

Abstract
Congenital absence of the internal carotid artery is a rare anatomical variant. The primarily reported origins of the ophthalmic artery associated with this variant are the posterior communicating, middle cerebral, and external carotid arteries. We report the case of a patient without an internal carotid artery whose ophthalmic artery originated from the contralateral internal carotid artery. The superior hypophyseal and prechiasmal arteries may contribute to collateral flow to the orbit from the contralateral internal carotid artery.
Keywords: Anomalous origin of ophthalmic artery, Internal carotid artery agenesis, Circuminfundibular anastomosis, Superior hypophyseal artery, Prechiasmal artery
Introduction
Absence of the internal carotid artery (ICA) is rare. According to Vasović et al. [1], hypoplasia, aplasia, and agenesis of the ICA were reported in 466 cases by the end of 2020, with a prevalence of 0.1%. The diagnosis of ICA agenesis is based on collateral flow patterns to the cerebral hemisphere ipsilateral to the absent ICA and the absence of the carotid canal. Some studies have investigated the origin of the ophthalmic artery (OphA). The main sites of origin of the OphA associated with the absence of the ICA are the ipsilateral posterior communicating artery (PCoA) [2,3], ipsilateral middle cerebral artery (MCA) [4], and external carotid artery [5]. However, to the best of our knowledge, cases of OphA originating from the contralateral ICA are extremely rare in the English literature. Herein, we report a case of OphA originating from the contralateral ICA associated with ipsilateral ICA agenesis.
Case presentation
A 45-year-old woman presenting with headache and facial pain underwent magnetic resonance angiography, showing the absence of flow-related signal intensity within the right ICA.
The right MCA received a collateral flow from the right PCoA, in which multiple fusiform dilations and aneurysms were observed (Fig. 1). The A1 segment of the right anterior cerebral artery (ACA) was absent, and the right ACA received collateral flow from the left ICA through the anterior communicating artery (Fig. 1). The right OphA originated from the supraclinoid segment of the left ICA, followed by the inferior aspect of the optic chiasm, and entered the right optic canal (Fig. 2). The bone-window computed tomography image showed total absence of the right carotid canal (Fig. 3). Cerebral angiography was performed to assess for the presence of multiple cerebral aneurysms. Three-dimensional digital subtraction angiography of the left ICA revealed that the right OphA originated from the medial aspect of the left ICA, slightly proximal to the left OphA (Fig. 4). In addition, the right OphA passed through the ventral side of the pituitary stalk, from which 2 small vessels toward the pituitary stalk and the right optic tract branched off (Fig. 5).
Fig. 1.

Frontal maximum intensity projection of the magnetic resonance angiography demonstrates total absence of flow in the right internal carotid artery. The collateral flows to the right middle cerebral artery via the right posterior communicating artery (arrow) and to the right anterior cerebral artery via the anterior communicating artery (arrowhead).
Fig. 2.

Axial slab maximum intensity projection image from the magnetic resonance angiography demonstrates the right ophthalmic artery originating from the left internal carotid artery, running ventral to the pituitary stalk, and reaching the right optic canal (arrowheads). The normally originated left ophthalmic artery is also visible (arrow).
Fig. 3.

The bone-window computed tomography image shows total absence of the right carotid canal. The left carotid canal is visible (arrow).
Fig. 4.

Anterior-posterior image from 3-dimensional digital subtraction angiography demonstrates the right ophthalmic artery (arrowheads) originating from the left internal carotid artery just proximal to the left ophthalmic artery (arrow).
Fig. 5.

(A, B) Axial slab maximum intensity projection images of 3-dimensional digital angiography show 2 small branches (white straight arrows) from the right ophthalmic artery (white curved arrow) running toward the pituitary and the optic tract. Pituitary gland (black arrow) and stalk (black arrowhead) are seen posterior to these branches.
Discussion
In the present case, the right OphA originated from the left ICA in the absence of the right ICA. The absence of the ICA is believed to be caused by abnormal regression of the first and third aortic arches in the developing embryo [6,7]. It is thought that a variety of collateral blood flows develop in combination with the timing of the formation of the circle of Willis and basilar arteries [8,9]. Lie classified the absence of the ICA into 6 categories based on collateral blood flow pathways to the cerebral hemisphere, and this case was classified as type A. In acquired ICA occlusion, a bony carotid canal is formed; however, the ipsilateral carotid canal is not observed during ICA agenesis. This characteristic pattern of collateral vessels and carotid canal defects led to the diagnosis of unilateral ICA agenesis.
The OphA has various anomalous origins. The most common variant is the middle meningeal artery origin, followed by the cavernous segment origin of the ICA [10]. The main reported sites of origin of the OphA associated with the absence of the ICA are the ipsilateral PCoA [2,3], ipsilateral MCA [4], and external carotid artery [5].
To date, only 3 cases of OphA originating from the contralateral ICA following absence of the ICA have been reported [[11], [12], [13]]. In these case reports, the path of anomalous OphA has not been discussed in detail. The embryological explanation for this abnormal ophthalmic arterial origin remains speculative; however, circuminfundibular anastomoses formed mainly by the bilateral superior hypophyseal arteries (SHAs) may be involved. The SHA is a branch of the supraclinoid ICA. The SHA originates medially or posteromedially to the ICA and within 5 mm of the origin of the OphA [14]. This artery runs toward the origin of the pituitary stalk and divides into several branches that supply the optic nerve, optic chiasm, anterior gland of the pituitary, pituitary stalk, and third ventricle [15].
The branches that terminate at the proximal portion of the stalk connect with the branches of the contralateral SHA, forming the main part of the circuminfundibular anastomosis anterior to the infundibulum [14]. The circuminfundibular anastomosis has two other main components: the infundibular arteries from the PCoA and the prechiasmal arteries from the OphA [16].
In this case, a right anomalous OphA originating from the medial aspect of the left ICA, slightly proximal to the left OphA and small branches running toward the pituitary stalk and optic tract were discovered. It is possible that the left SHA was anastomosed with the right prechiasmal artery via the right SHA to supply the right orbit (Fig. 6). Prechiasmal arteries are rare, with only one (1.7%) identified in 30 autopsy specimens in 1 report [17] and 3 in 25 autopsy specimens (6%) identified in another report [15]. The infrequent occurrence of the prechiasmal artery and the absence of the ICA may be related to the fact that the OphA originating from the contralateral ICA is very rare.
Fig. 6.
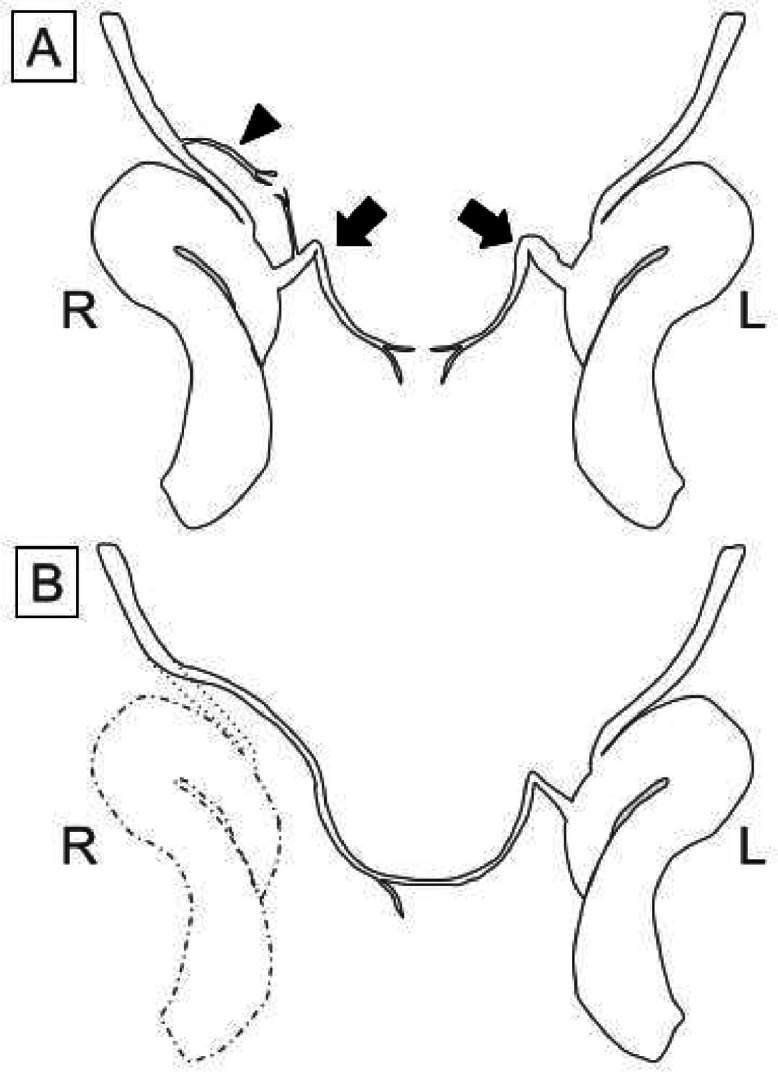
Schematic drawing of the superior hypophyseal arteries (SHAs) (arrows), the prechiasmal artery (arrowhead) from the right ophthalmic artery, and the internal carotid arteries, viewed from below (A). In this case (B), the anastomoses between the left SHA and the right prechiasmal artery via the right SHA may enable the right orbit to be supplied by the contralateral internal carotid artery.
Conclusion
We encountered an extremely rare case in which the OphA originated from the contralateral ICA and was associated with agenesis of the ICA. The circuminfundibular anastomosis formed by the bilateral SHA, prechiasmal artery, and infundibular artery may be involved in the formation of a collateral pathway between the orbit and contralateral ICA. To avoid ischemic complications during endovascular embolization and surgery of the sella turcica, radiologists should be aware of the possibility of this collateral pathway and report it to the surgeon.
Patient consent
In this case report, written informed consent was obtained.
Footnotes
Competing Interests: The authors have no conflicts of interest.
Acknowledgments: This study was funded by Toranomon Hospital and the University of Tokyo to cover expenses for English editing and article submission, respectively.
References
- 1.Vasović L, Mrkaić A. Congenital unilateral absence of the internal carotid artery associated with aneurysms of different arteries: a review. World Neurosurg. 2022;164:393–412. doi: 10.1016/j.wneu.2022.05.141. [DOI] [PubMed] [Google Scholar]
- 2.Kunishio K, Yamamoto Y, Sunami N, Asari S. Agenesis of the left internal carotid artery, common carotid artery, and main trunk of the external carotid artery associated with multiple cerebral aneurysms. Surg Neurol. 1987;27:177–181. doi: 10.1016/0090-3019(87)90292-8. [DOI] [PubMed] [Google Scholar]
- 3.Naeini RM, De J, Satow T, Benndorf G. Unilateral agenesis of internal carotid artery with ophthalmic artery arising from posterior communicating artery. AJR Am J Roentgenol. 2005;184:571–573. doi: 10.2214/ajr.184.2.01840571. [DOI] [PubMed] [Google Scholar]
- 4.Teal JS, Naheedy MH, Hasso AN. Total agenesis of the internal carotid artery. AJNR Am J Neuroradiol. 1980;1:435–442. [Google Scholar]
- 5.Amano T, Inamura T, Matsukado K, Yoshikai S, Yuhi F, Nagata S. Ruptured saccular aneurysm of a dolichoectatic internal carotid artery in a patient with agenesis of the contralateral internal carotid artery: case report. Neurol Med Chir. 2004;44:20–23. doi: 10.2176/nmc.44.20. [DOI] [PubMed] [Google Scholar]
- 6.Huber G. Intracranial carotid anastomosis and partial aplasia of an internal carotid artery. Neuroradiology. 1980;20:207–212. doi: 10.1007/BF00336685. [DOI] [PubMed] [Google Scholar]
- 7.Savastano S, Feltrin GP, Chiesura-Corona M, Miotta D. Cerebral ischemia due to congenital malformations of brachiocephalic arteries: case reports. Angiology. 1992;43:76–83. doi: 10.1177/000331979204300110. [DOI] [PubMed] [Google Scholar]
- 8.Li S, Hooda K, Gupta N, Kumar Y. Internal carotid artery agenesis: a case report and review of literature. Neuroradiol J. 2017;30:186–191. doi: 10.1177/1971400917692162. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Given CA, Huang-Hellinger F, Baker MD, Chepuri NB, Morris PP. Congenital absence of the internal carotid artery: case reports and review of the collateral circulation. AJNR Am J Neuroradiol. 2001;22:1953–1959. [PMC free article] [PubMed] [Google Scholar]
- 10.Toma N. Anatomy of the ophthalmic artery: Embryological consideration. Neurol Med Chir. 2016;56:585–591. doi: 10.2176/nmc.ra.2015-0324. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Zhou W-Z, Zhao L-B, Liu S, Shi H-B. Teaching NeuroImages: unilateral agenesis of internal carotid artery with ophthalmic artery from opposite side. Neurology. 2015;84:e65–e66. doi: 10.1212/WNL.0000000000001317. [DOI] [PubMed] [Google Scholar]
- 12.Ogul H, Havan N, Gedikli Y, Pirimoglu B, Kantarci M. A new anatomic variation: coexistence of both Dandy-Walker variant and ophthalmic artery originating from contralateral internal carotid artery. J Craniofac Surg. 2016;27:e336–e338. doi: 10.1097/SCS.0000000000002482. [DOI] [PubMed] [Google Scholar]
- 13.Zink WE, Komotar RJ, Meyers PM. Internal carotid aplasia/hypoplasia and intracranial saccular aneurysms: series of three new cases and systematic review of the literature. J Neuroimaging. 2007;17:141–147. doi: 10.1111/j.1552-6569.2007.00092.x. [DOI] [PubMed] [Google Scholar]
- 14.Krisht AF, Barrow DL, Barnett DW, Bonner GD, Shengalaia G. The microsurgical anatomy of the superior hypophyseal artery. Neurosurgery. 1994;35:899–903. doi: 10.1227/00006123-199411000-00014. discussion 903. [DOI] [PubMed] [Google Scholar]
- 15.Gibo H, Lenkey C, Rhoton AL., Jr. Microsurgical anatomy of the supraclinoid portion of the internal carotid artery. J Neurosurg. 1981;55:560–574. doi: 10.3171/jns.1981.55.4.0560. [DOI] [PubMed] [Google Scholar]
- 16.Dawson BH. The blood vessels of the human optic chiasma and their relation to those of the hypophysis and hypothalamus. Brain. 1958;81:207–217. doi: 10.1093/brain/81.2.207. [DOI] [PubMed] [Google Scholar]
- 17.Truong HQ, Najera E, Zanabria-Ortiz R, Celtikci E, Sun X, Borghei-Razavi H, et al. Surgical anatomy of the superior hypophyseal artery and its relevance for endoscopic endonasal surgery. J Neurosurg. 2018;131:154–162. doi: 10.3171/2018.2.JNS172959. [DOI] [PubMed] [Google Scholar]