

Abstract
Background:
Estimating the prevalence of food insecurity among vulnerable sub-groups, especially pregnant women, is significant. This study aimed to estimate the pooled prevalence of food insecurity among Iranian pregnant women and to determine its related factors.
Materials and Methods:
This study constitutes a systematic review and meta-analysis of cross-sectional studies involving pregnant women, published between January 2000 and September 2022, in English and Persian on seven databases. Finally, 14 studies were analyzed and synthesized, with the results presented in the form of forest plots. Heterogeneity was investigated using the I2 index and the meta-regression to evaluate variables suspected of causing heterogeneity. Statistical analysis and synthesis were performed using Stata-16.
Results:
The pooled prevalence of food insecurity among Iranian pregnant women was 45% (95% confidence interval: 37–54%). In a multi-variable meta-regression model, p values were significant for the year of data collection and the type of the questionnaire. The adjusted I2 and R2 indices were estimated at 84.47 and 51.46%, respectively. The prevalence of food insecurity among Iranian pregnant women has been estimated at half a million.
Conclusions:
Given the high prevalence of food insecurity among pregnant women in Iran, we propose the inclusion of food insecurity screening for this vulnerable demographic within the primary healthcare package. Additionally, we advocate for the allocation of food subsidies to pregnant women confronting food insecurity.
Keywords: Food insecurity, food security, Iran, meta-analysis, pregnant women, prevalence, systematic review
Introduction
Food insecurity is a condition in which people lack adequate physical, socio-cultural, political, and economic access to food to meet their nutritional needs to have a healthy life. The lack of accessible and economical food can have adverse effects on physical, social, emotional, and cognitive developments of individuals throughout life.[1] The mild type of food insecurity includes concerns or uncertainties about the availability as well as poor quality of food. On the other side, the moderate type of food insecurity includes reduced food quantity and failure to meet standard food needs. In the severe category of food insecurity, in addition to the aforementioned condition, individuals experience an entire day of hunger due to insufficient funds to purchase food.[2] According to the report released by the Food and Agriculture Organization (FAO) (2021), the global moderate and severe types of food insecurity increased from 21.2 to 29.3% between 2014 and 2021, which reached 30.4% in 2020. In addition, in 2021, about 29.3% of the global population experienced the severe type of food insecurity, being about 350 million more than the rate in 2019.[2] The food insecurity prevalence in 2018 among Iranian pregnant women in Tehran, Qazvin, and Ilam provinces was reported to be 34.2, 43.9, and 34.3%, respectively.[3,4,5]
Adequate nutrition is vital for pregnant women. Consequently, pregnant women with a normal body weight require an increased intake of vitamins, minerals, and an additional 300 kcal per day to ensure their health and support proper fetal growth compared to non-pregnant individuals.[6] During pregnancy, women undergo a variety of physiological, behavioral, and psycho-social changes that may be affected by limited access to adequate food. Food insecurity is an important risk factor that can affect a pregnant woman’s physical health, being associated with negative consequences, such as an increased risk of at least one of the pregnancy complications, including preeclampsia, hyperlipidemia, hypertension, overweight, and diabetes.[7] In addition, it is associated with congenital defects and adverse fetal health consequences, such as a cleft palate, tetralogy of Fallot, a reduction in exclusive breast-feeding, and infant mortality.[1,8] Furthermore, difficulties in providing food may lead to stressful events in the family, thereby endangering the mother’s mental health as well as causing anxiety and depression.[7] In the general population, several factors play roles in food insecurity, including household income, ethnicity, age, and educational level. Globally, the gender gap in the prevalence of moderate and severe types of food insecurity increased in 2021, having been 4.3% higher in women than in men; besides, it increased by 1.3% com-pared to the rate in 2020.[2] Most pregnant women living in low-income countries and regions are facing food insecurity due to the increased nutritional needs, inadequate access to food, lack of dietary diversity, and additional costs of prenatal care and future necessities for the baby.[1]
Some studies have confirmed the effect of maternal food insecurity on the health of infants and children.[9,10] The results of a systematic review (2020) showed that the prevalence of food insecurity in households with pregnant women and infants ranged from 5.2 to 87%.[8] In a systematic review and meta-analysis published in 2016, the prevalence of food insecurity among Iranian households, mothers, and children was reported to be 49, 61, and 67%, respectively, which had a rising trend from 2004 to 2015.[11] Iran has confronted declining birth rates and an aging population in recent years. In response, the government has instituted policies aimed at bolstering the population and encouraging childbirth by discontinuing free family planning services and infertility treatment. In recent years, several articles have reported on the prevalence of food insecurity among pregnant women in various cities and provinces of Iran.[12,13] Thus, the present study was designed and conducted to estimate the pooled prevalence of Food Insecurity among Iranian Pregnant Women (FIPW) and its associated factors.
Materials and Methods
This study was conducted based on the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) protocol.[14] The protocol of this study was registered at PROSPERO under code CRD42021278388.
Cross-sectional studies reporting the prevalence of FIPW between January 1, 2000 and September 30, 2022, in English or Persian, were searched. The search was conducted on the international databases of Medline, Web of Science, Scopus, Embase, and ISC, and the Persian databases of Magiran, SID, Researchgate, WHO, Cabdirect, Go.gale, Medrxiv, and Semanticscholar were searched for gray literatures. To this end, two researchers (AE and IM) searched the abovementioned databases independently using pre-determined keywords, their combinations, and their Persian equivalents. The keywords included prevalence, food security, food insecurity, pregnancy, postpartum, preterm labor, gestation*, Iran*, and pregnant women. The search strategy based on the PECO framework was determined as follows: Prevalence (O) of food insecurity © among Iranian pregnant women (P) compared to non-pregnant women or total women of reproductive age or the general population of Iran, other countries, or globally ©. The search strategy was changed according to the guidelines of each database. After removing duplicate articles, two researchers (AE and RF) screened the titles and abstracts of articles independently based on the inclusion and exclusion criteria. The inclusion criteria were cross-sectional studies on pregnant women at any gestational age with an average age of 18–45 years and those measuring the prevalence of food insecurity based on the standard questionnaires of USDA-18, HFIAS-9, and Radimer-Cornell-16. On the other side, the exclusion criterion was failure to report prevalence information. After removing irrelevant studies, the two researchers studied the full text of the articles and screened them based on the inclusion and exclusion criteria. At every stage, disagreements were resolved through discussion or based on the judgment of the third researcher (IM).
Data were extracted by two researchers (AM and RF) independently from the studies, which were entered into an Excel datasheet. Disagreements between the researchers were resolved through discussion and the judgment of the third researcher (IM). The extracted information included general information on the first author, year of publication, and year of the study. In addition, methodological information on the sampling method, sample size, number of participants, type of questionnaires, and inclusion and exclusion criteria was extracted. The characteristics of the study population included the city or province of the study, urban or rural population of the study, number of people with food insecurity, number of people with food insecurity at different levels (mild, moderate, and severe), average age, gestational age, response rate, occupational status (housewives/employees), wanted or unwanted pregnancy, family size, pregnancy rank, average Body Mass Index (BMI), educational level, and Perceived Economic Status (PES) (low, medium, and high). In addition, the Annual Inflation Rate (AIR) and the average Annual Food Expenditure per Person (AFEP) were extracted in US dollar from the website of the Central Bank of the Islamic Republic of Iran in the investigated province. Moreover, the Crude Birth Rate (CBR) was extracted for every 105 individuals from the website of the National Organization for Civil Registration. Having considered $835 as the cut-off point for AFEP, the records were divided into two categories, and the pooled prevalence of food insecurity was calculated.[15,16,17] As the time period for measuring food insecurity in the Radimer-Cornell-16 questionnaire, like that in the USDA-18 questionnaire, is 1 year, the studies were categorized in one group for analysis. The quality of the studies was assessed by two researchers (AM and BM) independently using the Joanna Briggs Institute (JBI) Critical Appraisal tools for use in the JBI systematic reviews checklist for prevalence studies. In case of any disagreements after the discussion, the judgment of the third researcher (IM) prevailed.
To calculate the pooled prevalence, synthesis, random effect models, the 95% confidence interval (95% CI), and the metaprop command in Stata were used. In addition, to better estimate the standard error and confidence intervals of the records, the pooled prevalence was calculated using the Freeman–Tukey double-arcsine transformation command. The records were weighted by sample size. Furthermore, heterogeneity among the studies was assessed using I2 and the Galbraith plot. Values equaling 50% or higher than I2 (0 ≤ I2 ≤ 100) were considered statistically heterogeneous. In the meta-analysis of prevalence studies, the assessment of the publication bias was not logical because the purpose of prevalence studies is not to investigate the relationship between the variables of exposure and outcome. In addition, neither the authors’ willingness to report the results nor the editors’ willingness to accept and publish the article was affected by the results. In all statistical analyses, p < 0.05 was considered statistically significant, and all statistical analyses were performed using Stata 16 (Stata Corp, College Station, TX, USA). To conduct the univariate meta-regression, the variables of the year of data collection, mean age, AFEP, and questionnaire type were entered into the model separately, with the parameters re-estimated by the finite maximum likelihood method. The multi-variable meta-regression was conducted for those variables with a p value less than 0.2. Finally, year of data collection and the type of the questionnaire as independent variables were entered in the multi-variable meta-regression to investigate heterogeneity.
Ethical considerations
Researchers tried to act in an unbiased way to analyze the retrieved data of articles. The Ethics Committee of Lorestan University of Medical Sciences approved this study (Project code: IR.LUMS.REC.1400.247).
Results
Figure 1 presents a detailed account of the literature search process and article selection. Out of a total of 225 records retrieved from diverse sources, following screening and the removal of duplicates and unrelated records according to the exclusion criteria, 14 records published between 2014 and 2018 have been included in this review. The characteristics of the studies included are presented in Table 1. The statistical population of the records included women referring to community health centers. Cluster sampling was performed for all records. The average response rate in the records was 96.75% (80.52–100), and the mean age of the participants in the records was 28.45 (26.5–30.15). In 76.70% of the records, the educational level of the pregnant women had been reported, yet their rankings were not the same. A total of 86% of the records reported the employment status of pregnant women, of whom 85% were housewives. Only 50% of the records reported PES, based on which 31% of the pregnant women surveyed were in low-income households, 49% were in middle-income households, and 20% were in high-income households. A total of 64% of the records indicated that the pregnant women were either urban or rural, based on which 99% of the pregnant women were urban. However, the family size was not mentioned in 93% of the records. In addition, only 21% of the records reported the mean and standard deviation of the BMI. In all records, 64.30% reported whether pregnancies were wanted or unwanted, with a variation range between 13.20 and 50% of unwanted pregnancies.[3,18] In total, 64% of the records mentioned the pregnancy rank, 44% of which having been first pregnancies. In 50% of the records, participants entered the study between 2.5 and 9 months of gestation, 85% entered the study between 6 and 7 months of gestation, and 35% entered the study from delivery to 8 months after it, yet in 15% of the studies, the time had not been reported. In 85% of the records, the exclusion criterion was a history of chronic diseases in pregnant women. However, the rest of the studies did not mention any exclusion criteria. The mean range of quality scores of the records was 80% (56–100), 57% of which having been of a high quality and 43% having been of a low quality. In addition, comparison of the prevalence of FIPW and the quality of the records showed no regular pattern. Heterogeneity of studies was assessed using Galbraith plot [Figure 2]. The total number of the participants in the records was 8939, of whom 3741 suffered from food insecurity. The pooled prevalence of FIPW was estimated at 45% (95% CI: 37–54%). The frequency of Iranian pregnant women with food insecurity has been estimated at half a million. Out of the 14 records, eight studies (57%) reported FIPW by level, 64% reported mild food insecurity, 24% reported moderate food insecurity, and 12% reported severe food insecurity. Among the records, 50% used the HFIAS-9 questionnaire, 42% used the USDA-18 questionnaire, and one study used the Radimer-Cornell-16 questionnaire to measure FIPW. Figure 3 shows the pooled prevalence of FIPW by the type of the questionnaire, AFEP, and climatic zones.
Figure 1.

PRISMA flow diagram for food insecurity in Iranian pregnant women
Table 1.
Characteristics of the included studies
| Author | Year of study | Location | Participants | FI* (N) | Questionnaire | Perceived economic status (%) | Critical Appraisal | ||
|---|---|---|---|---|---|---|---|---|---|
|
| |||||||||
| Low | Moderate | High | |||||||
| Alikamali et al.[12] | 2018 | Zarand | 400 | 313 | USDA-18 | 21.75 | 65.25 | 13.00 | 100% |
| Dolatian et al.[3] | 2016 | Ilam | 674 | 231 | HFIAS-9 | NR** | NR | NR | 100% |
| Ezzeddin et al.[4] | 2014 | Tehran | 325 | 111 | USDA-18 | 22.80 | 63.69 | 12.92 | 89% |
| Fathi Beyranvand et al.[19] | 2017 | Khorramabad | 148 | 64 | Radimer-Cornell-16 | NR | NR | NR | 100% |
| Hojaji et al.[20] | 2015 | Tehran | 700 | 244 | USDA-18 | 33.29 | 34.43 | 32.29 | 78% |
| Karbin et al.[21] | 2017 | Khorasan Razavi | 2481 | 821 | HFIAS-9 | NR | NR | NR | 89% |
| Kazemi et al.[13] | 2018 | Hamadan | 684 | 521 | USDA-18 | NR | NR | NR | 67% |
| Kazemi et al.[22] | 2017 | Qazvin | 394 | 173 | HFIAS-9 | 49.24 | 42.89 | 7.87 | 56% |
| Khoshgoo et al.[23] | 2017 | Qom | 394 | 187 | USDA-18 | NR | NR | NR | 67% |
| Moafi et al.[5] | 2017 | Qazvin | 394 | 173 | HFIAS-9 | 49.24 | 42.89 | 7.87 | 67% |
| Rajizadeh et al.[24] | 2015 | Yazd | 351 | 191 | HFIAS-9 | 33.05 | 32.76 | 32.76 | 89% |
| Rasty et al.[18] | 2015 | Falavarjan | 400 | 176 | USDA-18 | NR | NR | NR | 67% |
| Hoseini et al.[25] | 2016 | Qazvin | 860 | 278 | HFIAS-9 | 7.44 | 60.00 | 32.56 | 100% |
| Sharifi et al.[26] | 2016 | Ilam | 734 | 258 | HFIAS-9 | NR | NR | NR | 56% |
*Food Insecurity, **Not Reported
Figure 2.
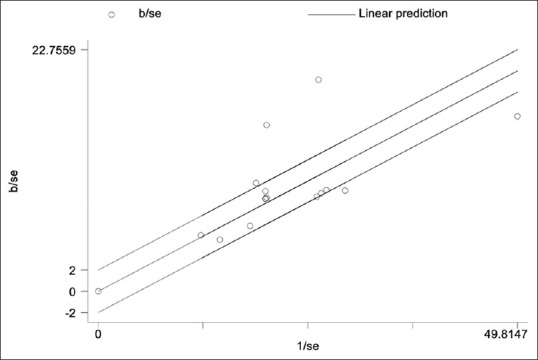
Galbraith plot for assessing heterogeneity
Figure 3.

Forest plots of pooled estimate prevalence of Iranian pregnant women food insecurity based on (a) the used questionnaires, (b) average annual food expenditure per person (AFEP) US$, and (c) the climatic regions
The pooled prevalence of food insecurity in the studies having used the USDA-18 questionnaire to collect the data was higher than that in the studies having used the HFIAS-9 questionnaire (52 and 39%, respectively). However, the difference was not statistically significant.
The pooled prevalence of FIPW in studies with AFEP <$835 was higher than the pooled prevalence of food insecurity in other studies (54 and 37%, respectively), but the difference was not statistically significant. In addition, the prevalence of food insecurity in studies with AFEP <$835 showed a larger distribution than that in other studies. Besides, the pooled prevalence of FIPW varied according to climatic regions, including mountainous, semi-desert, and desert regions, having been 47, 38, and 59%, respectively; however, the difference was not statistically significant. Among the records, four studies examined the statistical difference of the FIPW prevalence based on PES, with the difference having been significant in two studies[20,24] and insignificant in two other studies.[5,22] Only one study reported a statistically significant difference in the prevalence of food insecurity based on the educational level.[5] However, none of the records examined the statistical difference among FIPW based on the age, wanted or unwanted pregnancy, pregnancy rank, and occupational status (housewives/employees). Since these variables were not reported in the records, it was possible neither to estimate the pooled prevalence of FIPW nor to analyze the sub-groups based on them.
In the multi-variable meta-regression model, p values were significant for the year of data collection and the type of the questionnaire (p < 0.05). According to the meta-regression results, the adjusted I2 and R2 indices were estimated at 84.47 and 51.46%, respectively [Table 2]. Figure 4 shows the meta-regression by the type of the questionnaire and the year of data collection. In addition, Figure 5a shows that the FIPW trend followed the AIR trend from 2015 to 2018. On the other side, Figure 5b shows that as the FIPW trend increased from 2014 to 2018, CBR experienced a decreasing trend.
Table 2.
Meta-regression for determining heterogeneity
| Final model | β coefficient | SE* | p | Heterogeneity I2% | Adj.R2%** |
|---|---|---|---|---|---|
| Year | 0.08 | 0.03 | 0.015 | 84.47 | 51.46 |
| Questionnaire | -0.13 | 0.06 | 0.047 | ||
| Constant | -151.31 | 52.69 | 0.015 |
*SE: Standard Error; **Adj.R2: Adjusted R squared
Figure 4.

Meta-regression graph: (a) the used questionnaire type and (b) the year of data collection
Figure 5.

(a) Comparison of the food insecurity trend in pregnant women with the inflation rate during years 2014–2018; (b) Comparison of the food insecurity trend in pregnant women with crude rate of birth in 105 persons in Iran during the years 2014-2018. The dotted line is the best fit line (regression line)
Discussion
The present study aimed to estimate the pooled prevalence of FIPW and also to determine the factors associated with it. To this end, the pooled prevalence of FIPW was estimated at 45%. The results of the meta-regression showed that the variables of the year of data collection and the type of the questionnaire significantly explained heterogeneity of the prevalence in the records by 51.46%.
The mean FIPW rate for mild, moderate, and severe levels of food insecurity were 64, 24, and 12%, respectively. In a systematic review and meta-analysis (2014), food insecurity levels in Iranian households were 58, 30, and 12%, respectively.[9] Therefore, it can be argued that Iranian households with pregnant women (2014–2018) and all Iranian households (1991–2011) experienced relatively similar levels of food insecurity. However, Iranian women do not seem to consider food security as the main criterion for trying to get pregnant. The prevalence of unwanted pregnancies in a systematic review and meta-analysis among Iranian pregnant women during the time period of 2012–2018 (26%, 95% CI: 23–28) reinforced this hypothesis.[27] The high rate of the pooled prevalence of FIPW (45%) can be a factor associated with the reduction in planned pregnancies in Iran.
Given the disparities in classifications or the absence of statistical difference testing concerning variables such as residence (urban/rural), age group, family size, planned or unplanned pregnancies, pregnancy order, birth order, employment status (housewives/employees), BMI, and educational level of pregnant women grappling with food insecurity in the records, we were unable to ascertain the factors associated with FIPW. Nonetheless, the results from a systematic review and meta-analysis conducted in 2020 indicate a statistically significant variance in food insecurity among pregnant women based on their BMI and educational attainment.[28] In essence, higher educational levels appear to correlate with enhanced socio-economic status and reduced food insecurity. Limited studies have been undertaken on the rural pregnant population, making it advisable to conduct additional investigations within this demographic. Despite conflicting results concerning statistical disparities among FIPW based on the economic status of households in the records, the findings of a systematic review and meta-analysis from 2014 indicate a statistically significant divergence in food insecurity predicated on the economic well-being of Iranian households.[29] Various studies have employed three approaches to evaluate participant economic status, including direct income inquiries, inquiries regarding welfare provisions, and inquiries into purchasing Power Equivalent Scores (PESs). The first two approaches have demonstrated lesser validity due to the potential for erroneous information and the constraints involved in categorizing individuals into high-income, middle-income, and low-income groups. Inquiries into PES appear to offer greater validity and reliability when measuring economic status due to their independence from the time of the study and economic pressures stemming from inflation. As such, we recommend employing PES inquiries in future studies to assess participant economic status and examine its correlation with food insecurity.
The difference in the estimated pooled prevalence, according to the type of the questionnaire, can be related to their different content, time of the study, and study population. Based on the content analysis, the researchers believe that the different questionnaires used have the same content for measuring food insecurity. Comparison of the FIPW trend from 2015 to 2018 with the AIR trend in this time period showed that the changes in these two variables followed the same pattern [Figure 5a].
When the US unilaterally withdrew from the Joint Comprehensive Plan Of Action (JCPOA) in 2018 and economic sanctions were reinstated, the Iranian market suffered severe inflation, and food prices rose.[30] It seems that the increased inflation rate and the decreased purchasing power of households reduced households’ access to food, so FIPW increased.
The high distribution of prevalence rates (33–78%) in studies with AFEP <$835 could be due to different eating habits or inadequate budgeting for providing foods. Inadequate financial resources have reduced the variety of foods available, which may result in reducing or eliminating some meals, thereby increasing the risk of food insecurity. Living in different climatic zones can affect the prevalence of food insecurity due to different levels of people’s access to local food, lower prices of some foods at the place of production, and costs of transporting food products from one place to another.
Our study is not without limitations. Although some sources of heterogeneity were identified, a significant portion of them remained unknown. The limited quality of some records may constrain the generalizability of our findings. In light of the inconsistency in classifying certain variables, such as types of FIPW, educational levels, and age, or the absence of reported statistical correlation tests in some records, it has proven challenging to pinpoint the factors associated with FIPW. However, our study benefits from strengths such as sub-group analysis, meta-regression, and the extraction of AIR, AFEP, and CBR data from reliable sources to analyze FIPW based on these parameters.
Conclusion
Given the substantial prevalence of FIPW in Iran, it appears imperative to reconsider population growth policies and the discontinuation of free family planning services. Given the concurrent rise in the prevalence of FIPW and the AIR between 2014 and 2018, it seems that food insecurity among women of childbearing age constitutes one of the contributing factors to the shortcomings of pregnancy incentive programs. Therefore, it is recommended that screening for FIPW and women of the childbearing age be added to the primary healthcare package and that food subsidies be allocated to pregnant women with food insecurity.
Financial support and sponsorship
Lorestan University of Medical Sciences
Conflicts of interest
Nothing to declare.
Acknowledgements
This study was the result of research project No. 1397-1-99-2379 approved by Lorestan University of Medical Sciences.
References
- 1.Iqbal S, Ali I. Maternal food insecurity in low-income countries: Revisiting its causes and consequences for maternal and neonatal health. J Agric Food Res. 2021;3:100091. [Google Scholar]
- 2.IFAD, UNICEF, WFP, WHO. The State of Food Security and Nutrition in the World 2022. Repurposing food and agricultural policies to make healthy diets more affordable. FAO Rome, Italy: 2022. [Google Scholar]
- 3.Dolatian M, Sharifi N, Mahmoodi Z. Relationship of socioeconomic status, psychosocial factors, and food insecurity with preterm labor: A longitudinal study. Int J Reprod Biomed. 2018;16:563–70. [PMC free article] [PubMed] [Google Scholar]
- 4.Ezzeddin N, Jahanihashemi H, Zavoshy R, Noroozi M. The prevalence of postpartum depression and its association with food insecurity among mothers referring to community health centers. Iran J Psychiatry. 2018;13:280–7. [PMC free article] [PubMed] [Google Scholar]
- 5.Moafi F, Kazemi F, Samiei Siboni F, Alimoradi Z. The relationship between food security and quality of life among pregnant women. BMC Pregnancy Childbirth. 2018;18:319. doi: 10.1186/s12884-018-1947-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Lokhande TN, Varma KS, Gharate SM, Mahajan SK, Surana KR. Vitamins as nutraceuticals for pregnancy. Vitamins as Nutraceuticals: Recent Advances and Applications. Wiley Online Library. 2023:185–204. [Google Scholar]
- 7.Ivers LC, Cullen KA. Food insecurity: Special considerations for women. Am J Clin Nutr. 2011;94:1740S–4S. doi: 10.3945/ajcn.111.012617. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Augusto ALP, AV de Abreu Rodrigues, Domingos TB, Salles-Costa R. Household food insecurity associated with gestacional and neonatal outcomes: A systematic review. BMC Pregnancy Childbirth. 2020;20:1–11. doi: 10.1186/s12884-020-02917-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Mohammadi Nasrabadi F, Omidvar N, Khoshfetrat M, Kolahdooz F. Household food insecurity in the Islamic Republic of Iran: A systematic review and meta-analysis. East Mediterr Health J. 2014;20:698–706. [PubMed] [Google Scholar]
- 10.Pedroso J, Buccini G, Venancio SI, Pérez-Escamilla R, Gubert MB. Maternal mental health modifies the association of food insecurity and early child development. Matern Child Nutr. 2020;16:e12997. doi: 10.1111/mcn.12997. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Behzadifar M, Behzadifar M, Abdi S, Malekzadeh R, Salmani MA, Ghoreishinia G, et al. Prevalence of food insecurity in Iran: A systematic review and meta-analysis. Arch Iran Med. 2016;19:288–94. [PubMed] [Google Scholar]
- 12.Alikamali M, Khodabandeh S, Motesaddi M, Bagheri Z, Esmaeili MA. The Association between demographic characteristics and attempting of pregnancy with postpartum depression and anxiety among women referring to community health centres: A Cross sectional study. Malays J Med Sci. 2020;27:93–104. doi: 10.21315/mjms2020.27.3.10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Kazemi F, Masoumi SZ, Shayan A, Yasaghi SZS. Prevalence of food insecurity in pregnant women and its association with gestational weight gain pattern, neonatal birth weight, and pregnancy complications in Hamadan County, Iran, in 2018. Agric Food Secur. 2020;9:1–8. [Google Scholar]
- 14.Panic N, Leoncini E, de Belvis G, Ricciardi W, Boccia S. Evaluation of the endorsement of the preferred reporting items for systematic reviews and meta-analysis (PRISMA) statement on the quality of published systematic review and meta-analyses. PLoS One. 2013;8:e83138. doi: 10.1371/journal.pone.0083138. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.The Central Bank of Iran. Household Budget Survey In Urban Areas in Iran. [Last accessed on 2023 Jan 16]. Available from:https://www.cbi.ir/simplelist/1421.aspx .
- 16.The Central Bank of Iran. Foreign Exchange Rates. [Last accessed on 2023 Jan 16]. Available from:https://www.cbi.ir/ExRates/rates_en.aspx .
- 17.National Organization for Civil Registration of Iran. Crude Birth Rate of Iran. [Last accessed on 2023 Jan 16]. Available from:https://www.sabteahval.ir .
- 18.Rasty R, Pouraram H, Heshmat R. Food insecurity and some demographic and socioeconomic characteristics, fertility, and pregnancy in women with planned and unplanned pregnancy. Iran J Epidemiol. 2015;11:34–42. [Google Scholar]
- 19.Fathi Beyranvand H, Eghtesadi S, Ataie-Jafari A, Movahedi A. Prevalence of food insecurity in pregnant women in khorramabad city and its association with general health and other factors. Iran J Nutr Sci Food Technol. 2019;14:21–30. [Google Scholar]
- 20.Hojaji E, Zavoshy R, Noroozi M, Jahanihashemi H. Assessment of household food security and its relationship with some pregnancy complications. J Mazandaran Univ Med Sci. 2015;25:87–98. [Google Scholar]
- 21.Karbin K, Khorramrouz F, Farkhani EM, Sobhani SR, Mosalmanzadeh N, Shahriari Z, et al. Household food insecurity during pregnancy as a predictor of anthropometric indices failures in infants aged less than 6 months:a retrospective longitudinal study. Public Health Nutrition. 2022;25:1005–12. doi: 10.1017/S1368980021003591. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Kazemi F, Moafi F, Samiei Siboni F, Alimoradi Z. Prevalence and predictors of food insecurity among pregnant women: A cross sectional study in Qazvin Province, Iran. Midwifery. 2018;66:25–9. doi: 10.1016/j.midw.2018.07.013. [DOI] [PubMed] [Google Scholar]
- 23.Khoshgoo M, Eslami O, Al-Hosseini MK, Shidfar F. The relationship between household food insecurity and depressive symptoms among pregnant women: A cross sectional study. Iran J Psychiatry. 2020;15:126–33. [PMC free article] [PubMed] [Google Scholar]
- 24.Rajizadeh A, Tavakoli M, Hajipour M, Rabiey-Faradonbeh M, Salehi-Abargouei A, Bonab AM, et al. Food security status of pregnant women in Yazd, Iran, 2014-2015. J Nutr Food Secur. 2019;4:152–60. [Google Scholar]
- 25.Hoseini KS, Kazemi F, Alimoradi Z, Oskoei SSS, Alijani H, Zolghadr S. Association between household food security and pregnancy complications. Soc Health Behav. 2018;1:26–30. [Google Scholar]
- 26.Sharifi N, Dolatian M, Mahmoodi Z, Mohammadi-Nasrabadi F, Mehrabi Y. The relationship between structural social determinants of health and food insecurity among pregnant women. Iran Red Crescent Med J. 2018;20:1–8. (In Press) [Google Scholar]
- 27.Sayehmiri K, Ebtekar F, Zarei M, Gheshlagh RG. Prevalence of unwanted pregnancy among Iranian women: An updated meta-analysis. BMC Pregnancy Childbirth. 2019;19:1–7. doi: 10.1186/s12884-019-2640-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Demétrio F, Teles CAS, Santos DBD, Pereira M. Food insecurity in pregnant women is associated with social determinants and nutritional outcomes: A systematic review and meta-analysis. Cien Saude Colet. 2020;25:2663–76. doi: 10.1590/1413-81232020257.24202018. [DOI] [PubMed] [Google Scholar]
- 29.Alimoradi Z, Kazemi F, Estaki T, Mirmiran P. Household food security in Iran: Systematic review of Iranian articles. Adv Nurs Midwifery. 2015;24:63–76. [Google Scholar]
- 30.Hejazi J, Emamgholipour S. The effects of the re-imposition of US sanctions on food security in Iran. Int J Health Policy Manag. 2022;11:651–7. doi: 10.34172/ijhpm.2020.207. [DOI] [PMC free article] [PubMed] [Google Scholar]