

Abstract
Background
The 2022 African Cup of Nations (AFCON) took place in Cameroon from January 9th to February 5th, 2022, including Garoua in the north. We aimed to measure the impact of this event on the local COVID-19 epidemic given the implementation of a preventive strategy based on a health pass.
Methods
All players, staff and fans involved in the AFCON event were screened with PCR tests. Symptomatic cases were also continuously monitored in the general population and screened for variants of concern. Daily numbers of confirmed cases were compared to neighboring countries numbers retrieved from a public domain source.
Results
In total, 1479 and 2481 tests were performed in the general population and on asymptomatic AFCON attendees, respectively. From the latter, 12.5% were PCR-positive; 97% were infected with Omicron, with no significant difference compared to the passive program (G-test, P value = 0.162). Surveillance indicated the AFCON did not increase the number of symptomatic PCR-positive cases in the general population compared to neighboring countries.
Conclusions
Though the COVID-19 epidemic was fueled by asymptomatic cases infected with the Omicron variant at the time, the non-therapeutic preventive measures implemented for AFCON mitigated an increase in the epidemic in the local population.
Keywords: COVID-19, outdoor event, transmission
Introduction
The 2022 African Cup of Nations (AFCON) soccer event took place in Cameroon from January 9th to February 5th, 2022, in the midst of the COVID-19 pandemic. This 4-week outdoor mass event gathered tens of thousands of people from the entire continent at the time when the SARS-CoV-2 Omicron variant emerged. The contest was held in five cities in Cameroon, including Garoua, an urban area with 360 000 inhabitants in the north of the country. The stadium in Garoua has a capacity of 25 000 seats.
Mass gathering events have been identified as high-risk venues for SARS-CoV-2 transmission, with evidence of transmission from asymptomatic carriers1 by airborne droplets.2 Thus, in an effort to limit local social and economic consequences, most events were banned at an early stage of the pandemic to prevent the spread of SARS-COV-2. Over time, comprehensive and efficient prevention strategies were progressively implemented for outdoor3 and indoor events, such as the use of antigen-detecting rapid diagnostic tests, the compulsory wearing of medical masks, social distancing and optimized ventilation.4,5
During the pandemic, the containment prevention policy to prevent the spread of COVID-19 in Cameroon was based on international travel restrictions (entry restrictions and testing), hand hygiene, social distancing, quarantine and treatment of confirmed cases; a lockdown was not implemented in the country. As part of the national strategy to control the COVID-19 epidemic, symptomatic cases in the general population were tested by RT-PCR in accordance with the World Health Organization (WHO) guidelines.6
The city of Garoua, a regional capital of Cameroon situated close to the border with Nigeria, was the only city in the north of the country to host AFCON matches that posed a risk of multiple gatherings. The Public Health Emergency Operations Center (COUPS) approved and implemented guidelines from the Ministry of Health that involved strict non-therapeutic measures addressed to the local population and visitors. These measures included mandatory mask wearing, social distancing and containment and isolation measures for infected persons. In addition, thanks to the country’s last 2 years of experience during the COVID-19 pandemic, a well-functioning system for surveillance and response during this mass-gathering was implemented before the AFCON competition began.
The present study aims to describe the impact of the AFCON event on the local COVID-19 epidemic in the context of the implementation of a preventive strategy that included a health pass.
Materials and methods
Settings and participants
The ‘Centre Pasteur du Cameroun annexe de Garoua’ (CPCAG) is the reference laboratory for molecular diagnosis of viral infections in northern Cameroon. This virology laboratory has been involved in the diagnosis of COVID-19 since the beginning of the pandemic in March 2020. As part of the national strategy to control the COVID-19 epidemic, symptomatic cases in the general population were tested by RT-PCR. RT-PCR testing was routinely performed for diagnosis and follow-up of COVID-19 among individuals with symptoms of COVID-19 or influenza in the general population and for all travelers to the country. We report here the data on the RT-PCR results from November 2021 to March 2022; this period included the AFCON event hosted by Cameroon from January 9th to February 5th, 2022, including five matches in the city of Garoua.
Prevention protocol
The prevention measures were implemented by the COUPS: for the entire population of Cameroon, mandatory mask wearing and, in case of a positive test, isolation for at least 7 days and until a negative test; for all travelers arriving and departing at airports and border crossings, a negative test within <72 hr; access to the stadium and fan zones during the AFCON was subject to the presentation of a health pass by both competing teams and spectators. All staff, players and spectators had to undergo either a rapid detection test (RDT) or a PCR test. For fully vaccinated people, the health pass has a validity of 1 week. Unvaccinated participants had to systematically present a negative diagnostic test performed within the previous 24 hr. RT-PCR tests were mandatory for all players, officials, ball boys and referees; an antigen test was sufficient for individuals in the bleachers and fan zones. Individuals who received a positive test were requested to self-quarantine for a period of 7 days. The health passes were managed in a secure digital centralized national web application set up by the Ministry of Health that recorded each individual’s tests and vaccination doses. The health pass strategy was not applicable to members of the local population who did not attend AFCON. Hand-washing facilities with hydroalcoholic gel were scattered in and around the stadium/fan zones.
Data from neighboring countries
To assess the impact of the AFCON contest on SARS-CoV-2 transmission, it is necessary to compare the passive testing figures to an unrelated control setting. As no specific data are available for cities in Cameroon that did not host the AFCON contest, we used data from neighboring countries as a proxy. We extracted data on the numbers of confirmed cases from the public domain using the WHO website (https://covid19.who.int/data). Gabon and Nigeria were the only neighboring countries for which sufficient data are available, i.e. the number of cases reported at least two time points per week and >10 000 new cases during the study period.
SARS-CoV-2 diagnostics
RNA was extracted from nasal swab specimens (QIAamp Viral RNA Mini Kit; Qiagen), and COVID-19 diagnosis was performed at CPCAG using a validated RT-PCR assay (Sansure Biotech) provided by the COVID-19 National Coordination Organization headed by the Cameroon Ministry of Health on an ABI QuantStudio™ 7 Flex system real-time PCR system (Thermofisher Scientific). Tests with Ct values for the target genes below or equal to 36 were considered positive.
Variant screening
PCR-positive specimens with Ct values below 30 were selected for further variant of concern screening. Variant detection and characterization were performed using the SNPsig® SARS-CoV-2 assay (EscapePLEX, NOVACYT PrimerDesign Ltd, UK) following the manufacturer’s instructions. This assay enables simultaneous discriminatory identification of four clinically significant mutations (E484K, K417N, K417T and P681R), together with confirmation of a SARS-CoV-2 positive sample. The combination of these four mutations allows detection and discrimination of the Alpha, Beta, Gamma, Delta and Omicron variants of SARS-CoV-2.
Data analysis
Data analysis was performed using the Tidyverse package of R language.7 G-tests were used to examine the significance of the differences in the proportion of variants between the passive routine screening program for the general population and travelers and the active screening program for the AFCON. Plots of the weekly number of cases were created using non-parametric local polynomial regression Locally Estimated Scatterplot Smoothing (LOESS).
Results
Based on the national strategy for COVID-19 epidemic control, symptomatic cases in the general population and all travelers were subjected to RT-PCR testing. Of the 1479 tests performed in Garoua city during this passive screening program from 1 November 2021 to 31 March 2022, 1231 were from symptomatic persons, and 266 (18%) were positive. The median age of the suspected cases was 38 years old (Table 1). The testing period reported in this study encompasses the 2 months preceding and the 2 months after the AFCON competition to capture the evolution of the dynamics of the epidemic in Cameroon.
Table 1.
Number of PCR tests, positivity rate and characteristics of individuals involved in the passive testing program in Garoua city from 1 November 2021 to 31 March 2022, and active AFCON testing program at Garoua from January 3rd to February 1, 2022
| Passive testing | AFCON testing | |
|---|---|---|
| Number of tests | 1479 | 2481 |
| Symptomatic | 1231 | 0 |
| Asymptomatic | 248 | 2481 |
| Positive tests | ||
| Number | 266 | 309 |
| % | 18 | 12.5 |
| Median age (y) | 38 | 34.5 |
| Gender ratio (H/F) | 1.1 | 2.8 |
During the time period of the active AFCON screening program for individuals who were required to take a PCR test to obtain a health pass (i.e. players, journalists, officials and all spectators), 12.5% (n = 309) of 2481 tests performed were PCR-positive. All of the tested individuals were asymptomatic. The median age of the positive cases was 34.5 years old, significantly lower than the median age of the positive cases in the passive screening program (Wilcoxon test P value = 0.006). A week before the beginning of the AFCON contest, the active screening program detected a positivity rate of 26%, which decreased to 12% in the first week, then stayed below 1% for the next 3 weeks until the end of the AFCON (Fig. 1).
Fig. 1.
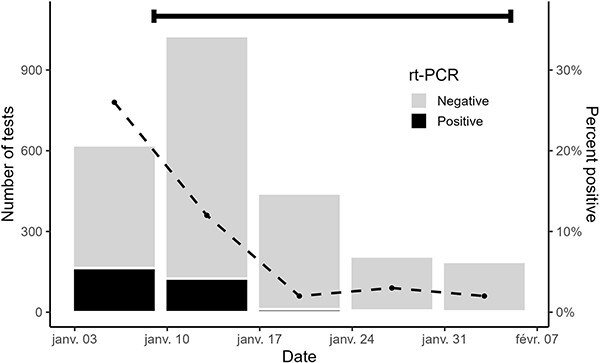
Number of RT-PCR tests conducted per week during the active AFCON screening program from January 3 to February 1, 2022. The black bar represents the number of positive RT-PCR tests (left axis). The dashed line represents the proportion of positive tests (right axis). The black horizontal bar indicates the time period of the AFCON.
The number of symptomatic cases increased during the last quarter of 2021 due to the emergence of the Omicron variant.8 The positivity rate for the passive testing program among the local population of Garoua was 58% in early January 2022, at the time the active testing for the AFCON began. Both the positivity rate and number of cases in the passive testing program steadily declined during the period of the contest; the rate of positivity was 28% in Week 1, 6% in Week 2 and remained at 0% until the AFCON ended. The number of PCR-positive cases was 64 in the week before the contest, 15 in the first week, three in the second week, three in the third week, zero in the last 2 weeks of the contest and zero during the 3 weeks after AFCON ended (Fig. 2). Indeed, by the end of February, the baseline number of cases and the positivity rate returned to the same levels as prior to the event (Fig. 2) and remained low until the end of our study period in March 2022.
Fig. 2.
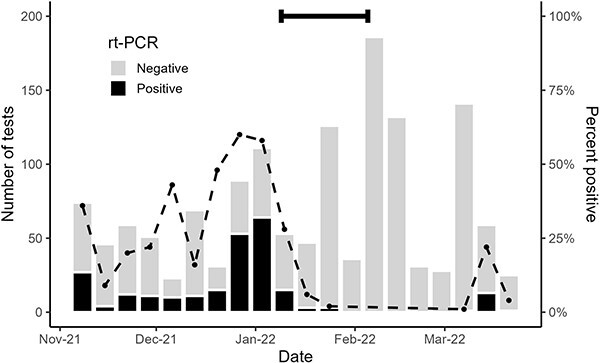
Number of RT-PCR tests per week in the passive testing program for the general population of Garoua from 1 November 2021 to 31 March 2022. Bars show the number of RT-PCR tests (left axis): black sections represent the number of positive tests and gray sections represent the number of negative tests. The dashed line shows the proportion of positive tests (right axis). The black horizontal bar indicates the time period of the AFCON.
Omicron was the predominant variant in both the passive testing program among the general population of Garoua and the active AFCON testing program. Real-time PCR showed 86% of the strains detected during the period of the AFCON belonged to the Omicron variant, similarly to other areas in the world (1). Further whole genome sequencing revealed that the uncalled variants in RT-PCR were all Omicron, exclusively clade 21K (data not shown). Thus, Omicron has been the main variant circulating in Garoua since December 2021, similarly to the rest of Cameroon and the African continent.9 During the period that active screening was conducted, Omicron represented 97% of SARS-CoV-2 strains detected in the passive and active screening programs. Furthermore, there was no significant difference in the proportions of variants detected by the passive and active screening programs (G-test, P value = 0.162; Supplementary Table 1).
Datasets on the daily numbers of confirmed cases of COVID-19 from neighboring countries were retrieved from the public domain source of the WHO website.10 Of the seven countries neighboring Cameroon, we only selected the countries that published data at least twice per week and reported at least 10 000 new cases over the period of interest for this study (November 2021 to March 2022), namely, Gabon and Nigeria. The locally weighted running line smoother to the fit for the point-by-point weekly numbers of cases was plotted using LOESS method (Fig. 3). The data used to plot this graph are listed in Supplementary Table 2. The maximum peak number of cases of COVID-19 in Garoua was observed in the week of January 3, 1 week ahead of the contest. The maximum peak number of cases was observed during the week of December 20 in Nigeria and the week of December 27 in Gabon. The interval between the peak maxima of the three settings either reflects a true difference in the spread of the pandemic or is due to differential delays in the data reporting process. Taking these maxima as reference points, the number of cases in Garoua, Nigeria and Gabon had fallen to 23%, 55% and 73%, respectively, 1 week later; to 5%, 39% and 41% 2 weeks later; to 5%, 23% and 36% 3 weeks later (the week of the last AFCON match in Garoua); to 0%, 11% and 18% 4 weeks later; and to 0%, 8% and 20% 5 weeks later, after the AFCON had ended. Overall, the decline in the number of cases was similar between the three geographical contexts.
Fig. 3.
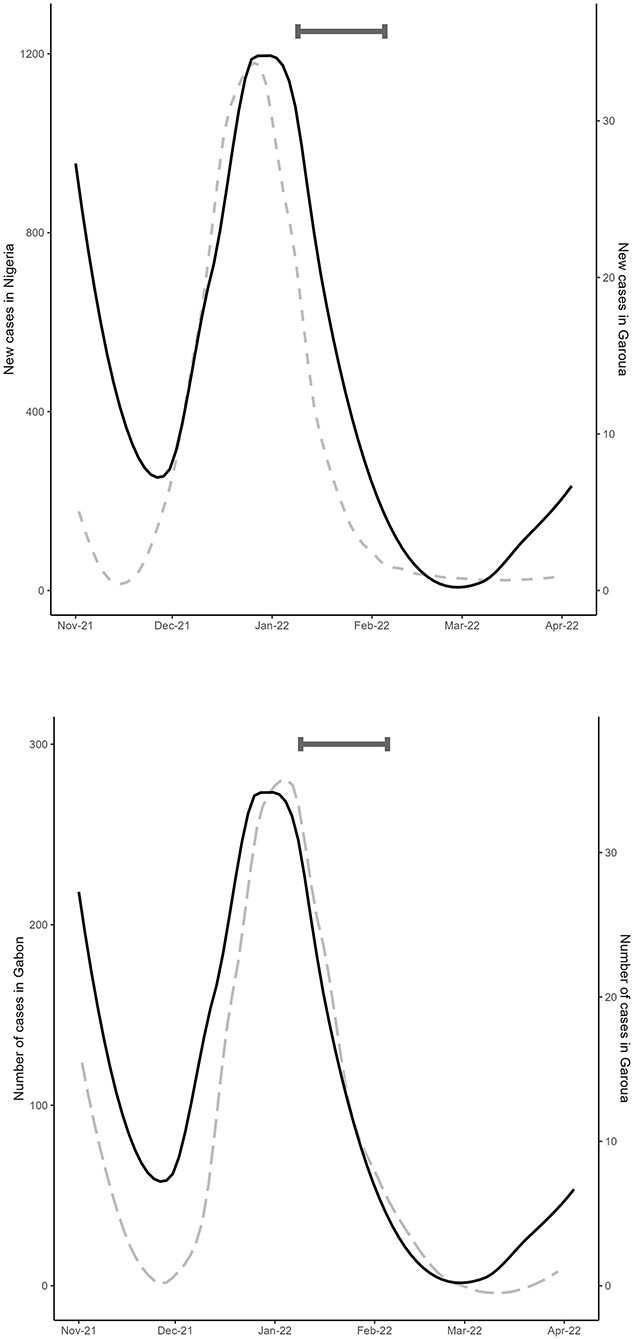
Locally estimated scatterplot smoothing of the number of cases of COVID-19 reported in Garoua (solid line, right axis) and the neighboring countries (long dash line, left axis) Nigeria (a) and Gabon (b). The black horizontal bar indicates the time period of the AFCON.
Discussion
The AFCON contest in Cameroon attracted tens of thousands of visitors. AFCON was held in the midst of the COVID-19 pandemic and represented a major public health challenge, especially as the event occurred when the SARS-CoV-2 Omicron variant was emerging. The city of Garoua hosted five matches in the 4-week contest. A variety of non-therapeutic measures were employed to mitigate the transmission of the virus: a health pass was required to access the stadium, consisting of a negative SARS-CoV-2 test, either RDT or RT-PCR, within <24 hr, or within 1 week if vaccinated. Quarantine was mandatory for all individuals who obtained a positive COVID-19 test.
Main findings of this study
The active screening program that was established for the health pass system detected a positivity rate of 12.5% based on PCR tests of AFCON visitors and attendees. This rate certainly reflects a proxy for the attack rate in the general population of Garoua city during January and February 2022, considering the entire population was at risk of infection. However, none of the 309 individuals who tested positive in the active screening program had any symptoms, and none of the individuals who tested negative reported any symptoms. Asymptomatic PCR-positive cases constitute a reservoir for the silent transmission of COVID-19 within the local population.11 However, the number of positive tests steadily decreased during the period of the contest, both among visitors and in the local population. Indeed, the weekly proportions of PCR-positive tests were 58% and 26% among visitors and the local population, respectively, before the first match, and these rates dropped continuously during the following four weeks. The incubation time of Omicron, the circulating variant at that time (Supplementary Fig. 1 and Supplementary Table 1), is 3.6 days, and 90% of symptoms appear within 7 days after infection.12 Thus, the follow-up period of this study would have detected any putative rise in cases in the local population due to the AFCON. Therefore, we conclude that the exogeneous inflow of individuals with COVID-19 associated with the AFCON did not trigger an increase in the number of PCR-positive cases in the local population.
As there is a lack of data from inside Cameroon as a comparison for these figures as denominators, we used data derived from sources in the public domain. Sufficient data were available for two neighboring countries, Nigeria and Gabon, to perform a robust comparison. While the peak maximal numbers of cases were observed on different dates in each of the three regions, the numbers of cases declined in a similar manner in all three countries, to 0% in Garoua, 8% in Nigeria and 20% in Gabon after the end of the event. These data strongly suggest that the AFCON contest did not significantly increase the number of symptomatic cases of COVID-19 in the general population of Garoua either during AFCON or in the subsequent seven weeks compared to neighboring countries with no such mass gathering events.
What is already known on this topic
Due to the mode of transmission of SARS-CoV-2 virus through airborne droplets,2 mass gathering events have been identified as high-risk venues. While the risk of SARS-CoV-2 transmission for indoor events has been documented,4,5,13,14 data for outdoor events are scarce.3,15,16 As the pandemic progresses, preventive measures, such as Ag-RDT screening, mask-wearing, social distancing, vaccination and optimized ventilation4,5 were progressively implemented for outdoor3 and indoor events. However, despite their effectiveness, these measures do not completely suppress SARS-CoV-2 transmission.15
What this study adds
Overall, this study indicates that the non-therapeutic measures implemented for the AFCON, including a health pass supported by a digital app and mandatory regular diagnostic testing, successfully mitigated the risk of enhanced SARS-CoV-2 transmission in Garoua. Thus, the AFCON event did not affect the dynamic of the epidemic in this region in terms of the number of cases or the circulating variants.
Limitations
From this study, it is difficult to deconvolve the relative importance of non-therapeutic measures, protective immunity from a previous infection and vaccination with the observed epidemic trends. By the end of 2021, Cameroun had reported a cumulative total of 109 666 confirmed cases in a population of over 27.2 million. This figure is certainly underestimated, as testing among the general population was based on a passive process. The national vaccination rate at the end of 2021 was 3% for at least one dose, which is inferior to the vaccination rates of 6.5% and 16.5% for the neighboring countries of Nigeria and Gabon, respectively.17 Thus, the low levels of acquired immunity among the population of Cameroon were far from sufficient to prevent a surge in the epidemic, given the low rate of cross-neutralization against Omicron, the predominant variant circulating at that time, which frequently reinfected individuals with a previous history of COVID-19 worldwide.18–20
In conclusion, despite the fact that the epidemic was fueled by asymptomatic cases infected with the Omicron variant ahead of the event and the AFCON attracted hundreds of PCR-positive individuals, the event did not result in an increase in the number of symptomatic or asymptomatic PCR-positive COVID-19 cases in the Garoua region as adequate preventive measures were implemented.
Supplementary Material
Acknowledgements
We would like to thank Christelle Yonta Tilong (Msc) and Ornelle Domdem Tchoua (Msc) for performing the molecular analyses in the laboratory during the pandemic, as well the local public health officials, in particular Dr Zakary Yaou (Regional Delegation for Health) and Dr Yaya Mohamodou (MD Coordinator, Regional Delegation for Health) for on-site management, case identification and data collection.
Jean-Luc Berland, Research Associate
Hermann Njifon, Research Associate
Emilie Westeel, Research Associate
Henri Moumbeket, PhD Student
Florence Komurian-Pradel, Research Associate, Head of GABRIEL Research Network
Pauliana Ilouga, Master’s Student
Richard Njouom, Head of Virology Department
Ronald Perraut, Research Director
Contributor Information
Jean-Luc Berland, Scientific and Medical Department, Fondation Merieux, 69002 Lyon, France.
Hermann Njifon, Centre Pasteur du Cameroun, Annexe de Garoua, Garoua, Cameroon.
Emilie Westeel, Scientific and Medical Department, Fondation Merieux, 69002 Lyon, France.
Henri Moumbeket, Centre Pasteur du Cameroun, Yaounde, Cameroon.
Florence Komurian-Pradel, Scientific and Medical Department, Fondation Merieux, 69002 Lyon, France.
Pauliana Ilouga, Centre Pasteur du Cameroun, Yaounde, Cameroon.
Richard Njouom, Centre Pasteur du Cameroun, Yaounde, Cameroon.
Ronald Perraut, Centre Pasteur du Cameroun, Annexe de Garoua, Garoua, Cameroon.
Conflict of interest
The authors declare that they have no conflict of interest.
Data availability
The submitted article includes all data generated during this study. The datasets on the numbers of confirmed cases in Cameroon neighboring countries were derived from the public domain using the WHO website (https://covid19.who.int/data).
References
- 1. Wilmes P, Zimmer J, Schulz J. et al. SARS-CoV-2 transmission risk from asymptomatic carriers: results from a mass screening programme in Luxembourg. Lancet Reg Health Eur 2021;4:100056. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Zhang R, Li Y, Zhang AL. et al. Identifying airborne transmission as the dominant route for the spread of COVID-19. Proc Natl Acad Sci U S A 2020;117(26):14857–63. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. De Polo A, Pais Dei Mori L, Mongillo M. et al. Halting the pandemic outside “CORTINA2021” alpine world ski championships: a challenge for sport and public health in times of COVID-19. J Public Health (Oxf) 2022;44(2):e203–10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Delaugerre C, Foissac F, Abdoul H. et al. Prevention of SARS-CoV-2 transmission during a large, live, indoor gathering (SPRING): a non-inferiority, randomised, controlled trial. Lancet Infect Dis 2022;22(3):341–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Revollo B, Blanco I, Soler P. et al. Same-day SARS-CoV-2 antigen test screening in an indoor mass-gathering live music event: a randomised controlled trial. Lancet Infect Dis 2021;21(10):1365–72. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Public health for mass gatherings: key considerations Published online. 2015; Accessed March 22, 2023. https://www.who.int/publications-detail-redirect/public-health-for-mass-gatherings-key-considerations
- 7. Wickham H, Averick M, Bryan J. et al. Welcome to the Tidyverse. J Open Source Softw 2019;4(43):1686. [Google Scholar]
- 8. Vaughan A. Omicron emerges. New Sci 2021;252(3363):7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Elbe S, Buckland-Merrett G. Data, disease and diplomacy: GISAID’s innovative contribution to global health. Glob Chall 2017;1(1):33–46. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. WHO coronavirus (COVID-19) dashboard data. Accessed July 12, 2023. https://covid19.who.int/data
- 11. Rothe C, Schunk M, Sothmann P. et al. Transmission of 2019-nCoV infection from an asymptomatic contact in Germany. N Engl J Med 2020;382(10):970–1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Wu Y, Kang L, Guo Z. et al. Incubation period of COVID-19 caused by unique SARS-CoV-2 strains: a systematic review and meta-analysis. JAMA Netw Open 2022;5(8):e2228008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Koizumi N, Siddique AB, Andalibi A. Assessment of SARS-CoV-2 transmission among attendees of live concert events in Japan using contact-tracing data. J Travel Med 2020;27(5):taaa096. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Sugano N, Ando W, Fukushima W. Cluster of severe acute respiratory syndrome coronavirus 2 infections linked to music clubs in Osaka, Japan. J Infect Dis 2020;222:1635–40. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Suñer C, Coma E, Ouchi D. et al. Association between two mass-gathering outdoor events and incidence of SARS-CoV-2 infections during the fifth wave of COVID-19 in north-east Spain: a population-based control-matched analysis. Lancet Reg Health Eur 2022;15:100337. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Drakesmith M, Hobson G, John G. et al. Developing a population data science approach to assess increased risk of COVID-19 associated with attending large events. Int J Popul Data Sci 6(3):1711. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Mathieu E, Ritchie H, Ortiz-Ospina E. et al. A global database of COVID-19 vaccinations. Nat Hum Behav 2021;5(7):947–53. [DOI] [PubMed] [Google Scholar]
- 18. Reynolds CJ, Pade C, Gibbons JM. et al. Immune boosting by B.1.1.529 (Omicron) depends on previous SARS-CoV-2 exposure. Science 2022;377(6603):eabq1841. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Zou J, Xia H, Xie X. et al. Neutralization against omicron SARS-CoV-2 from previous non-Omicron infection. Nat Commun 2022;13(1):852. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Lavezzo E, Pacenti M, Manuto L. et al. Neutralising reactivity against SARS-CoV-2 Delta and omicron variants by vaccination and infection history. Genome Med 2022;14(1):61. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
The submitted article includes all data generated during this study. The datasets on the numbers of confirmed cases in Cameroon neighboring countries were derived from the public domain using the WHO website (https://covid19.who.int/data).