

Abstract
Background:
Despite increasing use of quadriceps tendon (QT) autograft in anterior cruciate ligament (ACL) reconstruction (ACLR), limited data exist regarding its outcomes in high-risk adolescent athletes.
Purpose:
To (1) report the outcomes after QT ACLR in adolescent athletes and (2) identify patient-related and surgery-related factors that may influence failure rates after QT ACLR.
Study Design:
Case series; Level of evidence, 4.
Methods:
All patients aged 14 to 17 years who underwent primary anatomic, transphyseal, single-bundle QT ACLR between 2010 and 2021 with a minimum 2-year follow-up were included for analysis. Demographic and surgical data as well as preoperative International Knee Documentation Committee (IKDC) and Marx activity scores were collected retrospectively. All patients were also contacted to assess postoperative patient-reported outcomes (PROs), including IKDC and Marx activity scores, and return-to-sports (RTS) data. Outcomes of interest included rates of revision ACLR and ipsilateral complications, contralateral ACL tears, difference in pre- and postoperative PROs, and rates of RTS. Patient and surgical characteristics were compared between groups who required revision ACLR versus those who did not.
Results:
A total of 162 patients met inclusion criteria, of which 89 adolescent athletes (mean age 16.2 ± 1.1 years, 64% female) were included for analysis at mean follow-up of 4.0 years. Postoperative IKDC scores were significantly higher than preoperative scores (88.5 vs 37.5; P < .001), whereas Marx activity scores decreased postoperatively (14.3 vs 12.2; P = .011). Successful RTS occurred in 80% of patients at a mean time of 9.7 ± 6.9 months, and 85% of these patients returned to the same or higher level of sports. The most common reasons for failure to RTS included lack of time (n = 7, 70%) and fearing reinjury in the operative knee (n = 5, 50%). The overall revision ACLR rate was 10% (n = 9), and contralateral ACL tears occurred in 14% (n = 12) of patients. The overall ipsilateral knee reoperation rate was 22.5% (n = 20). No statistically significant differences in patient or surgical characteristics were observed between patients who underwent revision ACLR and those who did not.
Conclusion:
At a minimum 2-year follow-up after QT ACLR, adolescent athletes experienced significantly improved postoperative IKDC scores, high rates of RTS, and low rates of graft failure, despite a relatively high ipsilateral reoperation rate. Surgeons may utilize this information when identifying the optimal graft choice for adolescent athletes who have sustained an ACL injury and wish to return to high level of sporting activities.
Keywords: ACL, adolescent athletes, general, knee ligaments, quadriceps tendon
Younger age and increased activity level are some of the well-known risk factors for anterior cruciate ligament (ACL) injury, and failure rates of up to 20% following reconstruction of the ACL have been reported in adolescents 19 years old and younger.4,29,34 As such, more recent attention has been given to modifiable factors, including graft selection, during ACL reconstruction (ACLR) in this population to improve patient-reported outcomes (PROs) and decrease failure rates.
The quadriceps tendon (QT) autograft is being increasingly used in primary ACLR due to its decreased donor site morbidity compared with both bone-patellar tendon-bone and hamstring tendon autografts,5,7,19,20,23,33 and lower failure rates compared with hamstring tendon autograft.23,24 In addition, the QT autograft is a versatile option that can be harvested with or without a patellar bone block and sized appropriately for individualized ACLR.16,27 Despite this, limited data exist regarding outcomes of QT autograft ACLR in the adolescent athlete population. Available evidence indicates failure rates between 1% and 3% after QT autograft ACLR in pediatric and adolescent populations, which may be inconsistent with the higher failure rates of adolescent athletes in particular.3,11,35 In addition, further data regarding postoperative return to sports (RTS) and PROs after QT autograft ACLR remain sparse.11,35
The primary purpose of this study was to present a comprehensive report on outcomes, including PROs, RTS, revision rates, and complications after QT autograft ACLR in adolescent athletes from a single institution with over 10 years of experience with QT autograft ACLR. We hypothesized that patients in this population undergoing QT autograft ACLR would have improved postoperative PROs, high RTS rates, low revision rates, and low complications. The secondary purpose of this study was to identify demographic and surgical factors that differed in the patients who failed QT autograft ACLR versus those who did not. We hypothesized that patients who failed QT autograft ACLR were more likely to be younger, female, and have smaller graft diameters than those who did not fail QT autograft ACLR.
Methods
Retrospective Data Collection
This retrospective study was approved by the institutional review board at the University of Pittsburgh (No. STUDY19030196). All consecutive patients who underwent primary anatomic, transphyseal, single-bundle ACLR with QT autograft between 2010 and 2021 by 1 of 8 sports medicine fellowship-trained orthopaedic surgeons were included for analysis (B.P.L, V.M., J.D.H.). The decision to perform QT autograft ACLR occurred through shared decision-making with the patient, family, and performing surgeon. Exclusion criteria included patients >18 or <14 years old, ACLR performed in patients with an open physis, revision ACLR, double-bundle ACLR, multiligamentous knee reconstruction, and follow-up length <2 years. Demographic data including patient age, sex, body mass index, sport type and level of sport, injury acuity, and laterality of injury; preoperative International Knee Documentation Committee (IKDC) and preoperative Marx activity scores were also collected. Sport type was classified as pivoting (football, basketball, soccer, hockey, cheer/gymnastics, frisbee, and volleyball) versus nonpivoting (baseball/softball, track, skiing, wrestling, and cycling). Level of sport was classified as organized (competitive, varsity, or elite) versus recreational (nonorganized or club). Surgical characteristics including QT autograft diameter, QT autograft thickness (full versus partial), all soft tissue versus bone-block QT autograft, graft diameter to femoral notch width ratio, and concomitant meniscal or chondral procedures at time of primary ACLR were also collected. QT autograft diameter was based on the final width of the autograft pulled through the sizer before insertion.
Additional outcomes collected retrospectively included rates of future ipsilateral knee surgeries, including revision ACLR, medial and lateral meniscal procedures, chondral procedures, knee stiffness (defined as undergoing lysis of adhesions or manipulation under anesthesia), cyclops lesions, hardware removal, wound dehiscence, and patellar fracture. Lachman grade at final follow-up and rates of future contralateral ACLR were also obtained and recorded.
All patients included for analysis were contacted for completion of a questionnaire assessing postoperative PROs (including IKDC and Marx activity scores) and information regarding ability to RTS (including time from surgery to RTS, level of sports participation, and reason for lack of successful RTS). For multisport athletes, RTS was defined as returning to at least 1 sport or starting a new sport postoperatively, whereas level of RTS was defined as highest level of return achieved in at least 1 sport. For patients who did not successfully RTS, multiple reasons were allotted for selection, including lack of clearance to return to play, fear of reinjury, reinjury to ipsilateral or contralateral knee, or a change in interest or lack of availability or time for the sport.
All questionnaires were completed using an institutional REDCap database (REDCap, Vanderbilt University) and stored alongside the retrospective data collected. Follow-up length was determined using date of questionnaire completion or date of last follow-up clinic visit if no questionnaire was completed.
Finally, demographic (age, sex) and surgical (graft diameter, graft thickness, presence of bone block, and concomitant lateral extra-articular tenodesis [LET]) characteristics were compared between those patients who failed primary QT autograft ACLR and those who did not.
Surgical Technique for ACLR
All patients underwent primary, anatomic, transphyseal, single-bundle ACLR with ipsilateral QT autograft. Diagnostic arthroscopy was performed to confirm the presence of an ACL tear and evaluate for concomitant meniscal or chondral pathology, which were treated appropriately. The QT autograft was harvested just lateral to the vastus medialis oblique muscle, and graft thickness, diameter, and harvest of patellar bone block were determined based on surgeon discretion. The native ACL femoral and tibial footprints were visualized. The femoral tunnel was drilled through the anteromedial portal in the center of the anatomic ACL footprint, and the tibial tunnel was drilled via an outside-in technique using a tibial guide. The QT autograft was passed and fixed appropriately on the femoral and tibial sides utilizing continuous or adjustable loop suspensory fixation or interference screws, based on surgeon-specific technique, with a posterior drawer force applied.
Patients were allowed weightbearing as tolerated immediately after surgery unless a concomitant meniscal repair was performed, in which case patients were instructed to remain toe-touch weightbearing for 6 weeks. All patients used a hinged knee brace for 6 weeks postoperatively, after which time the brace was discontinued. The patients progressed through a stepwise physical therapy protocol that was dictated on patient progress and milestones. In general, the patients were allowed light straight-line jogging at 3 months, running at 4 months, and pivoting and sport-specific drills at 6 months. The patients were released to full sport at a minimum of 9 months postoperatively based on progress with physical therapy and passing specific objective criteria, including strength symmetry of 90% and functional testing.8,14,22
Statistical Analysis
All data were analyzed using Microsoft Excel (Version 16.6) and SPSS Version 28 (IBM). Descriptive statistics were reported for all demographic variables, surgical characteristics, and postoperative outcomes and displayed as means with standard deviations or numbers with percentages. Differences in demographic and surgical variables between groups with and without ipsilateral ACLR failure were assessed using the independent t test or Mann-Whitney U test for parametric and nonparametric data, respectively, and chi-square test for dichotomous variables. Due to multiple comparisons being performed between the groups, significance level was adjusted with Bonferroni correction to a level of P = .008.
Results
Patient Cohort and Surgical Characteristics
After exclusion criteria were applied, a total of 162 patients met inclusion criteria, of which 89 patients (55%) with minimum 2-year follow-up were ultimately included for analysis (Figure 1). The mean age and body mass index of the cohort were 16.2 ± 1.1 years and 23.8 ± 4.3 kg/m2, respectively. A total of 64% of patients were female (Table 1); 76 (85.4%) patients participated in a pivoting sport at time of injury, and 78 (87.6%) patients participated in organized (versus recreational) sports. The mean time to surgery was 1.8 ± 3.0 months, and the mean follow-up length was 4.0 ± 2.1 years.
Figure 1.
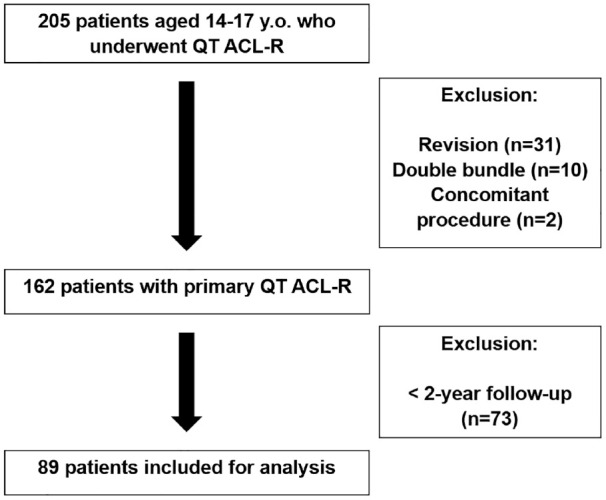
Flowchart of inclusion and exclusion criteria. ACL, anterior cruciate ligament, ACLR, anterior cruciate ligament reconstruction; QT, quadriceps tendon.
Table 1.
Descriptive Characteristics of Patient Demographics a
| Variable | Total Cohort (n = 89) |
|---|---|
| Age, y | 16.2 (1.1) |
| Sex (female), n (%) | 57 (64.0) |
| BMI, kg/m2 | 23.8 (4.3) |
| Laterality (right), n (%) | 42 (47.2) |
| Preinjury sport type (pivoting), n (%) b | 76 (85.4) |
| Level of sport (organized), n (%) c | 78 (87.6) |
| Time to surgery, mo | 1.8 (3.0) |
| Follow-up length, y | 4.0 (2.1) |
Data presented as mean (SD) unless otherwise indicated. BMI, body mass index.
Reported as percentage of pivoting versus nonpivoting sport at time of injury.
Reported as percentage of organized (competitive, varsity, or elite) versus nonorganized (nonorganized or recreational) sport at time of injury.
Isolated, primary QT autograft ACLR was performed in 43 (48.3%) patients, with concomitant medial meniscal procedure in 20 (22.5%) patients, lateral meniscal procedure in 33 (37.1%) patients, and LET in 6 (6.7%) patients (Table 2). Of patients with concomitant meniscal tears, 6 had lateral meniscal root tears. All meniscal tears underwent meniscal repair. The mean QT graft length and diameter was 74.1 ± 13.5 mm and 9.4 ± 0.8 mm, respectively. There was no difference in graft diameter observed between male and female patients (9.4 mm vs 9.3 mm; P = .674). In addition, 18 (20.2%) grafts were harvested with a patellar bone block, and 24 (27.0%) were partial thickness grafts. The mean notch width of patients was 16.1 ± 2.4 mm; mean graft diameter to notch width ratio of 0.6 ± 0.1.
Table 2.
Descriptive Characteristics of Primary Quadriceps Tendon ACLR Variables a
| Variable | n | Total Cohort |
|---|---|---|
| Prehab (yes), n (%) | 89 | 24 (27.0) |
| QT graft properties | ||
| Length, mm | 89 | 74.1 (13.5) |
| Diameter, mm | 89 | 9.4 (0.8) |
| Bone block (yes), n (%) | 89 | 18 (20.2) |
| Thickness (partial), n (%) | 89 | 24 (27.0) |
| Notch width, mm | 79 | 16.1 (2.4) |
| Diameter-to-notch ratio, mm | 79 | 0.6 (0.1) |
| Concomitant medial meniscus, n (%) | 89 | 20 (22.5) |
| Concomitant lateral meniscus, n (%) | 89 | 33 (37.1) |
| Concomitant LET, n (%) | 89 | 6 (6.7) |
| Tourniquet (yes), n (%) | 89 | 81 (91.0) |
| Tourniquet time, minutes | 81 | 93.6 (23.1) |
Data presented as mean (SD) unless otherwise indicated. ACLR, anterior cruciate ligament reconstruction; QT, quadriceps tendon; LET, lateral extra-articular tenodesis.
Patient-Reported Outcomes
Out of the total cohort, 71 (80%) patients completed postoperative PRO questionnaires. The mean preoperative IKDC and preoperative Marx activity scores were 37.2 ± 17.1 and 14.3 ± 3.1, respectively (Appendix Table 1). Postoperatively, mean IKDC scores increased to 87.5 ± 12.6, while mean Marx activity scores decreased to 12.2 ± 4.6. Patients with available pre- and postoperative IKDC scores achieved a significant increase in postoperative IKDC scores (88.5 vs 37.5; P < .001). Patients with available pre- and postoperative Marx activity scores had a significant decrease in postoperative Marx activity scores (14.3 vs 12.2; P = .011).
Return to Sports
Out of the total cohort, 50 (56.2%) patients completed the RTS questionnaire (Table 3), of whom 40 (80.0%) reported successful RTS at a mean time of 9.7 ± 6.9 months and median time of 6.7 months, which may be due to several patients returning without surgeon clearance. Among patients who RTS, 34 (85.0%) returned to the same or higher level of sport. Among the 10 patients who failed to RTS, the most common reasons for not returning included changing interests or lack of time (n = 7, 70.0%) and fearing reinjury or lacking confidence in the operative knee (n = 5, 50.0%). Other reasons included reinjury to the same knee (n = 2, 20.0%) and not being cleared to play (n = 1, 10.0%).
Table 3.
Descriptive Characteristics of RTS at Minimum 2-Year Follow-up a
| Variable | Total Respondents (n = 50) |
|---|---|
| RTS (yes) | 40 (80.0) |
| Level of RTS (same or higher) b | 34 (85.0) |
| Time to RTS, months, mean (SD) | 9.7 (6.9) |
| Reason for failure to RTS c | |
| Not cleared to play | 1 (10.0) |
| Too fearful of reinjury | 5 (50.0) |
| Interests have changed | 7 (70.0) |
| Reinjury to same knee | 2 (20.0) |
| Reinjury to opposite knee | 0 (0.0) |
| Sport not available | 0 (0.0) |
| Other | 2 (20.0) |
Data presented as number (%) unless otherwise indicated. Characteristics are reported among survey respondents. RTS, return to sports.
Reported as percentage of patients who returned to same or higher level of sport among those who successfully returned to sports (n = 40).
Reported as percentage of patients who failed to RTS (n = 10). Patients were able to list multiple reasons for failing to RTS.
Complications and Subsequent Surgeries
The overall revision ACLR rate was 10.1% (n = 9), and 13.5% (n = 12) of patients sustained contralateral ACL tears. No statistically significant differences in age, sex, or graft diameter were observed between patients who underwent ipsilateral revision ACLR and those who did not (Appendix Table 2). Additional ipsilateral knee reoperations occurred in 20 (22.5%) of patients, with the most common reasons for reoperation being postoperative loss of range of motion due to knee stiffness or cyclops lesions (n = 8, 8.9%) and meniscal surgery (n = 8, 8.9%) (Table 4). Among patients who underwent subsequent meniscal surgery, 6 sustained retear of previously repaired meniscal injury (87% success rate), whereas 2 sustained new ipsilateral meniscal injury. At final follow-up, 83 (93.3%) patients had Lachman grade 1A or less and 6 (6.7%) patients had Lachman grade 2A.
Table 4.
Descriptive Characteristics of Complications and Subsequent Knee Surgeries a
| Variable | Total Cohort (n = 89) |
|---|---|
| Lachman at final follow-up b | |
| Grade 1A or less | 83 (93.3) |
| Grade 2A | 6 (6.7) |
| Ipsilateral revision ACLR | 9 (10.1) |
| Other ipsilateral knee surgeries | |
| Stiffness | 2 (2.2) |
| Cyclops lesion | 6 (6.7) |
| Medial meniscus | 4 (4.5) |
| Lateral meniscus | 4 (4.5) |
| Wound dehiscence | 1 (1.1) |
| Hardware removal | 3 (3.4) |
| Contralateral ACLR | 12 (13.5) |
Data are presented as n (%). ACLR, anterior cruciate ligament reconstruction.
For patients who sustained ipsilateral failure and subsequent revision ACLR, Lachman grade at final follow-up before ACLR failure was used.
Discussion
The most important finding of the present study was the favorable outcomes after QT autograft ACLR in high-risk adolescent patients. At minimum 2-year follow-up, adolescent patients experienced significantly improved postoperative IKDC scores, high rates of RTS of 80%, and low ipsilateral graft failure rates of 10%. Further, an ipsilateral reoperation rate of 22% was identified in this cohort of high-risk adolescent athletes. Altogether, the findings of this study suggest that the QT is a viable graft choice for primary ACLR in adolescent athletes who wish to return to a high level of sporting activities.
Despite the recent rise in use of QT in primary and revision ACLR settings, 33 there remains limited evidence regarding the outcomes of QT ACLR in adolescent patients. Available data of small case series and systematic reviews suggest failure rates of 0% to 3% after QT ACLR in adolescent patients.11,35 However, younger age is a well-known risk factor for ipsilateral ACLR failure, 29 and adolescent athletes present a high-risk population for revision ACLR given the high level of sporting activities in this age group. 31 As a result, these studies may underestimate the true failure rate after ACLR in active and competitive adolescent athletes who wish to RTS, which has previously been reported in the range of 9% to 19% after use of autograft in ACLR.6,9,13,28 In the present study of competitive adolescent athletes, most of whom participated in pivoting sports, the ipsilateral revision ACLR rate was 10.1%, which was similar to previously reported rates in active adolescents 17 and lower than the contralateral ACL rupture rate of 13.5%. This demonstrates that the QT was effective in restoring rotatory knee stability and biomechanics to the operative knee.
In the present study, 80% of patients successfully returned to sports at a mean time of 9.7 months, of which 85% of patients returned to the same or higher level of activity postoperatively. The observed rate of RTS was similar to previously reported rates of RTS among adolescent athletes after ACLR with QT and other autografts, ranging from 60% to 100%.10,12,17,32 However, the present study may be limited by the low follow-up rate for RTS data among our cohort of patients, which has the potential to introduce bias. Among patients who did not successfully RTS, the most common reasons included changing interests, fearing reinjury, or lacking confidence in the operative knee. The latter is especially important, as recent evidence suggests psychological readiness significantly impacts ability and success of RTS.10,30 Previous studies have identified that lower psychological readiness to RTS was associated with higher risk for a second ACL injury, failure to RTS, and failure to return to preinjury level of activity after RTS.1,18,21 In this study, 50% of the patients who did not RTS identified lack of confidence in the operative knee as a contributing factor to their inability to RTS, highlighting the continued importance of, and need for, postoperative psychological testing to guide patients toward successful RTS.
When comparing patients requiring revision ACLR versus those who did not, no significant differences in patient or surgical characteristics were found, thus refuting our second hypothesis (Appendix Table 2). However, given the small effect sizes of this particular analysis, more research with a larger number of patients is needed to draw firmer conclusions on factors that differ between those adolescents who fail primary QT autograft ACLR and those who do not.
Overall, the QT autograft provides a favorable option for adolescent athletes undergoing ACLR. In addition to its large size and low donor site morbidity,19,20,23,25 the results of the present study show acceptable outcomes in this adolescent athlete cohort of patients. As evidenced by the significant improvement in postoperative PROs, high RTS rate, and low ipsilateral failure rate, the QT autograft can be considered as a graft choice for ACLR in the adolescent athlete. While a relatively high ipsilateral reoperation rate of 22% was identified, the majority of these reoperations were due to subsequent meniscal injuries, which are increased among high-risk adolescent athletes, or postoperative loss of range of motion. Further, while the QT autograft has been linked to a potential increase in rates of knee stiffness and development of cyclops lesions relative to other autografts, 15 the data are conflicting and currently limited in evidence.2,26
There are several limitations to the present study worth mentioning. First, we had a 55% follow-up rate at minimum 2-year follow-up, which may influence our results. Second, the study is retrospective in nature, and there was a lack of a control group to identify comparisons between QT and other autograft choices. Third, data regarding pivot shift grade were not included because the pivot shift examination was not performed routinely after surgery, resulting in inconsistent recording in our cohort. Fourth, although the present study included only QT ACLR performed by high-volume sports fellowship-trained surgeons, there may be heterogeneity in the techniques utilized during surgery, which has the potential to impact the observed results. Fifth, we utilized survey responses to assess PROs and RTS data, and the responses received in the present study may not be representative of the entire study population, especially with regard to RTS data and specific reasons for lack of RTS. Given the low follow-up rate with regard to RTS data (50/162 eligible patients), it is possible that patients who sustained ipsilateral ACL retear were less likely to complete the questionnaire, which may have resulted in an elevated RTS rate in our cohort. Finally, our comparison between patients who sustained ipsilateral ACLR failure and those who did not was likely underpowered to detect differences between groups, and further research with larger numbers of patients will be needed to further elucidate comparisons between adolescents who fail primary QT autograft ACLR and those who do not.
Conclusion
The QT autograft is a viable option for primary ACLR in adolescent athletes. At average 4-year follow-up, adolescent athletes experienced significantly improved postoperative IKDC scores, high rates of RTS, and low rates of graft failure, despite a relatively high ipsilateral reoperation rate. Surgeons may utilize this information when considering graft choices for adolescent athletes who have sustained ACL injury and wish to return to high level of sporting activities.
Appendix Table 1.
Descriptive Characteristics of Preoperative and Postoperative Patient-Reported Outcomes at Minimum 2-Year Follow-up a
| Variable | n | Total Cohort |
|---|---|---|
| Preoperative IKDC | 37 | 37.2 (17.1) |
| Postoperative IKDC | 71 | 87.5 (12.6) |
| IKDC difference | 37 | 51.0 (21.8) |
| Preoperative Marx | 63 | 14.3 (3.1) |
| Postoperative Marx | 71 | 12.2 (4.6) |
| Marx difference | 63 | 2.0 (4.9) |
Data are presented as mean (SD). IKDC, International Knee Documentation Committee; Marx, Marx activity rating scale.
Appendix Table 2.
Comparison of Demographic and Surgical Variables Between Patients Requiring Revision and No Revision ACLR a
| Variable | Revision ACLR (n = 9) | No Revision ACLR (n = 80) | P value b | Effect Size |
|---|---|---|---|---|
| Age, y | 16.9 (1.1) | 16.2 (1.0) | .044 | -0.71 |
| Sex (female), n (%) | 3 (33.3) | 54 (67.5) | .043 | 0.22 |
| Graft diameter, mm | 9.3 (0.8) | 9.4 (0.8) | .638 | 0.16 |
| QT with bone block (yes), n (%) | 4 (44.4) | 14 (17.5) | .056 | 0.20 |
| Graft thickness (partial), n (%) | 3 (33.3) | 21 (26.3) | .650 | 0.05 |
| Concomitant LET (yes), n (%) | 0 (0.0) | 6 (7.5) | .395 | 0.09 |
Data presented as mean (SD) unless otherwise indicated. ACLR, anterior cruciate ligament reconstruction; QT, quadriceps tendon; LET, lateral extra-articular tenodesis.
Bonferroni-adjusted significance level of P = .008 for multiple comparisons.
Footnotes
Final revision submitted December 1, 2023; accepted December 6, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: L.M. has received a grant from Arthrex; education payments from Mid-Atlantic Surgical Systems and Smith+Nephew; and hospitality payments from Stryker. B.P.L. has received education payments from Mid-Atlantic Surgical Systems. V.M. reports educational grants, consulting fees, and speaking fees from Smith+Nephew; educational grants from Arthrex and DePuy Synthes; is a board member of the International Society of Arthroscopy, Knee Surgery and Orthopaedic Sports Medicine (ISAKOS); and deputy editor-in-chief of Knee Surgery, Sports Traumatology, Arthroscopy (KSSTA). J.D.H. is on the editorial board of KSSTA. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the University of Pittsburgh (ref No. STUDY19030196).
ORCID iDs: Sahil Dadoo  https://orcid.org/0000-0003-0397-6220
https://orcid.org/0000-0003-0397-6220
Jonathan D. Hughes https://orcid.org/0000-0002-1298-7514
References
- 1. Ardern CL, Osterberg A, Tagesson S, Gauffin H, Webster KE, Kvist J. The impact of psychological readiness to return to sport and recreational activities after anterior cruciate ligament reconstruction. Br J Sports Med. 2014;48(22):1613-1619. [DOI] [PubMed] [Google Scholar]
- 2. Arner JW. Editorial commentary: risk factors of cyclops syndrome in quadriceps autograft anterior cruciate ligament reconstruction: more helpful data in weighing graft choice. Arthroscopy. 2023;39(6):1480-1482. [DOI] [PubMed] [Google Scholar]
- 3. Barrett AM, Craft JA, Replogle WH, Hydrick JM, Barrett GR. Anterior cruciate ligament graft failure: a comparison of graft type based on age and Tegner activity level. Am J Sports Med. 2011;39(10):2194-2198. [DOI] [PubMed] [Google Scholar]
- 4. Borchers JR, Pedroza A, Kaeding C. Activity level and graft type as risk factors for anterior cruciate ligament graft failure: a case-control study. Am J Sports Med. 2009;37(12):2362-2367. [DOI] [PubMed] [Google Scholar]
- 5. Dai W, Leng X, Wang J, Cheng J, Hu X, Ao Y. Quadriceps tendon autograft versus bone-patellar tendon-bone and hamstring tendon autografts for anterior cruciate ligament reconstruction: a systematic review and meta-analysis. Am J Sports Med. 2022;50(12):3425-3439. [DOI] [PubMed] [Google Scholar]
- 6. Dekker TJ, Godin JA, Dale KM, Garrett WE, Taylor DC, Riboh JC. Return to sport after pediatric anterior cruciate ligament reconstruction and its effect on subsequent anterior cruciate ligament injury. J Bone Joint Surg Am. 2017;99(11):897-904. [DOI] [PubMed] [Google Scholar]
- 7. Diermeier T, Tisherman R, Hughes J, et al. Quadriceps tendon anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc. 2020;28(8):2644-2656. [DOI] [PubMed] [Google Scholar]
- 8. Drigny J, Ferrandez C, Gauthier A, et al. Knee strength symmetry at 4 months is associated with criteria and rates of return to sport after anterior cruciate ligament reconstruction. Ann Phys Rehabil Med. 2022;65(4):101646. [DOI] [PubMed] [Google Scholar]
- 9. Engelman GH, Carry PM, Hitt KG, Polousky JD, Vidal AF. Comparison of allograft versus autograft anterior cruciate ligament reconstruction graft survival in an active adolescent cohort. Am J Sports Med. 2014;42(10):2311-2318. [DOI] [PubMed] [Google Scholar]
- 10. Fones L, Kostyun RO, Cohen AD, Pace JL. Patient-reported outcomes, return-to-sport status, and reinjury rates after anterior cruciate ligament reconstruction in adolescent athletes: minimum 2-year follow-up. Orthop J Sports Med. 2020;8(11):2325967120964471. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Gagliardi AG, Carry PM, Parikh HB, Albright JC. Outcomes of quadriceps tendon with patellar bone block anterior cruciate ligament reconstruction in adolescent patients with a minimum 2-year follow-up. Am J Sports Med. 2020;48(1):93-98. [DOI] [PubMed] [Google Scholar]
- 12. Geffroy L, Lefevre N, Thevenin-Lemoine C, et al. Return to sport and re-tears after anterior cruciate ligament reconstruction in children and adolescents. Orthop Traumatol Surg Res. 2018;104(8S):S183-S188. [DOI] [PubMed] [Google Scholar]
- 13. Ho B, Edmonds EW, Chambers HG, Bastrom TP, Pennock AT. Risk factors for early ACL reconstruction failure in pediatric and adolescent patients: a review of 561 cases. J Pediatr Orthop. 2018;38(7):388-392. [DOI] [PubMed] [Google Scholar]
- 14. Hughes JD, Burnham JM, Hirsh A, et al. Comparison of short-term biodex results after anatomic anterior cruciate ligament reconstruction among 3 autografts. Orthop J Sports Med. 2019;7(5):2325967119847630. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Huleatt J, Gottschalk M, Fraser K, et al. Risk factors for manipulation under anesthesia and/or lysis of adhesions after anterior cruciate ligament reconstruction. Orthop J Sports Med. 2018;6(9):2325967118794490. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Kaeding CC, Leger-St-Jean B, Magnussen RA. Epidemiology and diagnosis of anterior cruciate ligament injuries. Clin Sports Med. 2017;36(1):1-8. [DOI] [PubMed] [Google Scholar]
- 17. Kay J, Memon M, Marx RG, Peterson D, Simunovic N, Ayeni OR. Over 90% of children and adolescents return to sport after anterior cruciate ligament reconstruction: a systematic review and meta-analysis. Knee Surg Sports Traumatol Arthrosc. 2018;26(4):1019-1036. [DOI] [PubMed] [Google Scholar]
- 18. Kitaguchi T, Tanaka Y, Takeshita S, et al. Importance of functional performance and psychological readiness for return to preinjury level of sports 1 year after ACL reconstruction in competitive athletes. Knee Surg Sports Traumatol Arthrosc. 2020;28(7):2203-2212. [DOI] [PubMed] [Google Scholar]
- 19. Lind M, Nielsen TG, Soerensen OG, Mygind-Klavsen B, Fauno P. Quadriceps tendon grafts does not cause patients to have inferior subjective outcome after anterior cruciate ligament (ACL) reconstruction than do hamstring grafts: a 2-year prospective randomised controlled trial. Br J Sports Med. 2020;54(3):183-187. [DOI] [PubMed] [Google Scholar]
- 20. Lund B, Nielsen T, Fauno P, Christiansen SE, Lind M. Is quadriceps tendon a better graft choice than patellar tendon? A prospective randomized study. Arthroscopy. 2014;30(5):593-598. [DOI] [PubMed] [Google Scholar]
- 21. McPherson AL, Feller JA, Hewett TE, Webster KE. Psychological readiness to return to sport is associated with second anterior cruciate ligament injuries. Am J Sports Med. 2019;47(4):857-862. [DOI] [PubMed] [Google Scholar]
- 22. Meredith SJ, Rauer T, Chmielewski TL, et al. Return to sport after anterior cruciate ligament injury: Panther Symposium ACL Injury Return to Sport Consensus Group. J ISAKOS. 2021;6(3):138-146. [DOI] [PubMed] [Google Scholar]
- 23. Mouarbes D, Menetrey J, Marot V, Courtot L, Berard E, Cavaignac E. Anterior cruciate ligament reconstruction: a systematic review and meta-analysis of outcomes for quadriceps tendon autograft versus bone-patellar tendon-bone and hamstring-tendon autografts. Am J Sports Med. 2019;47(14):3531-3540. [DOI] [PubMed] [Google Scholar]
- 24. Nyland J, Collis P, Huffstutler A, et al. Quadriceps tendon autograft ACL reconstruction has less pivot shift laxity and lower failure rates than hamstring tendon autografts. Knee Surg Sports Traumatol Arthrosc. 2020;28(2):509-518. [DOI] [PubMed] [Google Scholar]
- 25. Offerhaus C, Albers M, Nagai K, et al. Individualized anterior cruciate ligament graft matching: in vivo comparison of cross-sectional areas of hamstring, patellar, and quadriceps tendon grafts and ACL insertion area. Am J Sports Med. 2018;46(11):2646-2652. [DOI] [PubMed] [Google Scholar]
- 26. Ouweleen AJ, Hall TB, Finlayson CJ, Patel NM. Predictors of arthrofibrosis after pediatric anterior cruciate ligament reconstruction: what is the impact of quadriceps autograft? J Pediatr Orthop. 2021;41(7):395-399. [DOI] [PubMed] [Google Scholar]
- 27. Setliff JC, Nazzal EM, Drain NP, et al. Anterior cruciate ligament reconstruction with all-soft tissue quadriceps tendon versus quadriceps tendon with bone block. Knee Surg Sports Traumatol Arthrosc. 2023;31(7):2844-2851. [DOI] [PubMed] [Google Scholar]
- 28. Shelbourne KD, Sullivan AN, Bohard K, Gray T, Urch SE. Return to basketball and soccer after anterior cruciate ligament reconstruction in competitive school-aged athletes. Sports Health. 2009;1(3):236-241. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Webster KE, Feller JA. Exploring the high reinjury rate in younger patients undergoing anterior cruciate ligament reconstruction. Am J Sports Med. 2016;44(11):2827-2832. [DOI] [PubMed] [Google Scholar]
- 30. Webster KE, Feller JA. Psychological readiness to return to sport after anterior cruciate ligament reconstruction in the adolescent athlete. J Athl Train. 2022;57(9-10):955-960. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Webster KE, Feller JA, Leigh WB, Richmond AK. Younger patients are at increased risk for graft rupture and contralateral injury after anterior cruciate ligament reconstruction. Am J Sports Med. 2014;42(3):641-647. [DOI] [PubMed] [Google Scholar]
- 32. Webster KE, McPherson AL, Hewett TE, Feller JA. Factors associated with a return to preinjury level of sport performance after anterior cruciate ligament reconstruction surgery. Am J Sports Med. 2019;47(11):2557-2562. [DOI] [PubMed] [Google Scholar]
- 33. Winkler PW, Vivacqua T, Thomassen S, et al. Quadriceps tendon autograft is becoming increasingly popular in revision ACL reconstruction. Knee Surg Sports Traumatol Arthrosc. 2022;30(1):149-160. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Yellin JL, Parisien RL, Talathi NS, Farooqi AS, Kocher MS, Ganley TJ. Narrow notch width is a risk factor for anterior cruciate ligament injury in the pediatric population: a multicenter study. Arthrosc Sports Med Rehabil. 2021;3(3):e823-e828. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. Zakharia A, Lameire DL, Abdel Khalik H, et al. Quadriceps tendon autograft for pediatric anterior cruciate ligament reconstruction results in promising postoperative function and rates of return to sports: a systematic review. Knee Surg Sports Traumatol Arthrosc. 2022;30(11):3659-3672. [DOI] [PubMed] [Google Scholar]