

Abstract
Background:
Angular deformities of the lower extremities are common in children and are a frequent reason for orthopaedic referral. These deformities, which are usually encountered when children start to walk are typically measured using the tibiofemoral angle (TFA), which represents the angle formed by the intersection of the anatomical axis of the femur with the anatomical axis of the tibia.
Objectives:
This study aimed to determine the TFA in healthy South-Eastern Nigerian children, and to determine the effect of gender and age on this angle.
Materials and Methods:
This cross-sectional study was done in Enugu metropolis with 3147 school children and adolescents aged 3–17 years.
Results:
It was found that the majority of the subjects (97.6%) had valgus TFA. The maximum knee valgus angle from the study was 6.8° ± 0.80° at 4 years. Thereafter, the knee valgus angle declined to a mean of 2° at 17 years.
Conclusion:
There were physiological changes in TFAs noted, which vary with regards to both age and gender of the subject.
Keywords: Goniometer, tibio-femoral angle, valgus
Introduction
Angular deformities of the lower extremities are common in children and are a frequent reason for orthopaedic referral.[1] These deformities, which are usually encountered when children start to walk are usually of great concern to parents of the children.[2] The tibiofemoral angle (TFA) represents the angle formed by the intersection of the anatomical axis of the femur with the anatomical axis of the tibia.[3] This angle may also be expressed indirectly as the intercondylar distance or the intermalleolar distance.[3] It is commonly used to determine the angular deformities of the knee, and this alignment is subjected to the effects of genetic factors, intrauterine posturing, nutritional status, ligamentous laxity, and the anatomical peculiarities of the femur and tibia, which both change with age and weight bearing.[4]
It can be measured using radiographic, photographic, and clinical methods; however, the clinical method is widely used because it is non-invasive, easy to perform, reliable, and reproducible.[3]
Many studies have shown that TFA undergoes physiologic changes in healthy growing children and adolescents; as during normal development, the knees undergo sequential physiologic limb alignment changes from varus to valgus.[5] However, angular deformities may also develop due to pathologies at the epiphysis, physis, or metaphysis, and this may then lead to abnormal joint loading, which if left uncorrected predisposes to degenerative knee joint disease.[5]
Knowledge of the normal changes in TFA with growth is very important not only in differentiating physiologic from pathologic lower extremity conditions but also in allaying the anxiety in the parents. However, despite all the literature on limb alignment, misinterpretations of physiologic varus and valgus deformities of the knee persist, often leading to unnecessary therapeutic interventions, which are not only unwarranted but may prove harmful.[6]
Th study aims to determine the TFA in healthy Southeast Nigerian children.
Materials and Methods
The study area was Enugu metropolis, which serves as the capital of Enugu State in Southeastern Nigeria, and is made up of three local government areas; Enugu East, Enugu North, and Enugu South.
It was a cross-sectional descriptive study (using a simple random sampling method) conducted in 14 nursery, primary, and secondary schools from April 2020 to March 2021, involving the measurement of TFA, as well as obtaining the bio data of all patients.
Inclusion criteria
The inclusion criteria are as follows:
children between the ages of 3 and 17 years.
Exclusion criteria
The exclusion criteria are as follows:
those with obvious musculoskeletal disorders affecting the lower limbs (such as skeletal dysplasia, cerebral palsy, neuromuscular disorder, and foot deformities;
those with windswept deformity of the knee;
those who have lower limb length inequality; and
those who had undergone surgery on the lower limbs.
Sample size
The sample size was calculated using the formula:  where Z is the value for the selected alpha level of 0.05 = 1.96, σ is the standard deviation of the outcome variable from previous study[14] = 1.4, and e is the acceptable margin of error =0.05.
where Z is the value for the selected alpha level of 0.05 = 1.96, σ is the standard deviation of the outcome variable from previous study[14] = 1.4, and e is the acceptable margin of error =0.05.
The minimum sample size for the study was 3011.81. This was rounded up to 3147.
Procedure
TFA was measured using the clinical method described by Matthew and Madhuri.[7] Each subject was made to stand with the hips and knee in full extension and neutral rotation, with the ankles or knees touching each other. The anterior superior iliac spine (ASIS) was marked with a skin marker. The centre of the patella was identified and marked with a marker. The centre of the ankle, the midpoint between the medial and lateral malleoli identified with the aid of Vernier calliper was marked. A standard goniometer with adjustable arms was placed with the hinge at the centre of the patella. Each arm of the goniometer was adjusted such that the tip of the proximal arm touched the ASIS and the tip of the distal arm touched the midpoint of the ankle. TFA is measured to the nearest degree. A valgus TFA was expressed in a positive degree and a varus TFA in a negative degree. TFA was measured in both limbs. Skin marks made with the hypoallergenic marker were then cleaned with baby wipes.
Data analysis
The data collected was analysed using the IBM Statistical Package for Social Sciences, IBM SPSS version 20 (Armonk, NY: IBM Corp). A P value of less than 0.05 was considered statistically significant.
Results
A total of 3147 schoolchildren and adolescents aged 3–17 years participated in this study. Table 1 shows the age distribution of the subjects.
Table 1.
Age distribution of the subjects
| Age (years) | N | % |
|---|---|---|
| 3 | 215 | 6.8 |
| 4 | 213 | 6.8 |
| 5 | 178 | 5.7 |
| 6 | 210 | 6.7 |
| 7 | 214 | 6.8 |
| 8 | 210 | 6.7 |
| 9 | 210 | 6.7 |
| 10 | 210 | 6.7 |
| 11 | 212 | 6.7 |
| 12 | 212 | 6.7 |
| 13 | 215 | 6.8 |
| 14 | 216 | 6.9 |
| 15 | 216 | 6.9 |
| 16 | 213 | 6.8 |
| 17 | 203 | 6.5 |
| Total | 3147 | 100.0 |
In Table 1, a total number of 3147 subjects were studied; the age with the lowest number of subjects was to 5 years.
From Figure 1, there were 1577 (50.1%) males and 1570 (49.9%) females that participated in the study.
Figure 1.
Gender distribution of the subjects
From Table 2, most of the subjects (97.6%) had valgus TFA, whereas only 2.4% had varus TFA. The distribution was statistically significant (P = 0.000).
Table 2.
Distribution of varus and valgus TFA amongst the subjects
| Subjects | Subjects with valgus TFA | Subjects with varus TFA |
|---|---|---|
| n (%) | n (%) | |
| Male | 1537 (48.8) | 40 (1.3) |
| Female | 1536 (48.8) | 34 (1.1) |
| Total | 3073 (97.6) | 74 (2.4) |
P value = 0.000
Table 3 shows the mean varus TFA across the ages and gender. There was no significant difference in the varus knee angles between males and females.
Table 3.
Mean varus TFA ± standard deviation
| Age (years) | Varus angles (°) male | Varus angles (°) female | P value |
|---|---|---|---|
| Mean ± SD | Mean ± SD | ||
| 3 | 4.61 ± 1.88 | 3.93 ± 0.93 | 0.175 |
| 4 | 3.38 ± 1.25 | 3.50 ± 1.12 | 0.879 |
| 5 | 3.30 ± 0.97 | 4.67 ± 1.76 | 0.310 |
| 6 | 3.75 ± 0.35 | 0 | — |
| 7 | 4.38 ± 1.03 | 2.75 ± 1.06 | 0.145 |
| 8 | 3.00 ± 1.32 | 3.25 ± 0.35 | 0.819 |
| 9 | 4.00 ± 0.00 | 0 | — |
| 10 | 0 | 0 | — |
| 11 | 3.00 ± 0.00 | 0 | — |
| 12 | 0 | 0 | — |
| 13 | 0 | 0 | — |
| 14 | 0 | 0 | — |
| 15 | 0 | 0 | — |
| 16 | 3.00 ± 0.00 | 0 | — |
| 17 | 0 | 0 | — |
In Table 4, the highest mean valgus TFA was 6.56° ± 0.80° at 4 years in males and 6.94° ± 0.81° at 4 years in females. Female subjects had significantly higher mean TFA at 4, 6, 8, 15, and 17 years (P < 0.005).
Table 4.
Mean valgus TFA ± standard deviation amongst male and female subjects at different ages
| Age (years) | Valgus angles (°) male Mean ± SD | Valgus angles (°) female Mean ± SD | P value |
|---|---|---|---|
| 3 | 5.99 ± 0.97 | 6.21 ± 0.82 | 0.121 |
| 4 | 6.56 ± 0.80 | 6.94 ± 0.81 | 0.001* |
| 5 | 5.49 ± 0.94 | 5.74 ± 0.88 | 0.076 |
| 6 | 5.16 ± 1.07 | 5.62 ± 1.29 | 0.006* |
| 7 | 5.05 ± 1.33 | 5.22 ± 1.17 | 0.320 |
| 8 | 4.07 ± 1.53 | 4.51 ± 1.49 | 0.036* |
| 9 | 3.37 ± 1.47 | 3.50 ± 1.34 | 0.486 |
| 10 | 2.91 ± 1.42 | 3.08 ± 1.42 | 0.369 |
| 11 | 3.06 ± 1.55 | 3.14 ± 1.55 | 0.694 |
| 12 | 2.51 ± 1.51 | 2.57 ± 1.50 | 0.788 |
| 13 | 2.34 ± 1.52 | 2.45 ± 1.54 | 0.576 |
| 14 | 2.24 ± 1.55 | 2.40 ± 1.57 | 0.459 |
| 15 | 1.85 ± 1.52 | 2.73 ± 1.53 | 0.000* |
| 16 | 1.98 ± 1.11 | 2.20 ± 1.13 | 0.157 |
| 17 | 1.82 ± 1.29 | 2.19 ± 0.98 | 0.023* |
*statistically significant
Figure 2 shows that valgus TFA decreases with increasing age from 4 to 17 years in both males and females.
Figure 2.
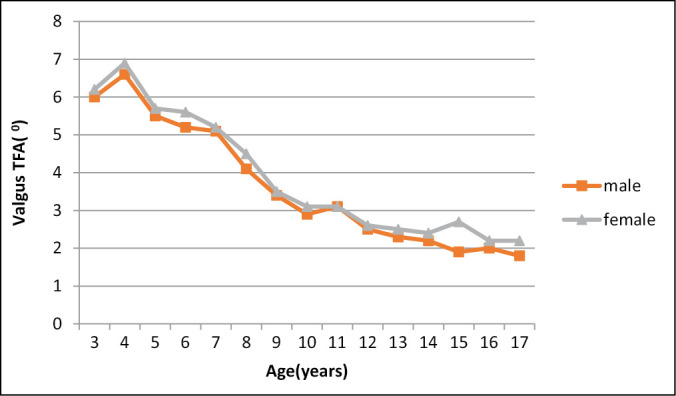
Relationship between valgus TFA of subjects and age
Discussion
Knowledge about changes in the alignment of the lower extremities with growth and its relationship to age and sex is very important. Accurate knowledge of such a change in any particular geography is necessary to differentiate the pathologic conditions from normal variations. Mild to moderate bowing of lower extremities is a common finding in infants and young children, and physiological knock-knees, which appear by 3–4 years of age are well defined.[8] The physiological variation in knee angle often causes apprehension among parents. Knowledge of normal variation is important for the explanation of some informative details, about the normal development of children to parents as well as to avoid unnecessary investigations, such as exposure to radiation and inappropriate use of a brace, which when not indicated might hinder natural development.[7]
In this study, the clinical method using a standard goniometer with an extendable arm was used to assess the TFA. Most of the subjects (97.6%) were found to have a valgus TFA. This is similar to other studies. Oginni et al.[9] reported that varus knee alignment was uncommon after 2 years of age. Health and Staheli[10] also reported that the presence of varus after 2 years is abnormal. Hence, a measurable varus angle at this period of age may be considered abnormal and needs detailed evaluation and follow-up.
Many studies have been carried out to define the normal range of values of knee angle, including the peak valgus angle. However, some of these studies have shown differences in normal values amongst different races. In this index study, the age at which peak valgus angulation occurred was between 3 and 4 years. This was in contrast to studies conducted by Mathew and Madhuri[11]and Saini et al.[12]where peak valgus angulation was seen between 5–6 and 6–7 years, respectively. Both studies were done on an Indian population.
In a study conducted by Cheng et al,[13] a similar peak valgus angle was noted at 3 years. They demonstrated a steady decrease in TFA from 8° valgus at age 3.5 years, which reversed gradually to reach the plateau of 1° valgus at age 8.5 years.
In this index study, the mean valgus angle of 6.56 ± 0.80 at 4 years decreased significantly to a mean of 1.82 ± 1.29 by 17 years old. This was like the study done by Harcourt,[14] in southeastern Nigeria, which showed that the mean TFA was 7.58 ± 2.05 at 4 years and this diminished progressively with increasing age.
This was like the study by Omololu et al.,[15] where it was found that most children had maximum bowing at 1–3 years and this reduced to neutral or 0° at of 5 years in girls and 7 years in males, all children had no bowing, that is, varus angle of 0° from 7 years upwards. In a study by Akinpelu et al.[16] on the influence of body positions on TFA measurement in children, their subjects showed a valgus knee angle with minimum values at 1 year, which peaked at 3 years and decreased thereafter.
In summary, the physiological changes in the TFA follow a similar pattern as established in literature but the degree and timing of the changes show some variations possibly attributable to race and ethnicity.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Thompson GH. Angular deformities of the lower extremities in children. In: Chapman MW, editor. Chapman’s Orthopaedic Surgery. 3rd ed. Philadelphia, PA: Lippincott William and Wilkins; 2001. pp. 4288–315. [Google Scholar]
- 2.Kaspiris A, Grivas TB, Vasiliadis E. Physiological alignment of lower limb changes during childhood: A clinical study in south-west Greece. Adv Biomed Res. 2010;1:249–51. [Google Scholar]
- 3.Levine AM, Drennan JC. Physiological bowing and tibia vara. J Bone Joint Surg (Am) 1982;64:1158–63. [PubMed] [Google Scholar]
- 4.Olufemi OO, Akinpelu AO, Odole AC. Development of tibiofemoral angle in a cohort of Nigerian children during the first 3 years of life. J Orthop. 2013;7:167–73. doi: 10.1007/s11832-012-0478-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Kaspir A, Zaphiropoulor C, Vasiliadis E. Range of variation of genu valgum and association with anthropometric characteristics and physical activity: Comparison between children aged 3-9 years. J Pediatr Orthop B. 2013;22:296–305. doi: 10.1097/BPB.0b013e328360f9a5. [DOI] [PubMed] [Google Scholar]
- 6.Lim K, Hin J, Lim A. Genu varum and valgum. In: Sivanathan S, Sherry E, Warnke P, Miller MD, editors. Mercer’s Textbook of Orthopaedics. London: Hodder Arnold; 2012. pp. 667–670. [Google Scholar]
- 7.Matthew SE, Madhuri V. Clinical tibiofemoral angle in South Indian children. Bone Joint Res. 2013;2:155–61. doi: 10.1302/2046-3758.28.2000157. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Arazi M, Ogun TC, Memik R. Normal development of the tibiofemoral angle in children A clinical study of 590 normal subjects from 3 to 17 years of age. J Pediatr Orthop. 2001;21:264–7. [PubMed] [Google Scholar]
- 9.Oginni LM, Badru OS, Sharp CA, Davie MW, Worsfold M. Knee angles and rickets in Nigeria Children. J Pediatr Orthop. 2004;24:403–7. doi: 10.1097/00004694-200407000-00011. [DOI] [PubMed] [Google Scholar]
- 10.Health CH, Staheli LT. Normal limits of knee angle in white children – Genuvarum and genuvalgum. J Paediatr Orthop. 1993;13:259–62. [PubMed] [Google Scholar]
- 11.Mathew SE, Madhuri V. Clinical tibiofemoral angle in South Indian children. Bone Joint Res. 2013;2:155–61. doi: 10.1302/2046-3758.28.2000157. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Saini UC, Bali K, Sheth B, Gahlot N, Gahlot A. Normal development of knee angle in healthy Indian children: A clinical study of 215 children. J Orthop. 2010;4:579–86. doi: 10.1007/s11832-010-0297-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Cheng JCY, Chan PS, Chiang SC, Hui PW. Angular and rotational profile of the lower limb in 2,630 Chinese children. J Pediatr Orthop. 1991;11:154–61. doi: 10.1097/01241398-199103000-00003. [DOI] [PubMed] [Google Scholar]
- 14.Harcourt SL. Clinical assessment of tibiofemoral angle in children 4-7 years of age in Enugu. Dissertation submitted to the National Postgraduate Medical College of Nigeria. 2004 [Google Scholar]
- 15.Omololu B, Tella A, Ogunlade SO, Adeyemo AA, Adebisi A, Alonge TO, et al. Normal values of knee angle, intercondylar and intermalleolar distance in Nigerian children. West Afr J Med. 2003;22:301–4. doi: 10.4314/wajm.v22i4.28051. [DOI] [PubMed] [Google Scholar]
- 16.Akinpelu AO, Tella BA, Oyewole OO, Odole AC. Influence of body position on tibiofemoral angle measurement in children. Int Journ Ortho Surg. 2013;21:1–5. [Google Scholar]