | 0.94 | 0.9 | 0.92 | |
| PI | 0.9 | 0.83 | 0.83 | 0.87 | 0.86 | 0.88 | 0.86 | 0.87 | |
| PT | 0.97 | 0.93 | 0.88 | 0.95 | 0.93 | 0.95 | 0.9 | 0.93 | |
| LL | 0.84 | 0.89 | 0.86 | 0.9 | 0.87 | 0.87 | 0.95 | 0.91 | |
| TK | 0.84 | 0.86 | 0.9 | 0.86 | 0.87 | 0.86 | 0.92 | 0.89 | |
Ex., examiner; 1st, 1st inspection; 2nd, 2nd inspection; SVA, sagittal vertical axis; PFA, pelvic femoral angle; PI, pelvic incidence; PT, pelvic tilt; LL, lumbar lordosis; TK, thoracic kyphosis.
Spinopelvic parameters and PFA in normal and malalignment groups
The normal and malalignment groups comprised 43 patients with a mean age of 59 years (range, 33–80 years) and 19 patients with a mean age of 66 years (range, 45–79 years), respectively. For the malalignment group, SVA and PI-LL were found to be non-normally distributed (P=0.01 and 0.049, respectively), while the rest of the parameters were normally distributed. As for the comparison between normal and malalignment groups, age, SVA, PFA, PI and PT were significantly larger, and LL, PI-LL and TK were significantly lower in malalignment group, respectively, as shown in Table 2.
Table 2. Demographic data.
| Variables | All | Normal group | Malalignment group | P value |
|---|---|---|---|---|
| Numbers of patients | 62 | 43 | 19 | – |
| Age (years) | 60.9±11.4 | 58.5±11.1 | 66.4±10.3 | 0.01* |
| SVA (mm) | 15.2±36.6 | −0.3±19.3 | 42.2 (25.7, 66.9) | <0.001* |
| PFA (°) | 193.8±7.1 | 192.4±6.8 | 196.9±6.8 | 0.01* |
| PI (°) | 53.1±9.2 | 51.8±7.7 | 56.1±11.5 | 0.09 |
| PT (°) | 18.4±7.7 | 15.8±5.8 | 24.3±8.1 | <0.001* |
| LL (°) | 49.1 (41.1, 56.2) | 52.0±8.5 | 38.8±12.9 | <0.001* |
| PI-LL (°) | 4.3 (−2.8, 10.4) | −0.2±6.5 | 17.5 (10.8, 23.6) | <0.001* |
| TK (°) | 34.1±13.6 | 38.6±11.0 | 24.0±13.7 | <0.001* |
The values are indicated in n, mean ± standard deviation and interquartile range: median (25–75 percentile) for normally and non-normally distributed parameters, respectively. The comparison between two groups were performed using the Mann-Whitney U test for SVA and PI-LL, and Student’s t-test for the rest of the parameters, respectively. *, statistical significance: P<0.05. SVA, sagittal vertical axis; PFA, pelvic femoral angle; PI, pelvic incidence; PT, pelvic tilt; LL, lumbar lordosis; TK, thoracic kyphosis.
Correlation between PFA and spinopelvic parameters
The Pearson and Spearman’s rank correlation coefficients for each parameter are listed in Table 3. PI-LL correlated with PFA (r=0.53, P<0.001), PT (r=0.58, P<0.001), LL (r=−0.49, P<0.001), and TK (r=−0.48, P=0.001) in the normal group, and PFA (r=0.47, P=0.046) and PT (r=0.77, P<0.001) in the malalignment group (Table 3). The scatter diagrams of the PFA and PI-LL in both groups are shown in Figure 4. PFA in the normal group was confirmed to have a normal distribution. From this linear correlation equation, PFA was deduced by individual PI-LL, which was named optimal PFA.
Table 3. Correlation between each parameter in each group.
| Variables | Normal group | Malalignment group | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| SVA | PFA | PI | PT | LL | PI-LL | TK | SVA | PFA | PI | PT | LL | PI-LL | TK | ||
| SVA | |||||||||||||||
| Correlation coefficient | – | – | – | – | – | – | – | – | – | – | – | – | – | – | |
| P value | – | – | – | – | – | – | – | – | – | – | – | – | – | – | |
| PFA | |||||||||||||||
| Correlation coefficient | 0.04 | – | – | – | – | – | – | −0.32 | – | – | – | – | – | – | |
| P value | 0.79 | – | – | – | – | – | – | 0.18 | – | – | – | – | – | – | |
| PI | |||||||||||||||
| Correlation coefficient | −0.11 | 0.52 | – | – | – | – | – | 0.04 | 0.75 | – | – | – | – | – | |
| P value | 0.47 | <0.001* | – | – | – | – | – | 0.89 | 0.0002* | – | – | – | – | – | |
| PT | |||||||||||||||
| Correlation coefficient | 0.05 | 0.91 | 0.6 | – | – | – | – | 0.1 | 0.82 | 0.68 | – | – | – | – | |
| P value | 0.7 | <0.001* | <0.001* | – | – | – | – | 0.68 | <0.001* | 0.001* | – | – | – | – | |
| LL | |||||||||||||||
| Correlation coefficient | −0.06 | 0.06 | 0.68 | 0.1 | – | – | – | −0.2 | 0.26 | 0.56 | 0.06 | – | – | – | |
| P value | 0.66 | 0.67 | <0.001* | 0.51 | – | – | – | 0.42 | 0.27 | 0.01* | 0.79 | – | – | – | |
| PI-LL | |||||||||||||||
| Correlation coefficient | −0.04 | 0.53 | 0.29 | 0.58 | −0.49 | – | – | 0.29 | 0.47 | 0.37 | 0.77 | −0.42 | – | – | |
| P value | 0.77 | <0.001* | 0.051 | <0.001* | <0.001* | – | – | 0.22 | 0.046* | 0.11 | <0.001* | 0.07 | – | – | |
| TK | |||||||||||||||
| Correlation coefficient | 0.41 | 0.26 | 0.15 | 0.22 | 0.51 | −0.48 | – | −0.004 | −0.46 | −0.39 | −0.42 | 0.05 | −0.45 | – | |
| P value | 0.005* | 0.08 | 0.31 | 0.14 | <0.001* | 0.001* | – | 0.99 | 0.047* | 0.09 | 0.06 | 0.82 | 0.053 | <0.001* | |
The Pearson correlation coefficient was calculated for normal group. For malalignment group, the correlation coefficient for variables including SVA and PI-LL was calculated using the Spearman correlation coefficient, while the Pearson correlation coefficient was calculated for other variables. *, statistical significance: P<0.05. SVA, sagittal vertical axis; PFA, pelvic femoral angle; PI, pelvic incidence; PT, pelvic tilt; LL, lumbar lordosis; TK, thoracic kyphosis.
Figure 4.

Relationship between PFA and PI-LL. (A) Normal group. (B) Malalignment group. PFA correlated with PI-LL in both groups. The Spearman’s rank correlation coefficient was 0.51 in the normal group and 0.47 in the malalignment group. PFA: the angle between a line drawn from the midpoint of the bilateral femoral head centers to the midpoint of the sacral endplate, and the proximal femoral shaft axis. PI: the angle between a line perpendicular to the endplate of the sacrum and a line drawn from the midpoint of the bilateral femoral head centers to the midpoint of the sacral endplate. LL: the angle between the upper endplate of L1 and the endplate of the sacrum. PI-LL: the angle defined as PI-LL. PFA, pelvic femoral angle; PI, pelvic incidence; LL, lumbar lordosis.
| [2] |
ΔPFA was obtained for each patient using the following formula:
| [3] |
The ΔPFA in the malalignment group was significantly larger than that in the normal group (P=0.001), at −0.5°±5.8° (range, −14.9° to 10.4°) and 5.5°±7.1° (range, −5.5° to 25.4°) in the normal and malalignment groups, respectively. A significant correlation was found between ΔPFA and SVA in the malalignment group, with Spearman’s rank correlation coefficient of 0.53 (P=0.02), whereas no correlation was found in the normal group (Figure 5). The power of this study was revealed to be 0.68 by the power analysis.
Figure 5.

Relationship between the ΔPFA and SVA in the normal group (A) and the malalignment group (B). No correlation was observed in the normal group (A). The ΔPFA was positively correlated with the SVA in the malalignment group, with a Spearman’s rank correlation coefficient of 0.66 (B). PFA: the angle between a line drawn from the midpoint of the bilateral femoral head centers to the midpoint of the sacral endplate, and the proximal femoral shaft axis. SVA: the distance between the plumb line passing through the center of the C7 vertebra and posterior superior corner of the sacral endplate. SVA, sagittal vertical axis; PFA, pelvic femoral angle.
Case presentations (Figure 6)
Figure 6.

Case presentations. (A) Case 1. A 61-year-old woman with a negative ΔPFA. She had a PI-LL mismatch, however, the hip joints were sufficiently extended. (B) Case 2. A 77-year-old woman with a positive ΔPFA. ΔPFA indicated that the hip joints were not sufficiently extended. The trunk was leaning slightly anterior. (C) Case 3. A 79-year-old woman with a positive ΔPFA. She had a PI-LL mismatch. The extension of the hip joints was insufficient. ΔPFA was larger than case 2. Certainly, SVA also becomes larger compared to case 2. PFA: the angle between a line drawn from the midpoint of the bilateral femoral head centers to the midpoint of the sacral endplate, and the proximal femoral shaft axis. SVA: the distance between the plumb line passing through the center of the C7 vertebra and posterior superior corner of the sacral endplate. PI, pelvic incidence; LL, lumbar lordosis; PFA, pelvic femoral angle; SVA, sagittal vertical axis; PT, pelvic tilt.
❖ Case 1. A 61-year-old woman with a negative ΔPFA. She had a PI-LL mismatch, however, the hip joints could be extended sufficiently. SVA was negative, and the trunk was not inclined anteriorly. The parameters were as follows: SVA, −2.7 mm; PI-LL, 18°; PFA, 206.6°; optimal PFA, 202.8°; and ΔPFA, −3.8°.
❖ Case 2. A 77-year-old woman with a positive ΔPFA. ΔPFA indicated that the hip joints could not be extended sufficiently. SVA was exceeded 40 mm. The trunk was leaning slightly anterior. The parameters were as follows: SVA, 52.2 mm; PI-LL, −2.3°; PFA, 184.3°; optimal PFA, 190.7°; and ΔPFA 6.3°.
❖ Case 3. A 79-year-old woman with a positive ΔPFA. She had a PI-LL mismatch. The extension of the hip joints was insufficient. ΔPFA was larger than case 2. Certainly, SVA also becomes larger compared to case 2, as the ΔPFA and SVA are correlated. The parameters were as follows: SVA, 182 mm; PI-LL, 51.7°; PFA, 197.6°; optimal PFA, 223°; and ΔPFA, 25.4°.
Discussion
PT is not a suitable parameter for assessing the sagittal alignment of the hip joints because it is affected not only by the hip joints but also by the knee joints (16). Thus, we utilized PFA, defined solely by the positional relationship between the pelvis and the femur. Previous reports have revealed that PFA is affected by age, sex, hip joint pathology (e.g., smaller in patients with hip osteoarthritis), pelvic morphology (e.g., larger in individuals with higher PI), and PI-LL (8,10,11,17). According to the measurement by low-dose radiation, head-to-foot and biplanar standing stereoradiographic images (EOS imaging, Alphatec, Paris, France), the mean PFA of healthy individuals (average age: 40 years) was 197°, whereas that of patients with spinal deformities ranged from 194° to 207° (8,10,17,18). Several factors affect sagittal alignment of the hip joints, and the standard PFA value is poorly understood.
In a study of adult patients with degenerative spinal disease, PFA was correlated with PI-LL, with a correlation coefficient of 0.541 (8). In our study of patients without remarkable spinal diseases, PFA was also correlated with PI-LL, suggesting that the hip joints play a role in compensating for spinopelvic mismatch during upright standing. The magnitude of the ΔPFA indicates the insufficiency of hip extension to compensate for spinopelvic mismatch in upright standing. ΔPFA becomes positive when the hip extension is insufficient relative to the optimal hip position based on the individual’s PI-LL, whereas it becomes negative when the hip extension is sufficient to compensate for PI-LL. The ΔPFA was larger in the malalignment group, indicating that the extension of the hip joints in individuals with sagittal malalignment was insufficient relative to the value calculated from PI-LL.
Spinopelvic mismatch is compensated by the thoracic spine, pelvis, and lower extremities (19). In the normal group, PI-LL correlated with PFA and TK, but ΔPFA did not correlate with SVA. These results suggest that upright standing is maintained by the hip joints and the thoracic spine to keep the trunk upright. These two compensation mechanisms work together to maintain the trunk upright. Therefore, no correlation between the degree of the compensation mechanism of the hip joints and anterior trunk inclination may have been found in the normal group. In the malalignment group, PI-LL did not correlate with TK. These results may indicate that the thoracic spine reached a compensatory limit owing to its small capacity in the degenerative spine (19). In addition, PI-LL correlated with PFA, as did the ΔPFA with SVA, suggesting that the compensatory function of the hip joints plays an important role in individuals with sagittal malalignment. The ΔPFA can be implicated as a regulator of SVA. That is, an inharmonious relationship between PI-LL and sagittal alignment of the hip joints causes an anterior inclination of the trunk in individuals with spinal sagittal malalignment.
To the best of our knowledge, this is the first report to present the concept of an optimal relationship between the PI-LL and sagittal hip alignment. It is clinically crucial that an optimal PFA could be calculated from PI-LL, and the difference between the optimal PFA and the measured PFA, in other words ΔPFA, could be expressed as an objective numerical value. The compensatory mechanism of the hip joints in response to spinopelvic mismatch could be objectively evaluated by using ΔPFA. We believe the ΔPFA may indicate a compensatory insufficiency of the hip joints in patients with spinal sagittal malalignment. In cases with positive ΔPFA, PI-LL may be poorly compensated by the hip joints because of coexisting pathology in the hip joints, weakness in the hip extensor muscles, flexion contracture of the hip joints, or by a PI-LL that is too large to be compensated only by the hip joints.
It has been reported that there exists an optimal LL for PI (2). This study presents a novel finding that spinopelvic mismatch significantly influences hip positioning in the erect posture. However, the dynamics of the hip joint undergo substantial changes during ambulation or in the transition from sitting to standing. Notably, the variation in sagittal pelvic tilt between the standing and sitting positions has been the subject of extensive research. It has been observed that individual variations in pelvic tilt adjustments, due to changes in posture, are closely associated with the range of motion in the lumbar spine (20,21). Furthermore, studies have shown that among Japanese women aged over 50 years, there is a notable reduction in both LL and lumbar mobility as a function of aging (22). In our investigation, the group with spinal malalignment was significantly older, suggesting a potential disparity in lumbar mobility between the examined groups. It is imperative for future research to delve into the examination of alterations in lumbar mobility and the positional dynamics of the hip joint during physical activities, such as walking or the transition from a seated to a standing posture.
This study has several limitations. First, the sample size particularly in the malalignment group was small which made the power insufficient. Further studies with a larger number of patients with spinal sagittal malalignment of greater severity are needed to establish the clinical applicability of this parameter, and to investigate whether this concept can be applied to patients with symptomatic spinal kyphosis. Furthermore, the exclusive inclusion of female subjects may introduce a gender-specific bias in the results pertaining to spinal alignment. Regarding sexual dimorphism, PI has been reported to exhibit negligible or minor differences between genders (4). Conversely, LL is documented to be more pronounced in females as compared to males (5,6). This study was a retrospective study that did not enroll healthy volunteers. The patients included in this study were undergoing treatment for osteoporosis, the majority of them were female. Due to the small number of male patients and the inability to statistically evaluate differences due to gender, only females were included in the study. Further research was needed on the hip compensation mechanism in cases with such diseases. Another limitation was that the health-related quality of life was not measured. Furthermore, the influences of the knee and ankle joints on the anterior inclination of the trunk were not evaluated.
Conclusions
The ΔPFA, which is the difference between the optimal and actual PFA, may indicate a compensatory insufficiency of the hip joints for spinal sagittal malalignment. In individuals with normal spinal sagittal alignment, a small PI-LL can be adjusted by the thoracic spine and hip joints to maintain a certain range of trunk inclinations. The relationship between the sagittal alignment of the hip joints and spinopelvic mismatch is closely related to upright standing in humans.
Supplementary
The article’s supplementary files as
Acknowledgments
We would like to thank Editage for editing and reviewing the language of this manuscript.
Funding: None.
Ethical Statement: The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. The study was conducted in accordance with the Declaration of Helsinki (as revised in 2013). The study was approved by Institutional Review Board of Tohoku University (No. 2022-1-912) and informed consent was taken from all the patients.
Footnotes
Reporting Checklist: The authors have completed the STROBE reporting checklist. Available at https://jss.amegroups.com/article/view/10.21037/jss-23-145/rc
Data Sharing Statement: Available at https://jss.amegroups.com/article/view/10.21037/jss-23-145/dss
Peer Review File: Available at https://jss.amegroups.com/article/view/10.21037/jss-23-145/prf
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://jss.amegroups.com/article/view/10.21037/jss-23-145/coif). The authors have no conflicts of interest to declare.
References
- 1.Hasegawa K, Dubousset JF. Cone of Economy with the Chain of Balance-Historical Perspective and Proof of Concept. Spine Surg Relat Res 2022;6:337-49. 10.22603/ssrr.2022-0038 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Schwab FJ, Blondel B, Bess S, et al. Radiographical spinopelvic parameters and disability in the setting of adult spinal deformity: a prospective multicenter analysis. Spine (Phila Pa 1976) 2013;38:E803-12. 10.1097/BRS.0b013e318292b7b9 [DOI] [PubMed] [Google Scholar]
- 3.Diebo BG, Ferrero E, Lafage R, et al. Recruitment of compensatory mechanisms in sagittal spinal malalignment is age and regional deformity dependent: a full-standing axis analysis of key radiographical parameters. Spine (Phila Pa 1976) 2015;40:642-9. 10.1097/BRS.0000000000000844 [DOI] [PubMed] [Google Scholar]
- 4.Mac-Thiong JM, Roussouly P, Berthonnaud E, et al. Age- and sex-related variations in sagittal sacropelvic morphology and balance in asymptomatic adults. Eur Spine J 2011;20 Suppl 5:572-7. 10.1007/s00586-011-1923-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Yukawa Y, Matsumoto T, Kollor H, et al. Local Sagittal Alignment of the Lumbar Spine and Range of Motion in 627 Asymptomatic Subjects: Age-Related Changes and Sex-Based Differences. Asian Spine J 2019;13:663-71. 10.31616/asj.2018.0187 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Lang-Tapia M, España-Romero V, Anelo J, et al. Differences on spinal curvature in standing position by gender, age and weight status using a noninvasive method. J Appl Biomech 2011;27:143-50. 10.1123/jab.27.2.143 [DOI] [PubMed] [Google Scholar]
- 7.Offierski CM, MacNab I. Hip-spine syndrome. Spine (Phila Pa 1976) 1983;8:316-21. 10.1097/00007632-198304000-00014 [DOI] [PubMed] [Google Scholar]
- 8.Ferrero E, Liabaud B, Challier V, et al. Role of pelvic translation and lower-extremity compensation to maintain gravity line position in spinal deformity. J Neurosurg Spine 2016;24:436-46. 10.3171/2015.5.SPINE14989 [DOI] [PubMed] [Google Scholar]
- 9.Innmann MM, Merle C, Phan P, et al. Differences in Spinopelvic Characteristics Between Hip Osteoarthritis Patients and Controls. J Arthroplasty 2021;36:2808-16. 10.1016/j.arth.2021.03.031 [DOI] [PubMed] [Google Scholar]
- 10.Hasegawa K, Okamoto M, Hatsushikano S, et al. Normative values of spino-pelvic sagittal alignment, balance, age, and health-related quality of life in a cohort of healthy adult subjects. Eur Spine J 2016;25:3675-86. 10.1007/s00586-016-4702-2 [DOI] [PubMed] [Google Scholar]
- 11.Hasegawa K, Okamoto M, Hatsushikano S, et al. Standing sagittal alignment of the whole axial skeleton with reference to the gravity line in humans. J Anat 2017;230:619-30. 10.1111/joa.12586 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Kamata K, Ozawa H, Sekiguchi Y, et al. Spino-pelvic- lower extremity balance during walking in elderly patients with spinal kyphosis. J Orthop Sci 2019;24:793-7. 10.1016/j.jos.2019.01.005 [DOI] [PubMed] [Google Scholar]
- 13.Vedantam R, Lenke LG, Bridwell KH, et al. The effect of variation in arm position on sagittal spinal alignment. Spine (Phila Pa 1976) 2000;25:2204-9. 10.1097/00007632-200009010-00011 [DOI] [PubMed] [Google Scholar]
- 14.Koo TK, Li MY. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J Chiropr Med 2016;15:155-63. 10.1016/j.jcm.2016.02.012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Schwab F, Ungar B, Blondel B, et al. Scoliosis Research Society-Schwab adult spinal deformity classification: a validation study. Spine (Phila Pa 1976) 2012;37:1077-82. 10.1097/BRS.0b013e31823e15e2 [DOI] [PubMed] [Google Scholar]
- 16.Lafage R, Liabaud B, Diebo BG, et al. Defining the Role of the Lower Limbs in Compensating for Sagittal Malalignment. Spine (Phila Pa 1976) 2017;42:E1282-8. 10.1097/BRS.0000000000002157 [DOI] [PubMed] [Google Scholar]
- 17.Day LM, DelSole EM, Beaubrun BM, et al. Radiological severity of hip osteoarthritis in patients with adult spinal deformity: the effect on spinopelvic and lower extremity compensatory mechanisms. Eur Spine J 2018;27:2294-302. 10.1007/s00586-018-5509-0 [DOI] [PubMed] [Google Scholar]
- 18.Shimizu T, Lehman RA, Jr, Sielatycki JA, et al. Reciprocal change of sagittal profile in unfused spinal segments and lower extremities after complex adult spinal deformity surgery including spinopelvic fixation: a full-body X-ray analysis. Spine J 2020;20:380-90. 10.1016/j.spinee.2019.09.012 [DOI] [PubMed] [Google Scholar]
- 19.Barrey C, Roussouly P, Le Huec JC, et al. Compensatory mechanisms contributing to keep the sagittal balance of the spine. Eur Spine J 2013;22 Suppl 6:S834-41. 10.1007/s00586-013-3030-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Rivière C, Lazennec JY, Van Der Straeten C, et al. The influence of spine-hip relations on total hip replacement: A systematic review. Orthop Traumatol Surg Res 2017;103:559-68. 10.1016/j.otsr.2017.02.014 [DOI] [PubMed] [Google Scholar]
- 21.Kobayashi T, Morimoto T, Yoshihara T, et al. The significant relationship among the factors of pelvic incidence, standing lumbar lordosis, and lumbar flexibility in Japanese patients with hip osteoarthritis: A descriptive radiographic study. Orthop Traumatol Surg Res 2022;108:103123. 10.1016/j.otsr.2021.103123 [DOI] [PubMed] [Google Scholar]
- 22.Kasukawa Y, Miyakoshi N, Hongo M, et al. Age-related changes in muscle strength and spinal kyphosis angles in an elderly Japanese population. Clin Interv Aging 2017;12:413-20. 10.2147/CIA.S113352 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
The article’s supplementary files as