

Computed tomography imaging of complex double-outlet right ventricle with TGA and a VSD.
Central Message.
A Bex-Nikaidoh procedure is feasible for complex TGA with VSD and left ventricular outflow tract obstruction with the relative contraindication of posterior coronary artery looping related to risk of coronary artery injury.
Aortic root translocation for correction of transposition of the great arteries (TGA) with associated ventricular septal defects (VSDs) and pulmonic stenosis was described by Bex and colleagues1 in 1980 and Nikaidoh2 in 1984. Abnormal coronary anatomy with posterior looping around the great vessels and crossing atrioventricular valve structures have been considered contraindications; however, there have been reports of success with such variants.3 We present a patient with double-outlet right ventricle and TGA with pulmonic stenosis, VSD, crossing papillary muscle, and aberrant coronary anatomy who successfully underwent the Bex-Nikaidoh procedure.
Case
A 22-month-old with double-outlet right ventricle, TGA, and subpulmonic VSD presented as a neonate after balloon atrial septostomy (Figure 1). Preoperative computed tomography angiography showed the left anterior descending artery arising from the leftward anterior sinus of Valsalva and the right coronary artery and left circumflex from the posterior sinus with a retro-pulmonic course (Figure 2). Echocardiography showed the anterior papillary muscle of the tricuspid valve straddling the VSD originating from the infundibular septum.
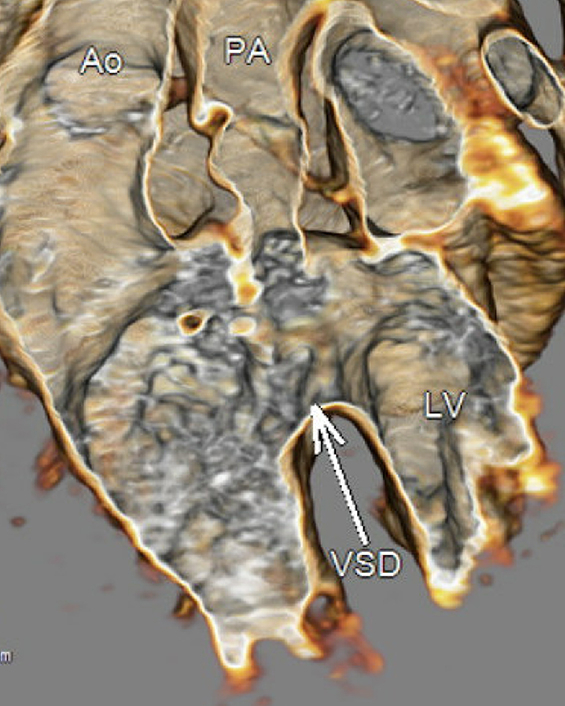
Figure 1.

Computed tomography scan reconstructed image displaying orientation of great vessels and relation to the VSD. Ao, Aorta; PA, pulmonary artery; LV, left ventricle; VSD, ventricular septal defect.
Figure 2.

Computed tomography scan reconstructed imaging of coronary artery position. LAD, Left anterior descending artery; PA, pulmonary artery; RCA, right coronary artery; Cx, circumflex artery.
After sternotomy, bicaval cannulation, and cardioplegic arrest, a right atriotomy was performed. Coronary buttons were harvested. The pulmonary valve leaflets were excised. The papillary muscle was detached from the infundibular septum before septal division. The neoaortic root was translocated posteriorly. A bovine patch was used to close the VSD. The papillary muscle was reimplanted into the VSD patch. Coronary buttons were implanted into the facing sinuses with anterior patch augmentation. A right ventricle to pulmonary artery conduit was created using an aortic homograft. The tricuspid valve was repaired with a commisuroplasty, and the atrial septal defect was closed (Video 1). The patient was successfully weaned from cardiopulmonary bypass and transferred to the intensive care unit. Discharge echocardiograms showed normal biventricular function.
Conclusions
A modified Bex-Nikaidoh operation can be performed successfully despite posterior looping of the coronary artery and papillary muscle crossing the VSD.
Webcast
You can watch a Webcast of this AATS meeting presentation by going to: https://www.aats.org/resources/modified-bex-nikaidoh-procedur-7364.

Conflict of Interest Statement
The authors reported no conflicts of interest.
The Journal policy requires editors and reviewers to disclose conflicts of interest and to decline handling or reviewing manuscripts for which they may have a conflict of interest. The editors and reviewers of this article have no conflicts of interest.
Footnotes
The Institutional Review Board of the Medical University of South Carolina did not review this study because it is a singular retrospective report that did not meet review requirements. Patient written consent for the publication of the study was not required due to removal of all unique identifiers meeting Health Insurance Portability and Accountability standards.
Supplementary Data
Demonstration of key steps in the modified Bex-Nikaidoh operation. Video available at: https://www.jtcvs.org/article/S2666-2507(24)00227-X/fulltext.
{kind=link}
References
- 1.Bex J.P., Lecompte Y., Baillot F., Hazan E. Anatomical correction of transposition of the great arteries. Ann Thorac Surg. 1980;29(1):86–88. doi: 10.1016/s0003-4975(10)61636-0. [DOI] [PubMed] [Google Scholar]
- 2.Nikaidoh H. Aortic translocation and biventricular outflow tract reconstruction. A new surgical repair for transposition of the great arteries associated with ventricular septal defect and pulmonary stenosis. J Thorac Cardiovasc Surg. 1984;88(3):365–372. [PubMed] [Google Scholar]
- 3.Agarwal V., Vaidyanathan S. Aortic root translocation: the Bex-Nikaidoh procedure. Indian J Thorac Cardiovasc Surg. 2021;37(Suppl 1):36–41. doi: 10.1007/s12055-020-00956-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Demonstration of key steps in the modified Bex-Nikaidoh operation. Video available at: https://www.jtcvs.org/article/S2666-2507(24)00227-X/fulltext.