
Figure 3. Clinical vignettes of patients treated with ICI for AM in the context of concomitant CLL.
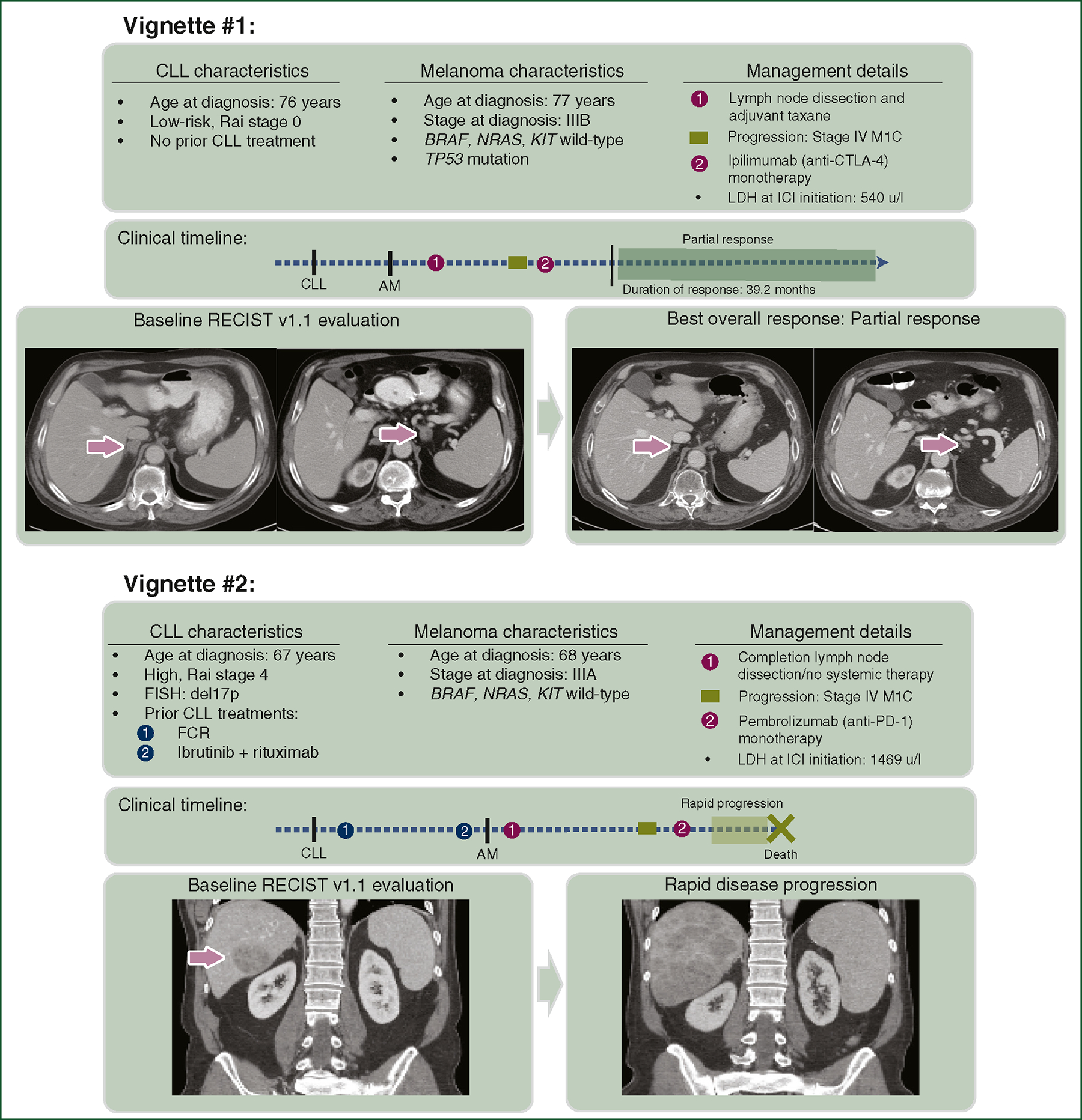
Clinical vignette #1 describes a 76-year-old male who was diagnosed with low-risk CLL and was managed on observation. A year later, he developed a cutaneous melanoma with clinically palpable nodal disease and was managed with wide local excision, lymph node dissection, and adjuvant taxane therapy. Months later, new metastatic disease was identified on surveillance imaging in bilateral adrenal glands. Following treatment with anti-CTLA-4 monotherapy, 3-month post-ICI imaging revealed a near-complete radiographic response. His response has been durable, with no relapse up to the date of this publication. Clinical vignette #2 describes a 67-year-old male who was diagnosed with Rai stage IV CLL with a high-risk 17p deletion by FISH, who was treated, first with combination fludarabine, cyclophosphamide, rituximab, then after CLL progression, with ibrutinib and rituximab. A year later, he developed a cutaneous melanoma treated with wide excision, sentinel lymph node biopsy, and subsequent lymph node dissection due to occult nodal disease. A year later, he developed a large hepatic metastasis and was treated with anti-PD-1 monotherapy. Unfortunately, follow-up imaging demonstrated rapid disease progression.
AM, advanced melanoma; CLL, chronic lymphocytic leukemia; CTLA-4, cytotoxic T-lymphocyte-associated protein 4; ICI, immune checkpoint inhibitor; LDH, lactate dehydrogenase; PD-1, programmed cell death protein 1.