
Fig. 6.
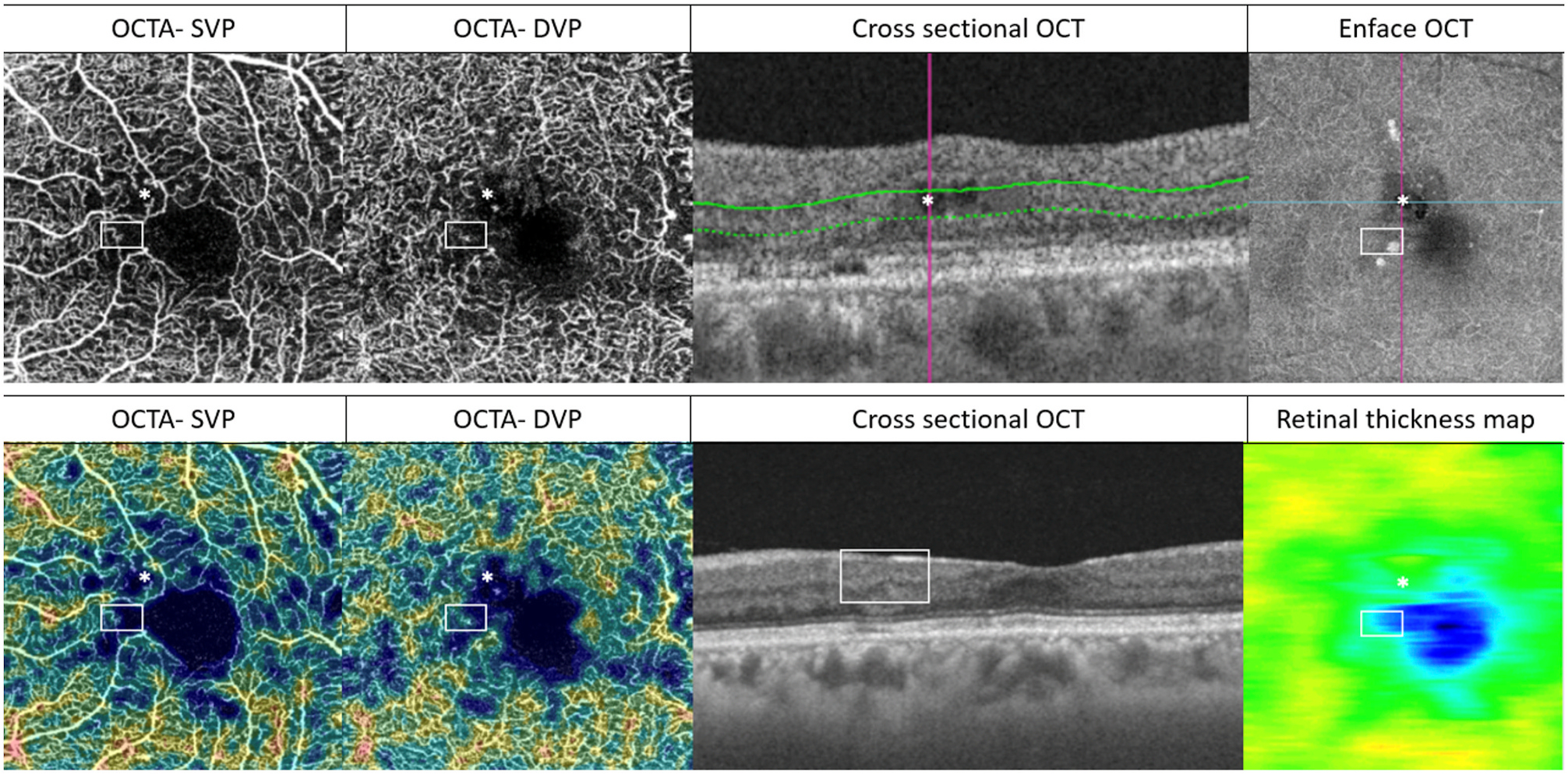
Potential artefacts and inaccurate DMI assessments in eyes with co-existing DMO (upper row) or DRIL (lower row). This figure illustrates the importance of interpreting OCTA with structural OCT (both cross-sectional and en face). A confluent area of perifoveal non-perfusion can be seen. Within this area, two locations (marked by a white asterisk and a white rectangle) are of specific interest. In the upper row, intraretinal cysts (*) can be identified in the structural OCT. The cyst appears as part of the confluent flow void in the superficial and deep layers on OCTA. It is challenging to determine whether this flow void represents the true capillary dropout. In the lower row, the area within the non-perfused area denoted by the rectangular white box on OCTA corresponds to an area of DRIL on cross-sectional OCT. There is corresponding retina thinning on the en-face structural retinal thickness map. It is important in both cases that co-existing structural changes are corrected during segmentation (with manual segmentation performed if necessary) to ensure accurate presentation of flow or non-flow areas on the en-face OCTA scans. The corresponding OCTA density maps are shown on the two left-most images in the bottom row. DMI = diabetic macular ischaemia; DMO = diabetic macular oedema; DRIL = disorganisation of the retinal inner layers; DVP = deep vascular plexus; OCT = optical coherence tomography; OCTA = optical coherence tomography angiography; SVP = superficial vascular plexus.