

Abstract
Objective:
Dual use of combustible cigarettes and e-cigarettes is common among U.S. tobacco users, yet mis-perceptions about the harm of dual use persist, often oversimplifying its multifaceted exposure and health impacts. To address this gap, we evaluated the association of prolonged dual use (consecutive use for more than 1 year) with psychosocial factors, including perceptions of absolute and relative harm of e-cigarettes, social norms, and intentions to quit smoking, among U.S. adult smokers over time.
Methods:
Using the data from Waves 1 to 5 (2013–2019) from the Population Assessment of Tobacco and Health (PATH) Study, we characterized dual use and prolonged dual use by sociodemographics and psychosocial factors among U.S. adult smokers. We examined the association between dual use, including prolonged dual use, and psychosocial factors over time using logistic regression.
Results:
Dual use of smokers decreased from 19.8 % in 2013 to 16.4 % in 2019, and prolonged dual use among dual users decreased from 40.0 % in 2013 to 27.4 % in 2019. Prolonged dual users, independent of frequency of use, presented significantly higher cigarette dependence than temporary dual users. The perception of absolute e-cigarette harm (perceiving e-cigarettes as very or extremely harmful) was negatively associated with prolonged dual use. No significant association was found between prolonged dual use and perception of relative e-cigarette harm (perceiving e-cigarettes are less harmful than cigarettes) as well as with intentions to quit smoking and beliefs that most people disapprove of e-cigarette use.
Conclusion:
Increased perceptions of absolute harm of e-cigarettes, rather than relative harm, appear to decrease prolonged dual use. Public health strategies should consider further emphasis in educating users of the absolute harm, as opposed to endorsing e-cigarette use as a harm reduction alternative, in their tobacco cessation efforts to further discourage dual use.
Keywords: E-cigarette, Cigarette, Harm perceptions, Harm reduction, Social norms
1. Introduction
Electronic cigarette (e-cigarette) use has increased dramatically since it was first introduced in the U.S. market in 2007. By 2021, 4.5 % of U.S. adults were reported as current e-cigarette users, and by 2023, 10 % of middle and high school students were reported as current e-cigarette users. (Birdsey et al., 2023; MMWR Morb Mortal Wkly Rep 2023) Opinions among the public, researchers, and health providers are divided on the potential health risks and benefits associated with e-cigarette use (Smith et al., 2021; National Academies of Sciences E, Division H, and M, Practice B on PH, and PH 2018) and current studies on whether e-cigarettes could help smokers completely quit or significantly reduce combustible cigarette consumption are not conclusive. (Hedman et al., 2021) Dual use of both combustible tobacco cigarettes and e-cigarette (henceforth as “dual users”), accounts for approximately 1.3 % of the 258.3 million adults aged 18 years old and older in the U.S. (Kramarow and Elgaddal, 2023) However, the heterogeneity among these users (i.e., temporary versus prolonged use) has not fully been explored. Data from the Population Assessment of Tobacco and Health (PATH) Study, which is a nationally representative, longitudinal study in the U.S. indicates that almost half of adult dual users remained dual users after one-year follow-up (Piper et al., 2020). As achieving 12-month abstinence is widely recognized as a critical milestone for predicting long-term smoking cessation success (Nohlert et al., 2013; Hoogendoorn et al., 2010), and health risks associated with dual use have not been conclusively settled (Reddy et al., 2021; Berlowitz et al., 2023), prolonged dual use, defined as beyond one year (henceforth “prolonged dual use”), is a significant concern that needs to be further studied.
When evaluating the health risks associated with tobacco products, both frequency and duration of exposure are critical dimensions to consider. (Fagerström, 2002) Frequent tobacco use, such as daily or multiple times a day, leads to a cumulative exposure to toxicants and carcinogens, increasing health risks. (Inoue-Choi et al., 2020) Meanwhile, the length of use, independent of frequency, also plays a substantial role in the exposure and health risks from tobacco products. (Bhatt et al., 2018) A recent study found that even minimal lifetime smoking—quantified as low as 6.4 pack-years—results in an increased risk of emphysema when compared to non-smokers. (Mathew et al., 2019) Given the diverse patterns of consumption among dual users, many of whom transition between intermittent use of different tobacco products at various intensities, it is crucial to classify and examine these individuals by duration of use. An analysis that considers the duration of dual use — a factor not highlighted in earlier studies — is essential for a thorough understanding of the health implications associated with this use pattern.
Harm perception is an important factor of health behaviors. Research has shown that individuals who perceived tobacco use as harmful were more likely to engage in harm reduction strategies, such as quitting or reducing tobacco use. (Elton-Marshall et al., 2020; Lozano et al., 2019) However, previous research on harm perception has focused on combustible cigarettes and the few studies that have assessed e-cigarettes have predominantly focused on comparing the perception of relative harm of e-cigarettes compared to cigarettes. (Xu et al., 2016) Perceptions of e-cigarette use are evolving and vary widely (Elton--Marshall et al., 2020; Huang et al., 2019), with many users considering them to be a safer alternative to combustible cigarettes. (Farsalinos and Polosa, 2014) This viewpoint oversimplifies the differences in harm between e-cigarettes and conventional cigarettes, and the complex exposure and health implications of prolonged dual use. Currently, the understanding of the absolute harm from e-cigarettes remained under-explored, which may have distinct health implications compared to the perceived absolute harm. (Lin et al., 2021) Additionally, social norms, referring to the shared beliefs of acceptable behaviors within a social group, were found to shift health behaviors including quitting and initiation of tobacco product uses. (Lozano et al., 2019; Cooper et al., 2016; Manning, 2009; Rivis and Sheeran, 2003) These norms differ from harm perception which focus on individual beliefs about health risks. Intention to quit smoking, often associated with e-cigarette use (Lozano et al., 2019; McDermott et al., 2020), is influenced by risk perception and social norms. With evolving e-cigarette devices and regulations (CDC 2020; U.S. Food and Drug Administration 2023) (Supplement Fig. 1), it is important to monitor the trends of these psychosocial factors and their association with prolonged dual use. Identifying the specific motivations and perceptions behind prolonged dual use can help clarify the actual risks involved, and craft targeted public health messages and interventions to reduce dual use, a pattern that still has unknown long-term health risks.
Our study aims to examine dual use with a focus on the duration of use, due to the absence of a uniform definition and the unclear health implications of prolonged dual use. We assessed the association between dual use, including prolonged dual use, with perceptions of both relative and absolute e-cigarette harm, social norms and intentions to quit smoking. First, we examined variations in dual use among U.S. adult smokers (aged ≥18 years) using data from the PATH Study from waves 1 to 5 (2013–2019). Specifically, we estimated the proportions of dual use and prolonged dual use stratified by demographic and psychosocial factors. We further examined whether the proportions of these factors were associated with dual use and prolonged dual use. Lastly, we explored the trends in the reasons of e-cigarette use other than harm reduction that potentially contribute to prolonged dual use.
2. Methods
2.1. Data source and study population
The PATH study is a nationwide longitudinal study, initiated by the National Institute on Drug Abuse (NIDA), National Institutes of Health (NIH), and the Food and Drug Administration (FDA), aiming to inform FDA’s tobacco regulations. The PATH Study is a representative sample of the U.S. Civilian noninstitutional population (CNP), conducted at approximately annual intervals (waves); survey weights are used to adjust for probabilities of selection into the survey as well as nonresponse. (United States Department Of Health And Human Services 2016) The timeline of data collection is presented in Supplement Fig. 1. A total of 32,320 adults (18 years and older) were selected by probability sampling across the U.S. as the Wave 1 Cohort, which was followed up annually, with each follow-up referred to as a wave. A replenishment cohort was recruited at Wave 4, together with the participants who completed the 4th follow-up from the Wave 1 cohort, to form the Wave 4 cohort. For our analysis, we used the Wave 1 cohort and their follow-up data from Waves 2 to 5, with annual follow-up rates of 83 %, 78 %, 74 % and 69 % for Waves 2 to 5, respectively. We included current established smokers (as defined in “tobacco use status” section) at each wave from Waves 1 to 5 as our analysis sample and conducted cross-sectional analysis within each wave.
2.2. Measures
2.2.1. Tobacco use status
Current tobacco use status was self-reported at each wave from Wave 1 to Wave 5. We assumed the status of tobacco product use remained unchanged until the next wave. Current established smokers were defined as respondents who have “smoked 100 or more cigarettes in their lifetime” and “currently smoke[s] every day or some days.” (United States Department Of Health And Human Services 2016) Fewer than 1 % of respondents with missing data to question on current e-cigarette use (“now use e-cigarettes”) were excluded from analysis of current waves. Respondents who were currently using tobacco products other than combustible cigarette and e-cigarette (including traditional cigar, cigarillo, filtered cigar, pipe, hookah, smokeless tobacco, snus, or dissolvable tobacco) “fairly regularly” (United States Department Of Health And Human Services 2016) (17 %, 15 %, 13 %, 15 % and 14 % from Wave 1 to 5 respectively) were excluded to reduce the impact from these products.
In this study, current exclusive smokers were defined as current established smokers who only use combustible cigarette. Current dual users were current established smokers who concurrently “use e-cigarettes every day or some days.” (United States Department Of Health And Human Services 2016) Questions about e-cigarette use were expanded to “electronic nicotine products” (EPRODS) (United States Department Of Health And Human Services 2016) beginning in Wave 2, including e-cigarette (a vape pen, personal vaporizer, or mod), e-cigar, e-pipe, and e-hookahs; all aforementioned EPRODS were treated as e-cigarettes in this study.
Dual use history of Wave 2 to 5 was collected using cigarette and e-cigarette use information from the prior visit. Dual use history of Wave 1 was determined by questions “were you smoking cigarettes every day, some days or not at all around this time 12 months ago” and “used e-cigarette around this time 12 months ago [every day, some days, not at all]” collected at Wave1. (United States Department Of Health And Human Services 2016) Prolonged dual use refers to dual use with a confirmed history for at least 12 months. In order to capture the frequency of dual use, dual use was also categorized as four mutually exclusive groups: everyday combustible cigarette and everyday e-cigarette use, everyday combustible cigarette and someday e-cigarette use, someday combustible cigarette and everyday e-cigarette use, someday combustible cigarette and someday e-cigarette use. A multivariate analysis was conducted to assess the association between prolonged dual use and frequency of dual use (Supplement Table 5).
2.2.2. Psychosocial factors
Full questions to measure each factor were derived from the PATH study and listed in detail in Supplement Table 1. Harm perception of e-cigarettes compared to cigarettes was categorized into “less harmful” and “about the same or more harmful.” Harm perception of e-cigarette alone was grouped into “not at all to somewhat harmful” and “very harmful or extremely harmful”. Social norms of e-cigarettes were measured by whether the respondent “thinks most people disapprove of using e-cigarettes” (Yes/No). Intention to quit smoking was categorized into “high” and “low” based on the median levels of interest in quitting smoking.
Reasons of e-cigarette use other than for the purpose of harm reduction were collected from all e-cigarette users by questions: “Use/used e-cigarette because: They are/were affordable” (Yes/No), “Can/could use it in places where smoking cigarettes is/was not allowed” (Yes/No), “They might be less harmful to people around me than cigarettes” (Yes/No), and “It comes/came in flavors I like/liked” (Yes/No).
2.2.3. Covariates
Self-reported sociodemographics (age, sex, race/ethnicity, education, and household income) and self-reported physical and mental health status were included at current wave (Supplement Table 1). (Chang et al., 2019) Nicotine dependence on cigarettes (cigarette dependence) and e-cigarettes (e-cigarette dependence) was measured by 11 Wisconsin Inventory of Smoking Dependence Motives (WISDM) items and four Nicotine Dependence Syndrome Scale (NDSS) items derived from Strong et al. (2017) on a sum scale of 75 with higher scores indicative greater dependence. (Strong et al., 2017)
2.3. Statistical analyses
We used a Sankey diagram to present the composition and transitions of dual use (raw counts) over five waves. We estimated the weighted percentage (95 % confidence interval [CI]) for dual use status of Wave 1 to 5 across social-demographic factors, self-reported health conditions, nicotine dependence, psychosocial factors, and duration of dual use (prolonged dual use). Unadjusted and multivariable adjusted logistic regression models were applied to estimate odds ratios (OR, 95 % CI) for dual use associated with psychosocial factors in Wave 1 to 5 separately, adjusting for sociodemographic characteristics, health conditions and nicotine dependence. Unadjusted and multivariable adjusted logistic regression models were also used to estimate OR (95 % CI) for prolonged dual use associated with psychosocial factors and reasons of e-cigarette use among dual users.
All analyses were conducted in R 4.2.2 (R Foundation, Vienna, Austria) using the survey 4.2–1 package. Data were weighted by the cross-sectional weight (Wave1) or single wave longitudinal weights to Wave 1 Cohort (Wave 2–5) provided by the PATH Study to yield nationally representative estimates. Variances were computed using a balanced repeated replication method with Fay’s coefficient adjustment value set at 0.3. (Judkins, 1990)
3. Results
Among a total of 9474 smokers with no established use of nicotine products other than combustible cigarettes and e-cigarettes at Wave 1, 1928 individuals (19.8 %, 95 % confidence interval [CI]: 18.9 to 20.8 %) reported current dual use. Fig. 1 illustrates the composition and transitions of dual users across waves. Consistently, around 30 % of dual users remained as dual users in the next wave (Supplement Table 2). The dual users who became exclusive smokers in the next wave increased from 34 % in Wave 1 to 46 % in Wave 2, decreased to 39 % in Wave 3 and further declined to 28 % in Wave 4. Among dual users, the proportion maintaining cigarette smoking in the next wave (including dual use and exclusive smoking) constituted the majority, with the prevalence ranging from 73 % in Wave 2 to 59 % in Wave 4.
Fig. 1.

Composition and transitions of dual use across 5 waves from the PATH study: a Sankey diagram representation. Abbreviations of the categories: Dual: Dual use; Smk: Exclusive smoking; AbSmk: Abstinence of smoking (Includes both exclusive e-cigarette user and no use of either cigarette or e-cigarette); LTF: Lost to follow-up. Notes: The width of the bands connecting the categories between waves indicates the number of individuals transitioning from one state to another. For example, a band with a width of around 3/10 of the ‘Wave1 - Dual’ transitioned to ‘Wave2 - Dual’ suggests around 30 % of individuals remained in the ‘Dual’ category from the first to the second wave. Detailed counts of each category were presented in Table S2. This figure focused on transitional patterns of dual use only. The branching of bands between waves signifies individuals moving from one category to dual use or from dual use to another category, reflecting changes in dual use over time.
3.1. Characteristics of the dual users at baseline (Wave 1)
Compared to exclusive smokers, dual users were more likely to be aged 25–34 years old (26.3 %, 95 %CI: 24.1 %–28.6 %), female (52.2 %, 95 %CI: 49.7 %–54.7 %), non-Hispanic White (75.8 %, 95 % CI: 73.5 %–78.1 %), have a household income of ≥$50,000 (30.2 %, 95 %CI: 27.4 %–33.1 %), some college or associate’s degree (38.4 %, 95 % CI: 35.7 %–41.1 %) and worse self-reported mental health (28.4 %, 95 %CI: 25.8 %–31.0 %) (Table 1). Cigarette dependence of dual users (mean: 45.0 [95 %CI: 44.1–45.8]) was significantly higher than exclusive smokers (mean: 41.8 [95 %CI: 41.3–42.3]). Around 80.2 % (95 %CI: 79.0 %–81.5 %) exclusive smokers were daily (everyday) smokers, which showed almost no differences compared to that of dual users (80.7 %, 95 %CI: 78.5, 82.8 %). The proportion of those who perceived less harm of e-cigarettes compared to cigarettes was higher among dual users (71.4 %, 95 %CI: 69.3 %–73.5 %), and dual users displayed significantly higher interest in quitting smoking (69.1 %, 95 %CI: 66.0 %–72.2 %) compared to exclusive smokers.
Table 1.
Characteristics of established smokers by dual use status at PATH Wave 1.
| Characteristics | Dual use status | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Total | Exclusive smokers | All dual users | Duration of dual use | ||||||||||||
| Prolonged dual use | Temporary dual use | ||||||||||||||
| (N = 9474) | (n = 7546) | (n = 1928) | (n = 764) | (n = 1164) | |||||||||||
| no. | % | %(95 % CI) | no. | % | %(95 % CI) | no. | % | %(95 % CI) | no. | % | %(95 % CI) | no. | % | %(95 % CI) | |
| Age, year | |||||||||||||||
| 18–24 | 1656 | 11.1 | (10.4, 11.8) | 1273 | 10.7 | (9.9, 11.4) | 383 | 12.7 | (11.2, 14.2) | 136 | 11.3 | (9.1, 13.5) | 247 | 13.6 | (11.6, 15.6) |
| 25–34 | 2125 | 23.4 | (22.4, 24.3) | 1654 | 22.6 | (21.6, 23.7) | 471 | 26.3 | (24.1, 28.6) | 172 | 23.8 | (20.2, 27.3) | 299 | 28.0 | (25.5, 30.6) |
| 35–44 | 1765 | 19.5 | (18.5, 20.5) | 1374 | 19.0 | (18.0, 19.9) | 391 | 21.8 | (19.5, 24.0) | 173 | 24.4 | (20.4, 28.4) | 218 | 20.0 | (17.7, 22.3) |
| 45–54 | 1857 | 21.2 | (20.3, 22) | 1508 | 21.6 | (20.6, 22.6) | 349 | 19.4 | (17.5, 21.4) | 142 | 20.1 | (16.7, 23.4) | 207 | 19.0 | (16.6, 21.4) |
| >=55 | 2070 | 24.9 | (23.9, 25.9) | 1737 | 26.1 | (25.0, 27.2) | 333 | 19.8 | (17.9, 21.6) | 140 | 20.5 | (16.9, 24.1) | 193 | 19.3 | (17.0, 21.6) |
| Male | 4533 | 51.1 | (50.0, 52.3) | 3670 | 52.0 | (50.8, 53.2) | 863 | 47.8 | (45.3, 50.3) | 349 | 48.8 | (44.8, 52.8) | 514 | 47.2 | (44.0, 50.3) |
| Race/ethnicity | |||||||||||||||
| Non-Hispanic white | 6361 | 70.0 | (68.9, 71.2) | 4953 | 68.6 | (67.2, 70.1) | 1408 | 75.8 | (73.5, 78.1) | 415 | 74.0 | (70.9, 77.1) | 650 | 77.0 | (74.0, 79.9) |
| Hispanic | 1218 | 11.2 | (10.5, 11.9) | 991 | 11.4 | (10.6, 12.1) | 227 | 10.4 | (8.7, 12.0) | 84 | 9.9 | (7.5, 12.2) | 143 | 10.7 | (8.5, 12.9) |
| Non-Hispanic black | 1218 | 12.8 | (12.0, 13.6) | 1076 | 14.1 | (13.1, 15.1) | 142 | 7.4 | (5.9, 8.9) | 59 | 7.8 | (5.9, 9.7) | 83 | 7.2 | (5.3, 9.0) |
| Others | 677 | 6.0 | (5.4, 6.6) | 526 | 5.9 | (5.2, 6.6) | 151 | 6.4 | (5.2, 7.7) | 76 | 8.4 | (6.0, 10.8) | 75 | 5.2 | (3.8, 6.5) |
| Income | |||||||||||||||
| <$10,000 | 1927 | 20.2 | (19.1, 21.4) | 1572 | 20.9 | (19.6, 22.2) | 355 | 17.6 | (15.5, 19.6) | 136 | 16.8 | (13.6, 20.0) | 219 | 18.1 | (15.8, 20.4) |
| $10,000 to $24,999 | 2464 | 27.7 | (26.6, 28.9) | 1966 | 27.9 | (26.8, 29.1) | 498 | 26.8 | (24.4, 29.3) | 197 | 26.1 | (22.4, 29.8) | 301 | 27.3 | (24.4, 30.2) |
| $25,000 to $49,999 | 2159 | 25.7 | (24.6, 26.8) | 1727 | 25.8 | (24.6, 27.0) | 432 | 25.4 | (23.2, 27.5) | 166 | 25.0 | (21.2, 28.7) | 266 | 25.6 | (22.9, 28.3) |
| ≥$50,000 | 2091 | 26.3 | (25.0, 27.7) | 1605 | 25.4 | (24.0, 26.7) | 486 | 30.2 | (27.4, 33.1) | 201 | 32.1 | (28.1, 36.1) | 285 | 29.0 | (25.8, 32.2) |
| Education | |||||||||||||||
| Less than High School | 1604 | 16.2 | (15.3, 17.1) | 1340 | 16.9 | (15.9, 17.9) | 264 | 13.3 | (11.6, 14.9) | 107 | 13.4 | (10.3, 16.5) | 157 | 13.2 | (11.2, 15.2) |
| Some college or associates degree | 3330 | 33.2 | (32.0, 34.5) | 2562 | 32.0 | (30.7, 33.3) | 768 | 38.4 | (35.7, 41.1) | 294 | 37.8 | (34.1, 41.4) | 474 | 38.7 | (35.1, 42.4) |
| GED or High school graduate | 3414 | 38.9 | (37.6, 40.1) | 2772 | 39.9 | (38.4, 41.3) | 642 | 34.8 | (32.5, 37.2) | 254 | 34.0 | (30.5, 37.6) | 388 | 35.4 | (32.0, 38.7) |
| Bachelor’s or Advanced degree | 1055 | 11.7 | (10.9, 12.5) | 813 | 11.3 | (10.4, 12.2) | 242 | 13.5 | (11.7, 15.3) | 105 | 14.8 | (12.0, 17.7) | 137 | 12.7 | (10.4, 15.0) |
| Physical health | |||||||||||||||
| Above Good | 3139 | 33.0 | (31.7, 34.2) | 2498 | 33.0 | (31.7, 34.3) | 641 | 32.7 | (30.0, 35.4) | 242 | 31.2 | (27.3, 35.1) | 399 | 33.7 | (30.8, 36.5) |
| Good | 3804 | 40.5 | (39.4, 41.6) | 3014 | 40.2 | (38.9, 41.5) | 790 | 41.8 | (39.3, 44.4) | 313 | 41.4 | (37.5, 45.3) | 477 | 42.1 | (39.2, 45.0) |
| Less than Good | 2516 | 26.5 | (25.3, 27.7) | 2021 | 26.8 | (25.5, 28.0) | 495 | 25.5 | (23.1, 27.9) | 207 | 27.4 | (23.1, 31.7) | 288 | 24.2 | (21.7, 26.7) |
| Mental health | |||||||||||||||
| Above Good | 4074 | 43.8 | (42.5, 45.0) | 3262 | 44.0 | (42.6, 45.4) | 812 | 42.9 | (40.3, 45.5) | 320 | 42.7 | (38.5, 46.9) | 492 | 43.0 | (40.1, 45.9) |
| Good | 2901 | 31.0 | (30.0, 32.0) | 2355 | 31.6 | (30.4, 32.7) | 546 | 28.7 | (26.6, 30.8) | 226 | 29.9 | (26.3, 33.5) | 320 | 27.9 | (25.1, 30.7) |
| Less than Good | 2472 | 25.3 | (24.1, 26.4) | 1908 | 24.5 | (23.2, 25.7) | 564 | 28.4 | (25.8, 31.0) | 215 | 27.4 | (23.5, 31.3) | 349 | 29.1 | (26.4, 31.8) |
| Perceive e-cig less harmful than cigarette | 4580 | 53.4 | (52.1, 54.8) | 3231 | 48.5 | (46.9, 50.0) | 1349 | 71.4 | (69.3, 73.5) | 542 | 72.5 | (68.7, 76.2) | 807 | 70.7 | (68.1, 73.3) |
| High interest in quitting smoking | 4067 | 65.1 | (63.7, 66.6) | 3046 | 63.9 | (62.2, 65.6) | 1012 | 69.1 | (66.0, 72.2) | 190 | 68.9 | (64.5, 73.3) | 393 | 69.2 | (65.4, 73.1) |
| CIG dependence, mean (95 % CI) | 9331 | 42.5 | (42, 42.9) | 7526 | 41.8 | (41.3, 42.3) | 1905 | 45.0 | (44.1, 45.8) | 755 | 46.4 | (45.2, 47.7) | 1150 | 44.0 | (42.9, 45.1) |
| ECIG dependence, mean (95 % CI) | NA | NA | NA | NA | NA | NA | 714 | 25.1 | (24.0, 26.3) | 360 | 24.6 | (23.1, 26.1) | 354 | 25.7 | (24.1, 27.4) |
| Daily cigarette use | 7587 | 80.3 | (79.2, 81.4) | 6041 | 80.2 | (79.0, 81.5) | 1546 | 80.7 | (78.5, 82.8) | 621 | 82.1 | (78.9, 85.2) | 925 | 79.7 | (77.0, 82.5) |
| Daily e-cigarette use | NA | NA | NA | NA | NA | NA | 198 | 15.6 | (13.6, 17.6) | 112 | 16.4 | (14.0, 18.7) | 186 | 14.4 | (11.5, 17.3) |
The distribution of prolonged dual users showed no significant difference compared to temporary dual users across demographics and psychosocial factors at baseline. Both cigarette dependence (mean: 46.5 [95 %CI: 45.2–47.7]) and e-cigarette dependence (mean: 25.7 [95 %CI: 24.1–27.4]) were higher among prolonged dual users than among temporary dual users. The proportion of daily cigarette use among prolonged dual users (82.1 %, [95 %CI: 78.9, 85.2]) was similar to that among temporary dual users (79.7 %, [95 %CI:77.0 %, 82.5 %]). The proportion of daily e-cigarette use among prolonged dual users (16.4 %, [95 %CI: 14.0 %, 18.7 %]) was also similar to that among temporary dual users (14.4 %, [95 %CI:11.5 %, 17.3 %]).
3.2. Changes in characteristics of dual users
The proportion of current dual use among U.S. adult smokers was 19.8 % (95 CI: 18.9 %–20.8 %), 19.9 % (95 CI: 18.8 %–21.1 %), 14.0 % (95 CI:13.1 %–14.9 %), 12.4 % (95 CI:11.4 %–13.3 %), and 16.4 % (95 CI:15.1–17.7), from Wave 1 to 5 respectively. Supplemental Table 3 displayed the proportion of dual use among established smoker by subpopulations over time. Supplemental Table 4 displayed the characteristics of dual users at each wave. The age distribution of dual users tended to skew younger (under 44 years old) when comparing Wave 5 to Wave 1. The proportion of daily e-cigarette users among dual users from Wave1 (15.6 %, [95 %CI: 13.6, 17.6]) greatly increased to 32.2 % (95 % CI: 28.8 %, 35.5 %) (Supplement Table 4). Cigarette dependence of dual users decreased from 45.0 (95 %CI: 44.1–45.8) in Wave 1 to 39.5 (95 % CI: 38.3, 40.8) to Wave 5.
Fig. 2a depicts the proportions of prolonged use and psychosocial factors among dual users across waves. The proportion of prolonged dual use among dual users decreased from Wave 1 (40.0 %, 95 CI: 37.5 %–42.5 %) to Wave 5 (27.4 %, 95 CI: 24.1 %–30.7 %). Dual users who perceived e-cigarette as less harmful than combutible cigarettes decreased from Wave 1 (71.4 %, 95 % CI: 69.3 %–73.5 %) to Wave 5 (39.0 %, 95 % CI: 36.2 %–41.9 %), while dual users who perceived e-cigarette to be very or extremely harmful increased from Wave 3 (19.5 %, 95 % CI: 17.0 %–22.0 %) to 5 (31.1 %, 95 % CI: 28.2 %–34.0 %). Dual users who reported high interest in quitting cigarettes significantly dropped from Wave 1 (69.1 %, 95 %CI: 66.0 %–72.2 %) to Wave 5 (54.9 %, 95 %CI: 51.3 %–58.6 %). Dual users who reported thinking that most people disapprove of e-cigarettes significantly increased from Wave 2 (43.7 %, 95 %CI: 41.3 %–46.2 %) to Wave 5 (63.9 %, 95 %CI: 60.5 %–67.2 %).
Fig. 2.
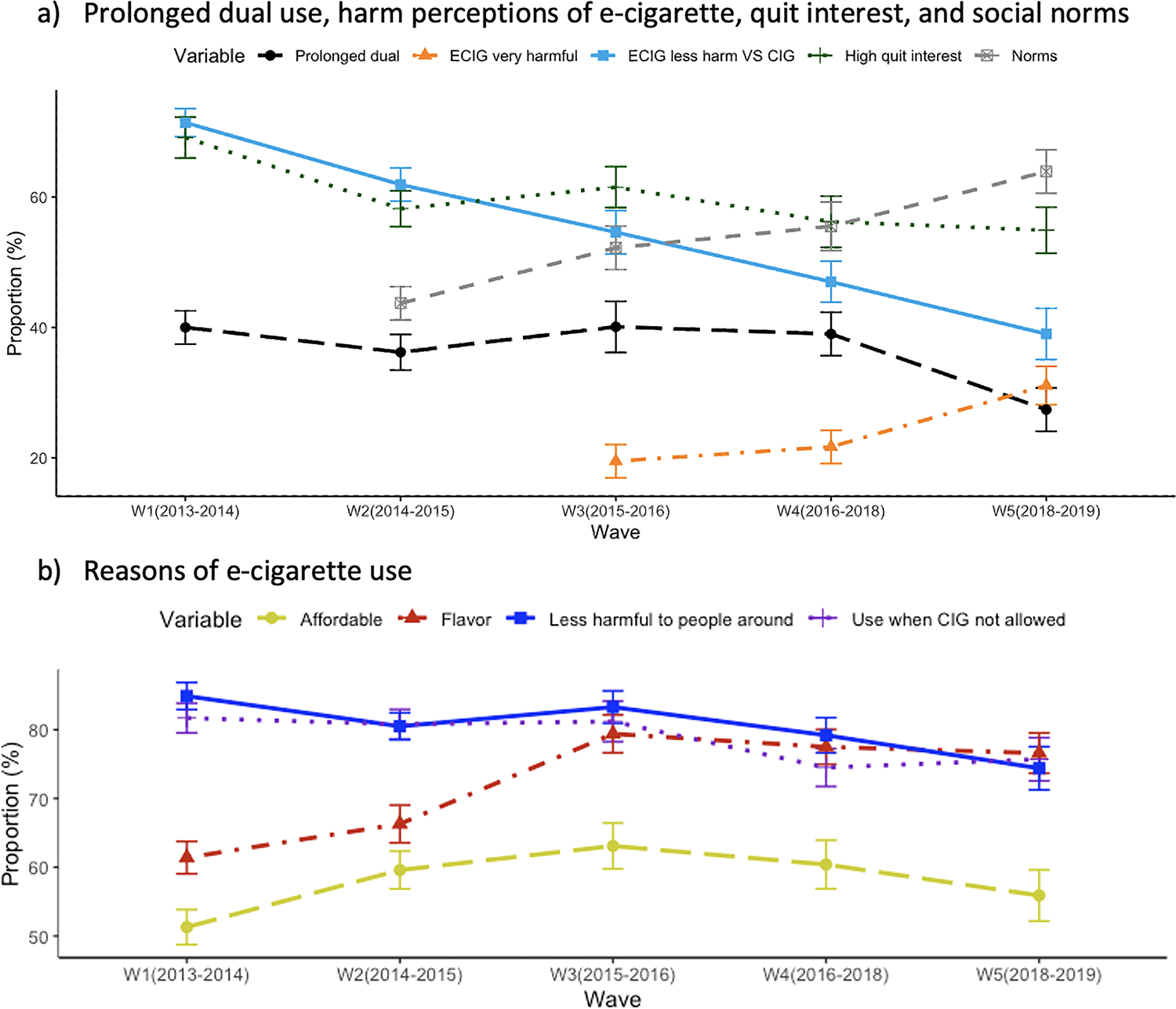
Prolonged dual use and risk factors among dual users in the PATH study from Wave 1 to 5.
Almost 85 % of dual users reported using e-cigarettes because e-cigarettes might be less harmful to people around them and 82 % of dual users reported using e-cigarettes because e-cigarettes can be used when/where cigarettes are not allowed (Fig. 2b). Dual users who used e-cigarettes because they come with flavors that they liked significantly increased from Wave 1 (61.4 %, 95 %CI: 59.0 %–63.8 %) to Wave 3 (76.6 %, 95 %CI: 74.7 %–79.5 %).
3.3. Dual use and risk factors
Individuals who were dual users, as compared to exclusive smokers, were more likely to perceive less harm of e-cigarette compared to cigarette and have higher interest in quitting smoking (Table 2A), although the adjusted odds ratio for higher quit interest was not statistically significant at Wave 1 and Wave 4. On the contrary, dual users were less likely to perceive e-cigarette alone to be very or extremely harmful consistently across Wave 3 to 5 (all p-values <0.001). Reporting a belief that most people disapprove of e-cigarette use was also negatively associated with dual use across all waves (all p-values <0.05).
Table 2.
Results of multivariable logistic regression analysis.
| Part A. Dual use and psychosocial factors | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Factors | Wave1 | Wave2 | Wave3 | Wave4 | Wave5 | ||||||
| Perceived less harm of ECIG compared to CIG | OR (95 % CI) | 2.66 | (2.36, 2.99)* | 3.45 | (3.06, 3.88)* | 3.87 | (3.32, 4.50)* | 4.01 | (3.42, 4.69)* | 4.38 | (3.60, 5.33)* |
| AOR (95 % CI) | 2.56 | (2.25, 2.92)* | 3.38 | (3.00, 3.81)* | 4.21 | (3.47, 5.11)* | 4.01 | (3.33, 4.83)* | 3.76 | (3.05, 4.64)* | |
| Perceived ECIG very of extremely harmful | OR (95 % CI) | NA | NA | 0.29 | (0.24, 0.35)* | 0.29 | (0.24, 0.34)* | 0.35 | (0.30, 0.41)* | ||
| AOR (95 % CI) | 0.28 | (0.22, 0.35)* | 0.28 | (0.23, 0.34)* | 0.37 | (0.32, 0.44)* | |||||
| High interest in quitting smoking | OR (95 % CI) | 1.26 | (1.06, 1.50)* | 1.30 | (1.14, 1.48)* | 1.52 | (1.30, 1.78)* | 1.22 | (1.02, 1.47)* | 1.20 | (1.01, 1.41)* |
| AOR (95 % CI) | 1.15 | (0.96, 1.38) | 1.24 | (1.08, 1.43)* | 1.56 | (1.32, 1.83)* | 1.18 | (0.96, 1.45) | 1.26 | (1.03, 1.54)* | |
| Think most people disapprove of ECIG | OR (95 % CI) | NA | 0.67 | (0.60, 0.75)* | 0.65 | (0.56, 0.75)* | 0.64 | (0.54, 0.75)* | 0.67 | (0.56, 0.80)* | |
| AOR (95 % CI) | 0.69 | (0.62, 0.77)* | 0.61 | (0.51, 0.73)* | 0.66 | (0.56, 0.80)* | 0.77 | (0.64, 0.93)* | |||
| Part B. Prolonged dual use, psychosocial factors and reasons of e-cigarette use | |||||||||||
| Factors | Wave1 | Wave2 | Wave3 | Wave4 | Wave5 | ||||||
| Psychosocial factors | |||||||||||
| Perceived less harm of ECIG compared to CIG | OR (95 % CI) | 1.09 | (0.86, 1.38) | 1.19 | (0.95, 1.50) | 1.13 | (0.88, 1.46) | 1.47 | (1.13, 1.91) | 1.30 | (0.95, 1.78) |
| AOR (95 % CI) | 1.12 | (0.86, 1.46) | 1.12 | (0.88, 1.42) | 1.21 | (0.88, 1.66) | 1.38 | (0.99, 1.91) | 1.26 | (0.84, 1.90) | |
| Perceived ECIG very of extremely harmful | OR (95 % CI) | NA | NA | 0.59 | (0.42, 0.83)* | 0.67 | (0.44, 1.01) | 0.62 | (0.43, 0.88)* | ||
| AOR (95 % CI) | 0.53 | (0.33, 0.84)* | 0.74 | (0.50, 1.11) | 0.58 | (0.38, 0.87)* | |||||
| High interest in quitting smoking | OR (95 % CI) | 0.98 | (0.76, 1.26) | 1.25 | (0.95, 1.66) | 1.06 | (0.74, 1.51) | 1.33 | (0.99, 1.79) | 0.92 | (0.69, 1.23) |
| AOR (95 % CI) | 0.80 | (0.61, 1.04) | 1.19 | (0.89, 1.60) | 1.07 | (0.73, 1.56) | 1.11 | (0.81, 1.53) | 0.83 | (0.58, 1.19) | |
| Think most people disapprove of ECIG | OR (95 % CI) | NA | 1.00 | (0.79, 1.26) | 1.03 | (0.78, 1.37) | 0.83 | (0.61, 1,13) | 1.13 | (0.84, 1.51) | |
| AOR (95 % CI) | 1.08 | (0.82, 1.43) | 1.11 | (0.81, 1.52) | 0.81 | (0.57, 1.14) | 0.98 | (0.70, 1.38) | |||
| Reasons of e-cigarette use | |||||||||||
| Affordable | OR (95 % CI) | 1.05 | (0.86, 1.28) | 1.07 | (0.86, 1.35) | 0.90 | (0.68, 1.20) | 0.89 | (0.68, 1.17) | 1.37 | (1.00, 1.87) |
| AOR (95 % CI) | 0.99 | (0.86, 1.32) | 1.03 | (0.80, 1.33) | 0.88 | (0.61, 1.29) | 0.79 | (0.57, 1.09) | 1.31 | (0.92, 1.86) | |
| Flavor | OR (95 % CI) | 1.06 | (0.86, 1.30) | 0.91 | (0.70, 1.18) | 0.79 | (0.57, 1.10) | 1.22 | (0.87, 1.70) | 1.88 | (1.21, 2.91) |
| AOR (95 % CI) | 1.17 | (0.93, 1.46) | 1.07 | (0.80, 1.44) | 0.77 | (0.50, 1.20) | 1.60 | (1.10, 2.33)* | 1.91 | (1.20, 3.04)* | |
| Less harmful to people around | OR (95 % CI) | 1.19 | (0.88, 1.60) | 1.44 | (1.04, 2.00)* | 0.98 | (0.70, 1.37) | 1.53 | (1.12, 2.10) | 1.70 | (1.23, 2.35)* |
| AOR (95 % CI) | 1.17 | (0.85, 1.62) | 1.41 | (0.99, 2.02) | 0.91 | (0.59, 1.42) | 1.39 | (0.95, 2.02) | 1.64 | (1.11, 2.40)* | |
| Use when CIG not allowed | OR (95 % CI) | 1.19 | (0.92, 1.53) | 1.68 | (1.24, 2.27)* | 1.22 | (0.85, 1.77) | 1.44 | (0.96, 2.14) | 1.55 | (1.03, 2.34)* |
| AOR (95 % CI) | 1.16 | (0.88, 1.54) | 1.51 | (1.06, 2.16)* | 0.98 | (0.63, 1.53) | 1.34 | (0.85, 2.11) | 1.65 | (1.06, 2.58)* | |
Note. OR=odds ratio; AOR=adjusted odds ratio; CI=confidence interval; NA=questions not available for this wave.
Adjusted multivariate regression models adjusted for age, sex, race/ethnicity, income, education, physical and mental health conditions, and cigarettes dependence.
p-value <0.05.
3.4. Prolonged dual use and risk factors
Prolonged dual use was not significantly associated with frequency of product use in Wave1 to Wave4 (Supplement Table 5). Only using cigarette someday and e-cigarette everyday in Wave5 was positively associated with prolonged dual use comparing to dual users using cigarette everyday and e-cigarette someday (Supplement Table 5).
Individuals who were prolonged dual users, as compared to temporary dual users, were less likely to perceive e-cigarette as very or extremely harmful in Waves 3 and 5 (Table 2B). No other psychosocial factors were observed to be associated with prolonged dual use, including perception of relative e-cigarette harm (perceiving e-cigarettes are less harmful that cigarettes), intentions to quit smoking and social norms that most people disapprove of e-cigarette use.
Prolonged dual use presented significant associations with the reasons of e-cigarettes being less harmful to other people and that e-cigarettes can be used when/where cigarettes are not allowed, but this was only found in certain waves. Using e-cigarettes because of the flavors was significantly associated with prolonged dual use with an AOR of 1.60 (95 %CI: 1.10–2.33) and 1.91 (95 %CI: 1.20–3.04) in Waves 4 and 5.
4. Discussion
In this study, we assessed the association of dual use, including prolonged dual use (consistent use of both products >1 year), which has never before been evaluated, with psychosocial factors using data from Waves 1 to 5 of the PATH study (2013–2019). Among all the psychosocial factors evaluated – intentions to quit smoking, social norms, perception of relative and absolute perception of harm – only the perception of absolute harm of e-cigarettes was negatively associated with prolonged dual use. Furthermore, we found that use of e-cigarettes for the enjoyment of flavors was potentially associated with prolonged dual use, given the popularity of a new generation of flavored e-cigarettes. Both these findings have implications to guide future directions on comprehensive tobacco cessation efforts. For example, public health campaigns could focus on educating users about the specific health risks of e-cigarettes to reduce prolonged dual use. Additionally, implementing regulations to restrict the availability of flavored e-cigarettes may be beneficial, as flavors are indicated as a contributing factor to prolonged use.
Despite considerable transitions between dual users and exclusive smokers over time, the majority of dual users persistently smoked cigarettes for durations extending to at least one year as evidenced by our study, which was also found from previous studies. (Piper et al., 2020; Barufaldi et al., 2021) In our assessment of overall dual use among U.S. adult smokers, we found that these users were strongly associated with higher intentions to quit smoking and perceptions of e-cigarettes being less harmful compared to cigarettes. We also found that dual users were less likely to perceive e-cigarettes alone as very or extremely harmful or to hold the norms that most people disapprove of e-cigarette use. Consistent with other studies, dual users in our study tended to be younger, female, non-Hispanic White individuals, with higher levels of education and household income, and among those with poor mental health conditions, when compared to exclusive cigarette smokers. (Chang et al., 2019; Hirschtick et al., 2021; Piper et al., 2019; Sweet et al., 2019) Our analyses found no demographic factors that distinguished prolonged dual users from temporary dual users. However, previous studies showed slightly different results by exploring the transition patterns of dual users, indicating that dual users who are white, male, and with higher educational attainment would be more likely to maintain dual use. (Piper et al., 2020; Coleman et al., 2019)
Cigarette dependence was identified as a key factor in predicting long-term cessation in smokers, and can make it more difficult for individuals to quit smoking. (Hyland et al., 2004) In our study, dual users exhibited higher cigarette dependence than exclusive smokers, and prolonged dual users exhibited higher cigarette dependence than temporary dual users. Higher cigarette dependence of prolonged dual users suggests that quitting smoking entirely after e-cigarette use can be challenging. Therefore, harm reduction strategies, which aim to reduce the negative health impacts from cigarette smoking, should consider prioritizing the prevention of additional addictions to multiple tobacco products. Prior research has predominantly focused on the frequency of dual usage of cigarettes and e-cigarettes to investigate its correlation with health risks and exposure levels (Borland et al., 2019). However, our research indicates that the frequency of dual use is distinct from the duration of such practices. We observed that the continuity of dual usage—defined as prolonged use—does not depend on whether individuals engage in daily or episodic (someday) consumption patterns. Thus, both regular and intermittent users may exhibit prolonged dual use behaviors. As previous studies suggest that even sporadic contact with tobacco products can escalate health risks (Mathew et al., 2019; Bhatta and Glantz, 2020), our findings indicate the critical importance of assessing dual use in terms of duration, independent of frequency.
The trends of a decrease in the prevalence of perceived harm of e-cigarettes compared to combustible cigarettes as well as an increase in prevalence of perceiving e-cigarettes as very or extremely harmful in this study parallels the trends in other national statistics. (Huang et al., 2019) The shift of the perceptions and the social norms of e-cigarettes being harmful likely reflects a growing awareness of the risks of addiction and uncertainty regarding the long-term health effects of e-cigarette use from recent research findings, government-mandated warnings, and media coverage of product risks. Several studies found that perceived less harm of e-cigarettes, motivations to quit smoking, social norms of perceived use of e-cigarettes by close friends and seeing e-cigarette use in public were positively associated with e-cigarette use and country-level e-cigarette use rate, (Elton-Marshall et al., 2020; Lozano et al., 2019; Cooper et al., 2016; East et al., 2019) emphasizing how perceptions of risks and potential benefits (e.g., smoking cessation) may play an important role as a harm reduction strategy. It is reflected in our study that cigarette smokers, who perceived e-cigarettes as less harmful than cigarettes, held the social norm of being in favor of e-cigarette use, and had a higher interest in quitting smoking, tended to be dual users. However, prolonged dual use was found to be only impacted by absolute harm perception of e-cigarettes, not the relative harm perception compared to cigarettes in our study, indicating that the relative risk and absolute risk of e-cigarettes may contribute differently to risk communication. Lack of accurate, consistent, and proactive absolute risk communications of e-cigarette use to the public may contribute to the confusion about the health risks of e-cigarettes and increase the potential for prolonged dual use.
While the perception of e-cigarette harm has increased over the years as seen in our study and other studies (Huang et al., 2019), and while we found a strong association of perceived harm and dual use, the prevalence of dual use among smokers decreased very slightly, indicating that it is still attractive for smokers to initiate or continue e-cigarette use for other reasons beyond harm reduction. Aside from using e-cigarettes as a harm reduction strategy, we found that dual users used e-cigarettes because they could be used in places when cigarettes are not allowed and that it reduces harm to people around the users, which are consistent with other studies. (Simonavicius et al., 2017) Meanwhile, our findings reveal an uptick, starting from Wave 3 (2015–2016), in dual users attributing their e-cigarette usage to the enjoyment of flavors, and significant associations between prolonged dual use and the enjoyment of flavors in subsequent Wave 4 (2016–2018) and Wave 5 (2018–2019). It’s noteworthy that this trend corresponds with the market introduction of PODs in 2015 and their subsequent rise in popularity. One explanation is that increased number of people who initiated PODs use due to enjoyment of flavor got addicted to nicotine because of high concentration of nicotine provided by PODs and become prolonged dual users. This adds the warning of preventing young people who use e-cigarettes for reasons other than harm reduction from being exposed to this product and at higher health risks than they expect.
4.1. Limitations and strengths
Our study was not without limitations. First, the harm perceptions and social norms were assessed using questions that may not fully capture various aspects of people’s understanding and opinions on e-cigarette use. This limitation could potentially lead to an incomplete representation of the true range and depth of harm perceptions and social norms, ultimately affecting the validity and applicability of our study findings to broader discussions on e-cigarette regulations. Second, due to the design of the PATH study, the duration of prolonged dual use varied by waves and any cessation and relapse between consecutive follow-ups was uncertain. Nevertheless, an “anniversary month” was assigned to each respondent by the PATH study design as a target data collection period to “improve the likelihood of the interviews taking place at 1-year intervals.” (United States Department Of Health And Human Services 2016) Third, the rapid product evolutions in the e-cigarette marketplace resulted in inconsistent terminology regarding e-cigarette use. For example, in the first two waves, a generic term “e-cigarettes” was used—while after Wave 2, ENPRODS was used to capture newer generations of vaping products. This variation in wording may affect the ability to make accurate comparisons across waves, although the majority of electronic products are still considered e-cigarettes. Fourth, polytobacco use is not uncommon (around 15 %) among tobacco users in our study. By excluding established users of other products, we may not be capturing results that truly generalize to the entire tobacco-using population. However, this approach allows us to concentrate on those who exclusively use both cigarettes and e-cigarettes, which is the primary target population of this study. Fifth, we should note that because the data were collected longitudinally, the comparison of changes over time was different from the comparisons of true cross-sectional survey data. For example, our respondents in Wave 2 were from the population that was previously selected into the Wave 1 Cohort and remained for Wave 2, which was not exactly the same as the population that was currently in scope for Wave 2. But the differences were subtle, as the composition of the U.S. population likely did not change substantially over the six-year study period. Thus, our results can still be considered representative of a cross-sectional U.S. population. Overall, we leveraged this nationally representative longitudinal data with a focus on dual use and associated psychosocial factors to monitor important trends of dual use and prolonged dual use associated with harm perceptions of e-cigarette a real-world setting.
5. Conclusion
Our investigation addresses previously understudied heterogeneity in dual use and explores the psychosocial factors that may drive prolonged dual use. Increased perceptions of absolute harm of e-cigarrettes, rather than relative harm compared to cigarette smoking, appear to decrease prolonged dual use, which suggest that presenting the absolute harm of e-cigarette use may be beneficial to prevent dual users from prolonged dual use. While the data in this paper do not allow for definitive causal associations, investigations of public health strategies to educate users about the absolute harm associated with both e-cigarettes and combustible cigarettes hold promise. Instead of endorsing e-cigarettes as a harm reduction alternative, the strategy could aim to discourage the prolonged dual use due to its potential unknown health risks.
Supplementary Material
Acknowledgements
We would like to extend our heartfelt thanks to all those who made this study possible. We express our sincere gratitude to Aleksandr B. Stefaniak for his invaluable suggestions and constant support on the manuscript.
Funding
This work was partially supported by the National Institute of Environmental Health Sciences (NIEHS) by the Food and Drug Administration (FDA) under Grant R01ES030025 (Rule) and by the Maryland Cigarette Restitution Fund under Grant PHPA-1896. The views expressed in this paper are those of the authors and do not necessarily represent the views of the funding agencies. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Declaration of competing interest
The authors declare the following financial interests/personal relationships which may be considered as potential competing interests:
Ana Rule reports financial support was provided by National Institute of Environmental Health Sciences. If there are other authors, they declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Footnotes
Human subjects
The IRB determined that this analysis, which uses publicly available and deidentified data, does not qualify as human subject research.
CRediT authorship contribution statement
Rui Chen: Writing – original draft, Project administration, Investigation, Formal analysis, Conceptualization. Angela Aherrera: Writing – review & editing, Investigation. Miranda R. Jones: Writing – review & editing, Conceptualization. Elizabeth A. Stuart: Writing – review & editing, Methodology. Meghan F. Davis: Writing – review & editing, Supervision, Project administration, Investigation. Ana M. Rule: Writing – review & editing, Supervision, Project administration, Investigation.
Supplementary materials
Supplementary material associated with this article can be found, in the online version, at doi:10.1016/j.heha.2024.100103.
References
- Barufaldi LA, Guerra RL, de Albuquerque R de CR, et al. , 2021. Risk of smoking relapse with the use of electronic cigarettes: a systematic review with meta-analysis of longitudinal studies. Tob. Prev. Cessat 29, 29. 10.18332/tpc/132964. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Berlowitz JB, Xie W, Harlow AF, et al. , 2023. Cigarette-E-Cigarette transitions and respiratory symptom development. Am. J. Prev. Med 64 (4), 556–560. 10.1016/j.amepre.2022.10.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bhatt SP, Kim Yil, Harrington KF, et al. , 2018. Smoking duration alone provides stronger risk estimates of chronic obstructive pulmonary disease than pack-years. Thorax 73 (5), 414–421. 10.1136/thoraxjnl-2017-210722. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bhatta DN, Glantz SA, 2020. Association of E-Cigarette use with respiratory disease among adults: a longitudinal analysis. Am. J. Prev. Med 58 (2), 182–190. 10.1016/j.amepre.2019.07.028. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Birdsey J, Cornelius M, Jamal A, et al. , 2023. Tobacco product use among U.S. middle and high school students — National Youth Tobacco Survey, 2023. MMWR. Morb. Mortal. Wkly. Rep 72 (44), 1173–1182. 10.15585/mmwr.mm7244a1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Borland R, Murray K, Gravely S, et al. , 2019. A new Classification system for describing concurrent use of nicotine vaping products alongside cigarettes (so-called “Dual Use”): findings from the ITC-4 country smoking and vaping wave 1 survey T. Addict Abingdon Engl. 114 (Suppl 1), 24–34. 10.1111/add.14570. [DOI] [PMC free article] [PubMed] [Google Scholar]
- CDC. E-cigarette, or vaping, product use associated lung injury (EVALI): case series and diagnostic approach-ClinicalKey. Published February 25, 2020. Accessed March 4, 2021. https://www-clinicalkey-com.proxy1.library.jhu.edu/#!/content/playContent/1-s2.0-S2213260019304151?returnurl=null&referrer=null.
- Chang YC, Lee YH, Liu CT, Shelley M, 2019. Patterns of e-cigarette use and self-reported health outcomes among smokers and non-smokers in the United States: a preliminary assessment. J. Subst. Use 24 (1), 79–87. 10.1080/14659891.2018.1510053. [DOI] [Google Scholar]
- Coleman B, Rostron B, Johnson SE, et al. , 2019. Transitions in electronic cigarette use among adults in the Population Assessment of Tobacco and Health (PATH) Study, Waves 1 and 2 (2013–2015). Tob. Control 28 (1), 50–59. 10.1136/tobaccocontrol-2017-054174. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cooper M, Creamer MR, Ly C, Crook B, Harrell MB, Perry CL, 2016. Social norms, perceptions and dual/poly tobacco use among Texas youth. Am. J. Health Behav 40 (6), 761–770. 10.5993/AJHB.40.6.8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- East KA, Hitchman SC, McDermott M, et al. , 2019. Social norms towards smoking and electronic cigarettes among adult smokers in seven European Countries: findings from the EUREST-PLUS ITC Europe Surveys. Tob. Induc. Dis 16 (2) 10.18332/tid/104417. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Elton-Marshall T, Driezen P, Fong GT, et al. , 2020. Adult perceptions of the relative harm of tobacco products and subsequent tobacco product use: longitudinal findings from waves 1 and 2 of the population assessment of tobacco and health (PATH) study. Addict. Behav 106, 106337 10.1016/j.addbeh.2020.106337. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fagerström K, 2002. The epidemiology of smoking. Drugs 62 (2), 1–9. 10.2165/00003495-200262002-00001. [DOI] [PubMed] [Google Scholar]
- Farsalinos KE, Polosa R, 2014. Safety evaluation and risk assessment of electronic cigarettes as tobacco cigarette substitutes: a systematic review. Ther. Adv. Drug Saf 5 (2), 67–86. 10.1177/2042098614524430. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hedman L, Galanti MR, Ryk L, Gilljam H, Adermark L, 2021. Electronic cigarette use and smoking cessation in cohort studies and randomized trials: a systematic review and meta-analysis. Tob. Prev. Cessat 7, 62. 10.18332/tpc/142320. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hirschtick JL, Mattingly DT, Cho B, et al. , 2021. Exclusive, dual, and polytobacco use among US adults by sociodemographic factors: results from 3 nationally representative surveys. Am. J. Health Promot 35 (3), 377–387. 10.1177/0890117120964065. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hoogendoorn M, Feenstra TL, Hoogenveen RT, van Mölken MPMHR, 2010. Long-Term effectiveness and cost-effectiveness of smoking cessation interventions in patients with COPD. Thorax 65 (8), 711–718. 10.1136/thx.2009.131631. [DOI] [PubMed] [Google Scholar]
- Huang J, Feng B, Weaver SR, Pechacek TF, Slovic P, Eriksen MP, 2019a. Changing perceptions of harm of e-cigarette vs cigarette use among adults in 2 US national surveys from 2012 to 2017. JAMa Netw. Open 2 (3), e191047 10.1001/jamanetworkopen.2019.1047. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Huang J, Duan Z, Kwok J, et al. , 2019b. Vaping versus JUULing: how the extraordinary growth and marketing of JUUL transformed the US retail E-Cigarette market. Tob. Control 28 (2), 146–151. 10.1136/tobaccocontrol-2018-054382. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hyland A, Li Q, Bauer JE, Giovino GA, Steger C, Cummings KM, 2004. Predictors of cessation in a cohort of current and former smokers followed over 13 years. Nicotine Tob. Res. Off J. Soc. Res. Nicotine Tob 6 (Suppl 3), S363–S369. 10.1080/14622200412331320761. [DOI] [PubMed] [Google Scholar]
- Inoue-Choi M, Christensen CH, Rostron BL, et al. , 2020. Dose-Response association of low-intensity and nondaily smoking with mortality in the United States. JAMA Netw. Open 3 (6), e206436 10.1001/jamanetworkopen.2020.6436. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Judkins DR, 1990. Fay’s method for variance estimation. J. Off. Stat 6 (3), 223. [Google Scholar]
- Kramarow EA, Elgaddal N, 2023. Current electronic cigarette use among adults aged 18 and over: united States, 2021. NCHS Data Brief 475, 1–8. [PubMed] [Google Scholar]
- Lin W, Martinez SA, Ding K, Beebe LA, 2021. Knowledge and perceptions of tobacco-related harm associated with intention to quit among cigarette smokers, E-Cigarette users, and dual users: findings from the US Population Assessment of Tobacco and Health (PATH) wave 1. Subst. Use Misuse 56 (4), 464–470. 10.1080/10826084.2021.1879145. [DOI] [PubMed] [Google Scholar]
- Lozano P, Arillo-Santillán E, Barrientos-Gutíerrez I, Shigematsu LMR, Thrasher JF, 2019a. E-cigarette social norms and risk perceptions among susceptible adolescents in a country that bans E-Cigarettes. Health Educ. Behav. Off Publ. Soc. Public Health Educ 46 (2), 275–285. 10.1177/1090198118818239. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lozano P, Santillán EA, Barrientos-Gutíerrez I, Zavala-Arciniega L, Shigematsu LMR, Thrasher JF, 2019b. E-cigarette use and it association with smoking reduction and cessation intentions among Mexican smokers. Salud. Publica Mex 61 (3), 276–285. 10.21149/9797. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Manning M, 2009. The effects of subjective norms on behaviour in the theory of planned behaviour: a meta-analysis. Br. J. Soc. Psychol 48 (4), 649–705. 10.1348/014466608X393136. [DOI] [PubMed] [Google Scholar]
- Mathew AR, Bhatt SP, Colangelo LA, et al. , 2019. Life-Course smoking trajectories and risk for emphysema in middle age: the CARDIA lung study. Am. J. Respir. Crit. Care Med 199 (2), 237–240. 10.1164/rccm.201808-1568LE. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McDermott MS, East KA, Hitchman SC, et al. , 2020. Social norms for e-cigarettes and smoking: associations with initiation of e-cigarette use, intentions to quit smoking and quit attempts: findings from the EUREST-PLUS ITC Europe Surveys. Eur. J. Public Health 30 (Suppl 3). 10.1093/eurpub/ckaa014 iii46–iii54. [DOI] [PMC free article] [PubMed] [Google Scholar]
- MMWR Morb Mortal Wkly Rep, 2023. QuickStats: Percentage Distribution of Cigarette Smoking Status Among Current Adult E-Cigarette Users, By Age Group — National Health Interview Survey, United States, 2021, 72. National Health Interview Survey, United States, p. 270. [DOI] [PMC free article] [PubMed] [Google Scholar]
- National Academies of Sciences E, Division H and M, Practice B on PH and PH, 2018. Toxicology of E-Cigarette Constituents. National Academies Press, US. Accessed January 27, 2021. https://www.ncbi.nlm.nih.gov/books/NBK507184/. [Google Scholar]
- Nohlert E,Öhrvik J, Tegelberg Å, Tillgren P, Helgason ÁR, 2013. Long-term follow-up of a high- and a low-intensity smoking cessation intervention in a dental setting–a randomized trial. BMC Public Health 13 (1), 592. 10.1186/1471-2458-13-592. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Piper ME, Baker TB, Benowitz NL, Kobinsky KH, Jorenby DE, 2019. Dual users compared to smokers: demographics, dependence, and biomarkers. Nicotine Tob. Res 21 (9), 1279–1284. 10.1093/ntr/nty231. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Piper ME, Baker TB, Benowitz NL, Jorenby DE, 2020. Changes in use patterns over 1 year among smokers and dual users of combustible and electronic cigarettes. Nicotine Tob. Res 22 (5), 672–680. 10.1093/ntr/ntz065. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Reddy KP, Schwamm E, Kalkhoran S, Noubary F, Walensky RP, Rigotti NA, 2021. Respiratory symptom incidence among people using electronic cigarettes, combustible tobacco, or both. Am. J. Respir. Crit. Care Med 204 (2), 231–234. 10.1164/rccm.202012-4441LE. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rivis A, Sheeran P, 2003. Descriptive norms as an additional predictor in the theory of planned behaviour: a meta-analysis. Curr. Psychol 22 (3), 218–233. 10.1007/s12144-003-1018-2. [DOI] [Google Scholar]
- Simonavicius E, McNeill A, Arnott D, Brose LS, 2017. What factors are associated with current smokers using or stopping e-cigarette use? Drug Alcohol Depend. 173, 139–143. 10.1016/j.drugalcdep.2017.01.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Smith KE, Ikegwuonu T, Weishaar H, Hilton S, 2021. Evidence use in E-cigarettes debates: scientific showdowns in a ‘wild west’ of research. BMC Public Health 21 (1), 362. 10.1186/s12889-021-10396-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Strong DR, Pearson J, Ehlke S, et al. , 2017. Indicators of dependence for different types of tobacco product users: descriptive findings from Wave 1 (2013–2014) of the Population Assessment of Tobacco and Health (PATH) study. Drug Alcohol Depend. 178, 257–266. 10.1016/j.drugalcdep.2017.05.010. [DOI] [PubMed] [Google Scholar]
- Sweet L, Brasky TM, Cooper S, et al. , 2019. Quitting behaviors among dual cigarette and E-Cigarette users and cigarette smokers enrolled in the tobacco user adult cohort. Nicotine Tob. Res 21 (3), 278–284. 10.1093/ntr/nty222. [DOI] [PMC free article] [PubMed] [Google Scholar]
- U.S. Food and Drug Administration. E-Cigarettes, Vapes, and other Electronic Nicotine Delivery Systems (ENDS). Published July 21, 2023. Accessed July 23, 2023. https://www.fda.gov/tobacco-products/products-ingredients-components/e-cigarettes-vapes-and-other-electronic-nicotine-delivery-systems-ends.
- United States Department Of Health And Human Services, 2016. Population Assessment of Tobacco and Health (PATH) Series. National Institutes Of Health. National Institute On Drug Abuse. 10.3886/SERIES606. Published online. [DOI] [Google Scholar]
- Xu Y, Guo Y, Liu K, Liu Z, Wang X, 2016. E-Cigarette awareness, use, and harm perception among adults: a meta-analysis of observational studies. PLoS ONE 11 (11), e0165938. 10.1371/journal.pone.0165938. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.