
Fig. 5.
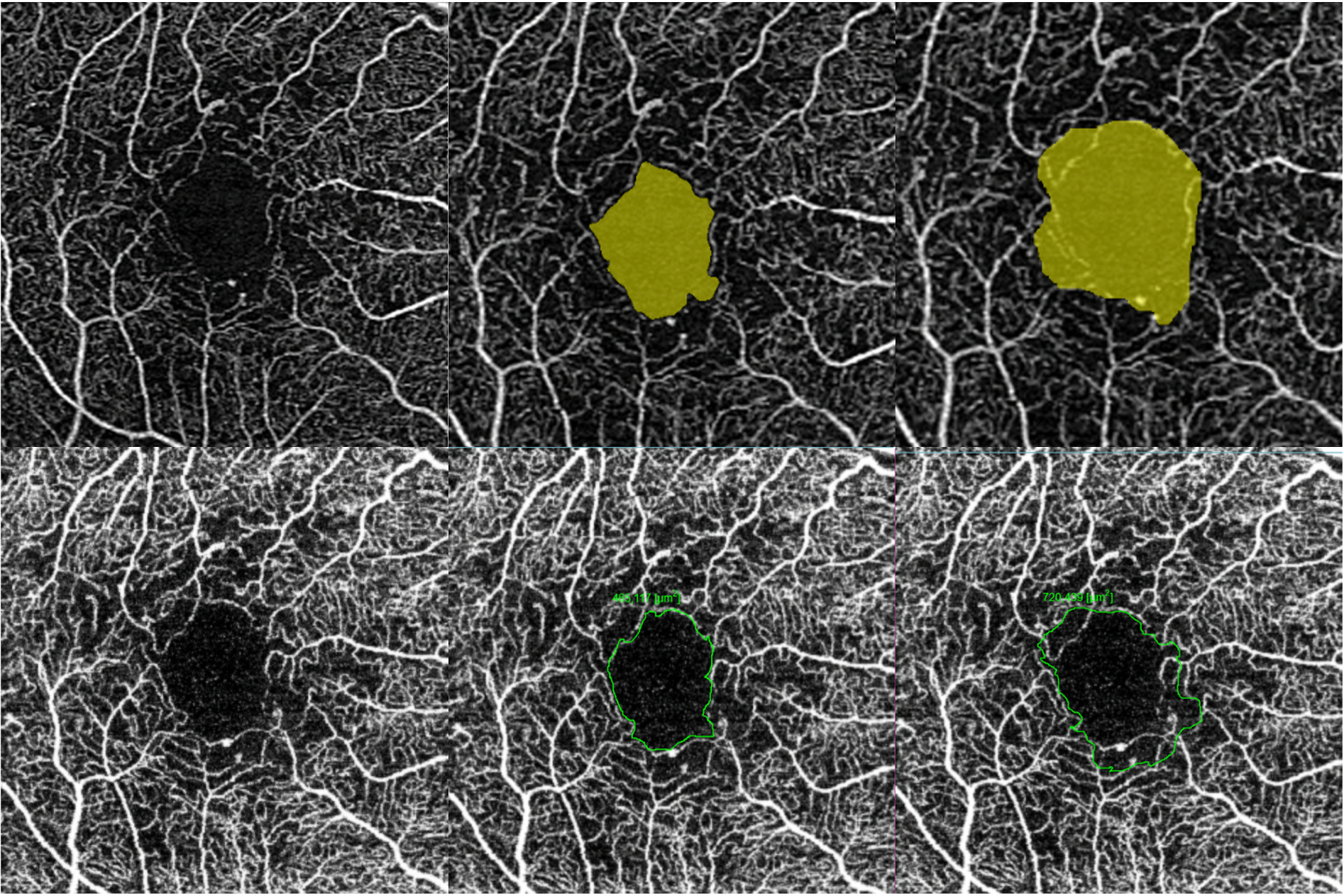
Challenges in interpreting the foveal avascular zone (FAZ) and the associated areas of capillary dropout in the perifoveal area. In this eye with DMI imaged by two commercial OCTA instruments (Top row: Cirrus, Zeiss; bottom row: Triton, Topcon), the true extent of the enlarged FAZ seen in the superficial capillary plexus (SCP) could not be reliably determined. The left-most column shows the original OCTA without delineation of the FAZ. The middle column is a conservative outline of the FAZ, but the perifoveal dropout is not reflected. The right-most column shows the FAZ outline, which considers the “moth-eaten” perifoveal areas where the capillary bed is deficient. This strategy results in a much larger FAZ readout. There is potential for significant variation in the FAZ area readout depending on the inclusion of the perifoveal nonperfusion area. This example illustrates that the FAZ area alone does not adequately describe the severity and the extent of DMI. Additional parameters to ascertain the actual ischaemia include perifoveal intercapillary area, total avascular area and extrafoveal avascular area. DMI = diabetic macular ischaemia; FAZ = foveal avascular zone; OCTA = optical coherence tomography angiography; SCP = superficial capillary plexus.