
FIGURE 2.
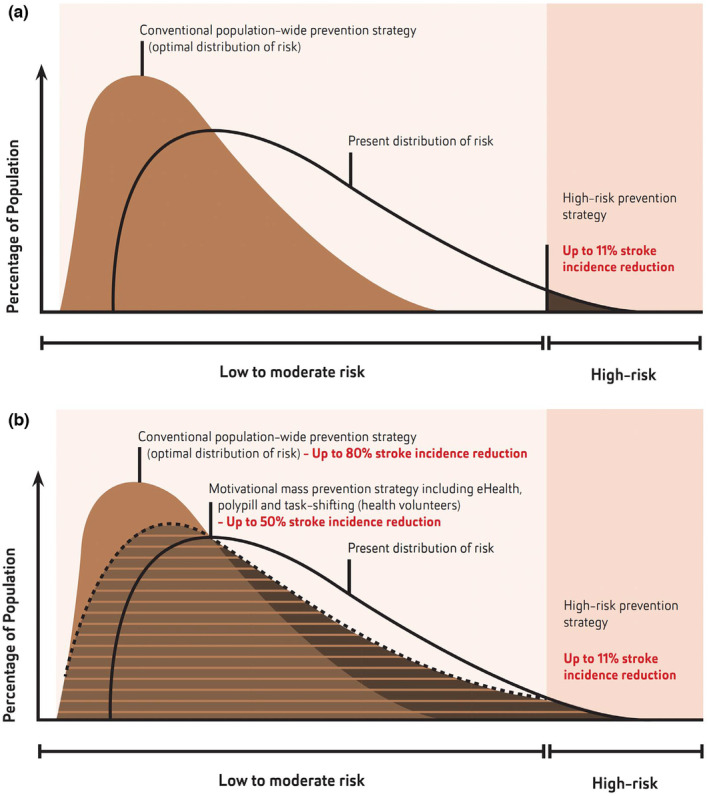
Optimal shift in the distribution of stroke and cardiovascular disease (CVD) risks that could be achieved with the adaptation of the recommended changes in stroke/CVD prevention strategies from high CVD risk prevention strategy to motivational mass prevention strategies in all individuals with elevated risk of stroke/CVD, regardless of the level of risk (e.g., eHealth, polypill and task‐shifting in stroke/CVD prevention/screening to health workers/volunteers) and wider implementation of population‐wide prevention strategies. (Modified from Feigin et al. [97] and Owolabi et al. [56], with permission.) Areas shaded in brown show a theoretically possible proportion of the population that could benefit from (a) high CVD risk prevention strategy (at best 11% stroke/CVD risk reduction) and (b) a motivational mass individual risk prevention strategy regardless of the CVD risk level (e.g., use of mobile applications to reduce lifestyle and other risks, polypill and task‐shifting), additional 40% reduction in stroke/CVD incidence and population‐wide prevention strategies, plus 30% stroke/CVD incidence reduction in addition to the motivational mass individual risk prevention strategy regardless of the level of increased CVD risk.