

Acute ST segment elevation myocardial infarction usually occurs when thrombus forms on a ruptured atheromatous plaque and occludes an epicardial coronary artery. Patient survival depends on several factors, the most important being restoration of brisk antegrade coronary flow, the time taken to achieve this, and the sustained patency of the affected artery.
Figure 1.

Histological appearance of a ruptured atheromatous plaque (bottom arrow) and occlusive thrombus (top arrow) resulting in acute myocardial infarction
Recanalisation
There are two main methods of re-opening an occluded artery: administering a thrombolytic agent or primary percutaneous transluminal coronary angioplasty.
Figure 2.

Effects of treatment with placebo, thrombolytic drugs, or primary percutaneous coronary intervention (PCI) on mortality, incidence of cerebrovascular events, and incidence of non-fatal re-infarction after acute myocardial infarction in randomised studies. Of the 1% incidence of cerebrovascular events in patients undergoing primary percutaneous intervention, only 0.05% were haemorrhagic. In contrast patients receiving thrombolytic drugs had a 1% incidence of haemorrhagic cerebrovascular events (P<0.0001) and an overall 2% incidence of cerebrovascular events (P=0.0004)
Although thrombolysis is the commonest form of treatment for acute myocardial infarction, it has important limitations: a rate of recanalisation (restoring normal flow) in 90 minutes of only 55% with streptokinase or 60% with accelerated alteplase; a 5-15% risk of early or late reocclusion leading to acute myocardial infarction, worsening ventricular function, or death; a 1-2% risk of intracranial haemorrhage, with 40% mortality; and 15-20% of patients with a contraindication to thrombolysis.
Table 1.
Comparison of methods of recanalisation
| Thrombolysis | Rescue angioplasty | Primary angioplasty | |
|---|---|---|---|
| Time from admission to recanalisation | 1-3 hours after start of thrombolysis | Time to start of thrombolysis plus 2 hours | 20-60 minutes |
| Recanalisation with brisk antegrade flow | 55-60% | 85% | 95% |
| Systemic fibrinolysis | +++ | +++ | − |
| Staff and catheter laboratory “burden” | − | + | +++ |
| Cost of procedure | + | +++ | +++ |
Primary angioplasty (also called direct angioplasty) mechanically disrupts the occlusive thrombus and compresses the underlying stenosis, rapidly restoring blood flow. It offers a superior alternative to thrombolysis in the immediate treatment of ST segment elevation myocardial infarction. This differs from sequential angioplasty, when angioplasty is performed after thrombolysis. After early trials of thrombolytic drugs, there was much interest in “adjunctive” angioplasty (angioplasty used as a supplement to successful thrombolysis) as this was expected to reduce recurrent ischaemia and re-infarction. Later studies, however, not only failed to show any advantage, but found higher rates of major haemorrhage and emergency bypass surgery. In contrast, “rescue” (also known as “salvage”) angioplasty, which is performed if thrombolysis fails to restore patency after one to two hours, may confer benefit.
Figure 3.

Methods of recanalisation for acute myocardial infarction
Pros and cons of primary angioplasty
Advantages
Large randomised studies have shown that thrombolysis significantly reduces mortality compared with placebo, and this effect is maintained long term. Primary angioplasty confers extra benefits in terms of substantial reductions in rates of death, cerebrovascular events, and re-infarction.
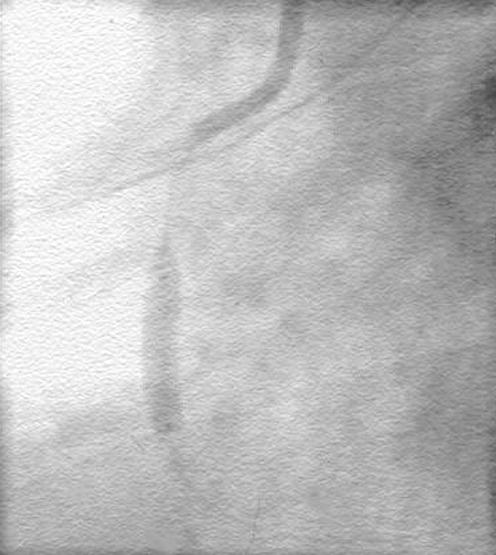
Figure 4.

Severe distal left main stem stenosis (arrow 1) and partially occluded mid-left anterior descending artery due to thrombus (arrow 2). In view of the severity of the lesion salvage angioplasty was contraindicated. An intra-aortic balloon pump was used to augment blood pressure and coronary flow before successful bypass surgery
The information provided by immediate coronary angiography is valuable in determining subsequent management. Patients with severe three vessel disease, severe left main coronary artery stenosis, or occluded vessels unsuitable for angioplasty can be referred for bypass surgery. Conversely, patients whose arteries are found to have spontaneously recanalised or who have an insignificant infarct related artery may be selected for medical treatment, and thus avoid unnecessary thrombolytic treatment.
Table 2.
Pros and cons of primary angioplasty* compared with thrombolysis
| Advantages |
| • High patency rates (> 90%) with brisk, antegrade flow |
| • Lower mortality |
| • Better residual left ventricular function |
| • More rapid electrocardiographic normalisation |
| • Less recurrent ischaemia (angina, reinfarction, exercise induced ischaemia) |
| • No systemic fibrinolysis, therefore bleeding problems avoided |
| • Improved risk stratification by angiography with identification of patients suitable for coronary artery bypass surgery |
| Disadvantages |
| • Higher procedural cost than streptokinase or alteplase (although long term costs lower) |
| • Can be performed only when cardiac catheterisation facilities and experienced staff available |
| • Recanalisation more rapid than thrombolysis only if 24 hour on-call team available |
| • Risks and complications of cardiac catheterisation and percutaneous intervention |
| • Reperfusion arrhythmias probably more common because of more rapid recanalisation |
With or without stenting
Disadvantages
The morbidity and mortality associated with primary angioplasty is operator dependent, varying with the skill and experience of the interventionist, and it should be considered only for patients presenting early (< 12 hours after acute myocardial infarction).
Procedural complications are more common than with elective angioplasty for chronic angina, and, even though it is usual to deal only with the occluded vessel, procedures may be prolonged. Ventricular arrhythmias are not unusual on recanalisation, but these generally occur while the patient is still in the catheterisation laboratory and can be promptly treated by intravenous drugs or electrical cardioversion. Right coronary artery procedures are often associated with sinus arrest, atrioventricular block, idioventricular rhythm, and severe hypotension. Up to 5% of patients initially referred for primary angioplasty require urgent coronary artery bypass surgery, so surgical backup is essential if risks are to be minimised.
There are logistical hurdles in delivering a full 24 hour service. Primary angioplasty can be performed only when adequate facilities and experienced staff are available. The time from admission to recanalisation should be less than 60 minutes, which may not be possible if staff are on call from home. However, recent evidence suggests that, even with longer delays, primary angioplasty may still be superior to thrombolysis.
Figure 5.




Anterior myocardial infarction of 4 hours' duration and severe hypotension, caused by a totally occluded proximal left anterior descending artery (arrow, top left). After treatment with abciximab, a stent was positioned. Initial inflation showed “waisting” of the balloon (top right), due to fibrous lesion resistance, which resolved on higher inflation (bottom left). Successful recanalisation resulted in brisk flow (bottom right), and the 15 minute procedure completely resolved the patient's chest pain
A catheterisation laboratory requires large initial capital expenditure and has substantial running costs. However, in an existing, fully supported laboratory operating at high volume, primary angioplasty is at least as cost effective as thrombolysis.
Primary angioplasty and coronary stents
Although early randomised studies of primary angioplasty showed its clinical effectiveness, outcomes were marred by high rates of recurrent ischaemia (10-15% of patients) and early reinfarction of the affected artery (up to 5%). Consequently, haemodynamic and arrhythmic complications arose, with the need for repeat catheterisation and revascularisation, prolonged hospital stay, and increased costs. Furthermore, restenosis rates in the first six months remained disappointingly high (25-45%), and a fifth of patients required revascularisation.
Although stenting the lesion seemed an attractive answer, it was initially thought that deploying a stent in the presence of thrombus over a ruptured plaque would provoke further thrombosis. However, improvements in stent deployment and advances in adjunctive pharmacotherapy have led to greater technical success. Recent studies comparing primary stenting with balloon angioplasty alone have shown that stented patients have significantly less recurrent ischaemia, reinfarction, and subsequent need for further angioplasty. Economic analysis has shown that, as expected, the initial costs were higher but were offset by lower follow up costs after a year.
However, one study (Stent-PAMI) showed that stenting was associated with a small (but significant) decrease in normal coronary flow and a trend towards increased six and 12 month mortality. This led some to examine the use of adjunctive glycoprotein IIb/IIIa inhibitors as a solution.
Figure 9.



Inferior myocardial infarction of 2.5 hours' duration caused by a totally occluded middle right coronary artery (arrow, top left). A guide wire passed through the fresh thrombus produced slow distal filling (top right). Deployment of a stent (bottom left) resulted in brisk antegrade flow, a good angiographic result, and relief of chest pain (bottom right). A temporary pacemaker electrode was used to counter a reperfusion junctional bradycardia. Note resolution in ST segments compared with top angiograms
Stenting and glycoprotein IIb/IIIa inhibitors
The first study (CADILLAC) to examine the potential benefits of glycoprotein IIb/IIIa inhibitors combined with stenting showed that abciximab significantly reduced early recurrent ischaemia and reocclusion due to thrombus formation. There was no additional effect on restenosis or late outcomes compared with stenting alone. The slightly reduced rate of normal coronary flow that had been seen in other studies was again confirmed, but did not translate into a significant effect on mortality.
Another study (ADMIRAL) examined the potential benefit of abciximab when given before (rather than during) primary stenting. Both at 30 days' and six months' follow up, abciximab significantly reduced the composite rate of reinfarction, the need for further revascularisation, and mortality. In addition, abciximab significantly improved coronary flow rates immediately after stenting, which persisted up to six months with a significant improvement in residual left ventricular function.
Future of primary angioplasty
Primary stenting is not only safe but, by reducing recurrent ischaemic events, also confers advantages over balloon angioplasty alone. Abciximab treatment seems to further improve flow characteristics, prevents distal thrombo–embolisation, and reduces the need for repeat angioplasty. A strategy of primary stenting in association with abciximab seems to be the current gold standard of care for patients with acute myocardial infarction. Future studies will examine the potential benefit of other glycoprotein IIb/IIIa inhibitors. The question of whether on-site surgical cover is still essential for infarct intervention continues to be debated.
Table 3.
Names of trials
| • CADILLAC—Controlled abciximab and device investigation to lower late angioplasty complications |
| • ADMIRAL—Abciximab before direct angioplasty and stenting in myocardial infarction regarding acute and long-term follow-up |
| • Stent-PAMI—Stent primary angioplasty in myocardial infarction |
The ABC of interventional cardiology is edited by Ever D Grech and will be published as a book in summer 2003.
Further reading
- •.Fibrinolytic Therapy Trialists' (FTT) Collaborative Group. Indications for fibrinolytic therapy in suspected acute myocardial infarction: collaborative overview of early mortality and major morbidity results from all randomised trials of more than 1000 patients. Lancet 1994;343: 311-22 [PubMed] [Google Scholar]
- •.Keeley EC, Boura JA, Grines CL. Primary angioplasty versus intravenous thrombolytic therapy for acute myocardial infarction: a quantitative review of 23 randomised trials. Lancet 2003;361: 13-20 [DOI] [PubMed] [Google Scholar]
- •.De Boer MJ, Zijlstra F. Coronary angioplasty in acute myocardial infarction. In: Grech ED, Ramsdale DR, eds. Practical interventional cardiology. 2nd ed. London: Martin Dunitz, 2002: 189-206
- •.Lieu TA, Gurley RJ, Lundstrom RJ, Ray GT, Fireman BH, Weinstein MC, et al. Projected cost-effectiveness of primary angioplasty for acute myocardial infarction. J Am Coll Cardiol 1997;30: 1741-50 [DOI] [PubMed] [Google Scholar]
- •.Grines CL, Cox DA, Stone GW, Garcia E, Mattos LA, Giambartolomei A, et al, for the Stent Primary Angioplasty in Myocardial Infarction Study Group. Coronary angioplasty with or without stent implantation for acute myocardial infarction. N Engl J Med 1999;341: 1949-56 [DOI] [PubMed] [Google Scholar]
- •.Montalescot G, Barragan P, Wittenberg O, Ecollan P, Elhadad S, Villain P, et al. Platelet glycoprotein IIb/IIIa inhibition with coronary stenting for acute myocardial infarction. N Engl J Med 2001;344: 1895-903 [DOI] [PubMed] [Google Scholar]
- •.Stone GW, Grines CL, Cox DA, Garcia E, Tcheng JE, Griffin JJ, et al. Comparison of angioplasty with stenting, with or without abciximab, in acute myocardial infarction. N Engl J Med 2002;346: 957-66 [DOI] [PubMed] [Google Scholar]