
Figure 2.
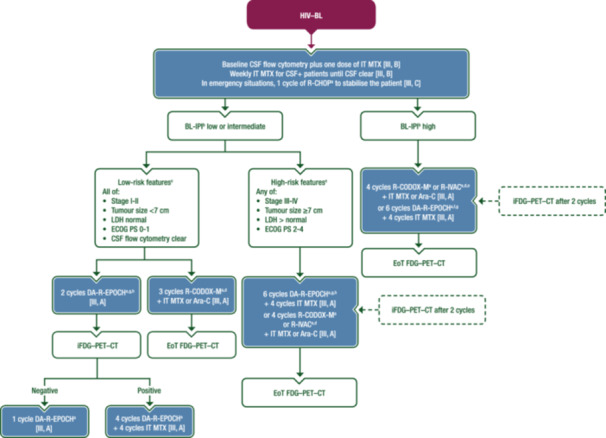
First‐line management of HIV–BL. Purple: algorithm title; blue: systemic anticancer therapy or their combination; white: other aspects of management and non‐treatment aspects; dashed lines: optional therapy. Ara‐C, cytarabine; BL, Burkitt lymphoma; CALGB, Cancer and Leukemia Group B; CNS, central nervous system; CSF, cerebrospinal fluid; CSF+, cerebrospinal fluid positive; CT, computed tomography; DA‐R‐EPOCH, dose‐adjusted rituximab–etoposide–prednisone–vincristine–cyclophosphamide–doxorubicin; ECOG, Eastern Cooperative Oncology Group; EMA, European Medicines Agency; EoT, end of treatment; FDA, Food and Drug Administration; FDG, [18F]2‐fluoro‐2‐deoxy‐D‐glucose; GMALL‐B‐ALL, German Multicentre Study Group for Adult Acute Lymphoblastic Leukaemia B‐cell acute lymphoblastic leukaemia; HIV–BL, human immunodeficiency virus‐associated Burkitt lymphoma; i, interim; IPI, International Prognostic Index; IT, intrathecal; LDH, lactate dehydrogenase; LMB, lymphomes malins B; MTX, methotrexate; PET, positron emission tomography; PS, performance status; R‐CHOP, rituximab–cyclophosphamide–doxorubicin–vincristine–prednisone; R‐CODOX‐M, rituximab–cyclophosphamide–vincristine–doxorubicin–methotrexate; R‐IVAC, rituximab–ifosfamide–etoposide–cytarabine; ULN, upper limit of normal. aRituximab is not EMA or FDA‐approved for the treatment of BL. bBL‐IPI factors are age ≥40 years, ECOG PS 2‐4, LDH >3 × ULN and CNS involvement, as per Olszewski et al. 29 cRisk definition as per Roschewski et al. 36 dOr equivalent regimens. Rituximab‐containing regimens such as LMB, GMALL‐B‐ALL and CALGB protocols are valid alternatives to R‐CODOX‐M or R‐IVAC. eR‐CODOX‐M or R‐IVAC (or equivalent regimens) are preferred for patients with high‐risk BL‐IPI and for those with CNS disease at diagnosis. fDA‐R‐EPOCH is an alternative for less fit patients or those aged >60 years. gConsider R‐CHOP plus immunotherapies for elderly and/or unfit patients with the aim of escalating if fitness improves. hDA‐R‐EPOCH may be preferred for patients with low‐ or intermediate‐risk BL‐IPI, especially those aged >60 years.