

Summary
Background
Intersectionality has rarely been considered in research studies of cognitive ageing. We investigated whether life-course financial mobility is differentially associated with later-life memory function and decline across intersectional identities defined by gender, and race and ethnicity.
Methods
Data were from two harmonised multiethnic cohorts (the Kaiser Healthy Aging and Diverse Life Experiences cohort and the Study of Healthy Aging in African Americans cohort) in northern California, USA (n=2340). Life-course financial mobility, measured using a combination of self-reported financial capital measures in childhood (from birth to age 16 years) and later adulthood (at the cohort baseline) was defined as consistently high, upwardly mobile, downwardly mobile, or consistently low. We clustered individuals into 32 strata representing intersectional identities defined by life-course financial mobility combined with gender, and race and ethnicity. Verbal episodic memory was assessed using the Spanish and English Neuropsychological Assessment Scales over four waves from 2017 to 2023. Adjusted mixed-effects linear regression models were estimated with and without fixed effects of gender, race and ethnicity, and financial mobility, to evaluate whether the random effects of the intersectional identity strata contributed variance to memory beyond individual fixed effects.
Findings
Mean age was 73·6 years (SD 8·1). Of 2340 individuals, 1460 (62·4%) were women, 880 (37·6%) were men, 388 (16·6%) were Asian, 1136 (48·5%) were Black, 334 (14·3%) were Latinx, and 482 (20·6%) were White. Consistently low and downwardly mobile financial capital were strongly negatively associated with later-life memory at baseline (−0·162 SD units [95% CI −0·273 to −0·051] for consistently low and −0·171 [−0·250 to −0·092] for downwardly mobile), but not rate of change over time. Intersectional identities contributed 0·2% of memory variance after accounting for the fixed effects of gender, race and ethnicity, and financial mobility.
Interpretation
Consistently low and downward life-course financial mobility are associated with lower later-life memory function. Intersectional identities defined by financial mobility in addition to gender, and race and ethnicity, contribute negligible additional variance to later-life memory in this study setting.
Funding
US National Institute on Aging, US National Institutes of Health.
Introduction
Positive socioeconomic trajectories across the life course, as indicated using markers of education, occupation, and income, are associated with better later-life cognitive outcomes.1–8 Improved socioeconomic standing could protect cognitive health through increased access to health care, opportunities for social engagement, and positive influence on lifestyle behaviours that are risk factors for dementia (eg, smoking, physical inactivity, and heavy alcohol use9,10). Improved financial standing could also allow individuals to improve their housing and nutrition, avoid exposure to environmental risks, and reduce the psychological stress associated with financial insecurity, all of which might be associated with later-life cognitive function and dementia risk.10–13 Despite the plausibility of these mechanisms, there is a paucity of research on financial mobility across the life course in relation to later-life cognitive outcomes, particularly in racially and ethnically diverse populations.
Evidence from more than 3000 Black and White adults in the Coronary Artery Risk Development in Young Adults Study in four cities in the USA shows that sustained poverty and income volatility over 20 years in midlife are associated with lower subsequent cognitive function.1,2 Evidence from the Kaiser Healthy Aging and Diverse Life Experiences Study(KHANDLE) in northern California, USA, shows that upward financial mobility and consistently high financial capital across the life course are positively associated with later-life cognitive function.14 These analyses assessed cognitive function at a single timepoint, and it is unknown whether life course financial mobility could bring differential returns to cognitive ageing trajectories across diverse social identities. Social identities can be classified using intersectionality, a theoretical framework that captures the multidimensional aspects of social identity that are used to advantage or disadvantage individuals in society.15,16 Intersectionality proposes that the health effects of sexism, racism, and other forms of so-called isms cannot be studied in isolation because they are not experienced in isolation.16
Resource substitution theory suggests that the association between life-course financial mobility and later-life cognitive health could vary by intersectional identities. According to resource substitution theory, health-promoting resources such as financial capital have greater influence for individuals with fewer alternative resources than for more advantaged individuals who have a greater number of alternative resources to draw upon.17,18 Applying resource substitution to intersectionality theory would suggest that women (who experience sexism) and minoritised racial and ethnic groups (who experience racism) could experience disproportionate later-life cognitive health risks with consistently low or downward life-course financial mobility compared with men and people racialized as White, because they might have fewer alternative resources to draw upon to protect their cognitive health as they age.
We thus aimed to investigate how life-course financial mobility might differentially be associated with later-life memory across population subgroups defined by gender and race and ethnicity, using data from two harmonised, multiethnic cohort studies. According to intersectionality and resource substitution theories, we hypothesised that older adults belonging to multiply disadvantaged groups (eg, women belonging to non-White racial or ethnic groups) could experience disproportionately greater later-life memory returns to upward financial mobility and disproportionately worse later-life memory returns to downward financial mobility than those belonging to less multiply disadvantaged groups.
Methods
Study design and participants
In this intersectional analysis, data were pooled from two harmonised longitudinal cohort studies of ageing: the KHANDLE cohort and the Study of Healthy Aging in African Americans (STAR) cohort. The KHANDLE and STAR studies were approved by the institutional review board at Kaiser Permanente Northern California (KPNC), CA, USA. All participants provided written informed consent.
The KHANDLE cohort includes community-dwelling older adults residing in the San Francisco Bay and Sacramento areas of California, USA. Individuals eligible for KHANDLE were long-term members of KPNC, an integrated health-care delivery system; were 65 years or older on Jan 1, 2017; spoke English or Spanish; and participated in at least one Kaiser Permanente multiphasic health check-up exam between 1964 and 1985. Stratified random sampling by race, ethnicity, and education was used with the goal of recruiting approximately equal proportions of Asian, Black, Latinx, and White participants and achieving diversity in educational attainment. Exclusion criteria included electronic medical record diagnosis of dementia or other neurodegenerative disease (frontotemporal dementia, Lewy body disease, Pick’s disease, Parkinson’s disease with dementia, and Huntington’s disease), or presence of health conditions that would impede participation in study interviews, including hospice activity in the past 12 months, history of severe chronic obstructive pulmonary disease in the past 6 months, congestive heart failure hospitalisations in the past 6 months, and history of end-stage renal disease or dialysis in the past 12 months. Wave one (baseline) KHANDLE study interviews occurred from April, 2017, to December, 2018. Follow-up study interviews occurred for three additional waves, approximately every 16–18 months since baseline: wave two interviews occurred from November, 2018, to May, 2020; wave three interviews occurred from June, 2020, to June, 2021; and wave four interviews occurred from February, 2022, to April, 2023. Study interviews were conducted in-person, with a shift to telephone interviewing during the COVID-19 pandemic.
The STAR cohort includes community-dwelling older Black adults residing in the San Francisco Bay area of California, USA. Individuals eligible for STAR were long-term members of KPNC; were 50 years or older on Jan 1, 2018; identified as Black or African American; and participated in at least one Kaiser Permanente multiphasic health checkup exam between 1964 and 1985. Sampling was randomly stratified by age and educational attainment to recruit approximately equal proportions of participants aged 50–64 years and participants 65 years and older. Exclusion criteria were the same as for the KHANDLE cohort. Wave one (baseline) STAR interviews occurred from November, 2017, to March, 2020. Follow-up study interviews occurred for two additional waves, approximately every 13–14 months since baseline: wave two interviews occurred from March, 2019, to August, 2020, and wave three interviews occurred from August, 2020, to November, 2021. As with the KHANDLE cohort, study interviews were conducted in-person, with a shift to telephone interviewing during the COVID-19 pandemic.
Exposure
The exposure variable was the combined intersectional strata of gender (female or male), race and ethnicity (White, Black, Latinx, or Asian), both self-reported at the baseline study interview, and life-course financial mobility. Gender responses were supplemented with electronic medical record data (ie, recorded by physicians) when self-reported data were unavailable. We refer to gender throughout, recognising that this variable captures both the biological aspects of sex and sociological aspects of gender.19 Life-course financial mobility was defined according to Peterson and colleagues,14 as four categories representing the combination of self-reported financial capital measures in childhood (from birth to age 16 years) and later adulthood (at the cohort baseline) as consistently high (high in childhood and later adulthood), upwardly mobile (low in childhood and high in later adulthood), downwardly mobile (high in childhood and low in later adulthood), and consistently low (low in childhood and later adulthood). Childhood financial capital was considered as low if the participant reported either criteria: (1) ever having to go hungry in childhood due to financial circumstances or (2) having family finances in childhood that were poor relative to others and having parents who did not own their childhood home. Later adulthood financial capital was considered as low if the participant reported any of the following criteria at the study baseline: received supplemental security income or state or county welfare; received financial assistance from friends or family; had an annual household income of US$55000 or less; or was often worried about having enough money to pay for living expenses and had an annual household income of $75000 or less. The combination of all possible categories of these three variables resulted in 32 strata representing intersectional identities of gender, race and ethnicity, and life-course financial mobility.
Outcome
Verbal episodic memory was selected as the outcome due to its clinical relevance with a high sensitivity to ageing-related change and as a hallmark early cognitive symptom of dementia.20 Verbal episodic memory was assessed at all waves of both the KHANDLE and STAR cohorts using the Spanish and English Neuropsychological Assessment Scales.21 Participants were assessed in their preferred language of Spanish or English. The verbal episodic memory scores were derived from a multitrial word-list learning test and standardised to the baseline distribution of the pooled cohort, which was standardised to have a mean of zero and an SD of one.
Covariates
Potential common causes of life-course financial mobility and later-life memory ageing were selected as model covariates:baseline age (continuous and mean-centred), country of birth (USA or outside USA), maternal education (high school or less, some college or Associate’s degree, Bachelor’s degree or higher, or missing or not applicable), and paternal education (high school or less, some college or Associate’s degree, Bachelor’s degree or higher, or missing or not applicable). Educational attainment (grade school; some high school; technical or trade school; some college; college degree; graduate school; high school or general educational development) was included to describe the sample and in a sensitivity analysis to evaluate the role of education in the link between financial mobility and later-life memory.
Statistical analysis
Characteristics of the sample were described using univariate statistics, overall and by cohort. This analysis uses the technique of multilevel analysis of individual heterogeneity and discriminatory accuracy (MAIHDA22,23). MAIHDA incorporates intersectionality theory into statistical modelling through multilevel models with random effects representing intersectional identity group strata. In this MAIHDA analysis, individuals were grouped into 32 strata defined by all possible combinations of the gender, race and ethnicity, and life-course financial mobility variables. Three-level linear multilevel regression models with random intercepts and slopes and time since baseline as the timescale (in calendar years) were estimated using restricted maximum likelihood estimation. Verbal episodic memory observations at level 1 were clustered within persons at level 2 and intersectional identity strata at level 3. We first estimated a null model including random effects for individuals and for intersectional identity strata alongside fixed covariate effects of age at baseline, mother’s education, father’s education, and country of birth. We assessed statistical interactions between these fixed covariate effects and time since baseline, in addition to a quadratic term for time, retaining only the age at baseline by time interaction because the rest of the interactions were not statistically significant. Next, we estimated a main-effects model, with the additional inclusion of fixed effects for gender, race and ethnicity, and life-course financial mobility. We evaluated each of their interactions with time since baseline, which were not statistically significant and thus not included in the model. This main-effects model allows for the estimation of the extent to which the observed memory intercepts and slopes differ from expected based on the fixed effects of each individual component comprising the intersectional strata.22 Hence, the stratum-level random intercept and slope and the proportion of variance in memory that they explain, indicated by the variance partition coefficient, are the model parameters of interest in the MAIHDA approach.23 The full model specifications are presented in the appendix (p 2).
All models were additionally adjusted for mode of study interview (in-person vs telephone) to account for the shift from in-person to telephone interviewing during the COVID-19 pandemic. We accounted for practice effects in memory testing in the KHANDLE cohort using a previously described approach.24 Practice effects are a phenomenon that occurs in cognitive testing when test scores improve after repeated cognitive test administration due to practice taking the tests, rather than real cognitive change.24 All analyses were conducted using Stata/SE, version 18.0, with p<0·05 indicating statistical significance.
We conducted three sensitivity analyses to evaluate the robustness of our results. In the first, we restricted the sample to individuals born in the USA only. In the second, we evaluated the effect of adjusting for educational attainment on our results. In the third, we re-ran our main effects model stratified by cohort, but without the random effects for intersectional identity strata, to evaluate whether the fixed effect of life-course financial mobility varied by cohort.
Role of the funding source
The funder of the study had no role in study design, data collection, data analysis, data interpretation, or writing of the report.
Results
At baseline, 1712 individuals were enrolled in KHANDLE and 764 were enrolled in STAR. At of the time of data analysis in November, 2023, data collection for KHANDLE wave four was ongoing, with 493 observations collected through April, 2023, being available. STAR has completed three data collection waves. A total of 2340 individuals (95% of those who were eligible for the current analysis) with a total of 6616 memory observations across waves were included in the analysis (appendix pp 3–4).
Mean age of the sample at baseline was 73·6 years (SD 8·1). Of the 2340 individuals in the sample, 1460 (62·4%) were women and 880 (37·6%) were men. 388 (16·6%) individuals identified as Asian, 1136 (48·5%) as Black, 334 (14·3%) as Latinx, and 482 (20·6%) as White (table 1). Age distribution by race and ethnicity is shown in the appendix (p 5). Of 2340 individuals, 1094 (46·8%) experienced consistently high financial capital from childhood to late adulthood, whereas 330 (14·1%) experienced upward financial mobility, 654 (27·9%) experienced downward financial mobility, and 262 (11·2%) experienced consistently low financial capital from childhood to late adulthood (table 1). When combined into intersectional identity strata, the most frequent stratum was Black women with consistently high financial capital(n=303) and the least frequent stratum was White men with consistently low financial capital (n=11; appendix p 6).
Table 1:
Baseline characteristics of the KHANDLE and STAR cohorts
| Total (n=2340) | KHANDLE (n=1615) | STAR (n=725) | |
|---|---|---|---|
|
| |||
| Age, years | 73·6 (8·1, 53–89) | 75·9 (6·6, 65–89) | 68·5 (8·7, 53–89) |
| Gender | |||
| Man | 880 (37·6%) | 657 (40·7%) | 223 (30·8%) |
| Woman | 1460 (62·4%) | 958 (59·3%) | 502 (69·2%) |
| Race and ethnicity | |||
| Asian | 388 (16·6%) | 388 (24·0%) | 0 |
| Black | 1136 (48·5%) | 417 (25·8%) | 719 (99·2%) |
| Latinx | 334 (14·3%) | 328 (20·3%) | 6 (0·8%) |
| White | 482 (20·6%) | 482 (29·8%) | 0 |
| Life-course financial mobility | |||
| Consistently high | 1094 (46·8%) | 760 (47·1%) | 334 (46·1%) |
| Upwardly mobile | 330 (14·1%) | 234 (14·5%) | 96 (13·2%) |
| Downwardly mobile | 654 (27·9%) | 427 (26·4%) | 227 (31·3%) |
| Consistently low | 262 (11·2%) | 194 (12·0%) | 68 (9·4%) |
| Mother's education | |||
| High school or less | 1465 (62·6%) | 1038 (64·3%) | 427 (58·9%) |
| Some college or an Associate's degree | 308 (13·2%) | 181 (11·2%) | 127 (17·5%) |
| Bachelor's degree or higher | 240 (10·3%) | 154 (9·5%) | 86 (11·9%) |
| Missing or not applicable | 327 (13·9%) | 242 (15·0%) | 85 (11·7%) |
| Father's education | |||
| High school or less | 1250 (53·4%) | 831 (51·5%) | 419 (57·8%) |
| Some college or an Associate's degree | 236 (10·1%) | 160 (9·9%) | 76 (10·5%) |
| Bachelor's degree or higher | 319 (13·6%) | 248 (15·4%) | 71 (9·8%) |
| Missing or not applicable | 535 (22·9%) | 376 (23·3%) | 159 (21·9%) |
| Country of birth | |||
| USA | 1933 (82·6%) | 1219 (75·5%) | 714 (98·5%) |
| Elsewhere | 407 (17·4%) | 396 (24·5%) | 11 (1·5%) |
| Educational attainment | |||
| Grade school | 47 (2·0%) | 45 (2·8%) | 2 (0·3%) |
| Some high school | 73 (3·1%) | 59 (3·7%) | 14 (1·9%) |
| Technical or trade school | 102 (4·4%) | 74 (4·6%) | 28 (3·9%) |
| Some college | 810 (34·6%) | 493 (30·5%) | 317 (43·7%) |
| College degree | 536 (22·9%) | 406 (25·1%) | 130 (17·9%) |
| Graduate school | 505 (21·6%) | 374 (23·2%) | 131 (18·1%) |
| High school or General Equivalency Diploma | 267 (11·4%) | 164 (10·2%) | 103 (14·2%) |
Data are n (%) or mean (SD, range). Both cohorts draw from the same sampling frame of community-dwelling, long-term members of Kaiser Permanente Northern California, an integrated health-care delivery system in northern California, USA. Eligibility for KHANDLE and STAR varied based on age and race and ethnicity, as seen in the demographic differences. Individuals were assessed for verbal episodic memory from 2017 to 2023. KHANDLE=Kaiser Healthy Aging and Diverse Life Experiences. STAR=Study of Healthy Aging in African Americans.
In the null model, with repeated outcomes of verbal episodic memory (level 1) clustered within individuals (level 2) and within intersectional identity strata defined by gender, race and ethnicity, and life-course financial mobility (level3), the random intercept estimate for the intersectional identity clusters was 0·105 (95% CI 0·060–0·186), corresponding to 12% of the total variance in verbal episodic memory (table 2). The random intercept estimate for individuals was 0·451 (0·407–0·499), corresponding to 63% of the total variance in verbal episodic memory (table 2). Differences between intersectional identity strata and between persons contributed little variance to the random slopes (table 2).
Table 2:
Parameter estimates from multilevel models of verbal episodic memory of the KHANDLE and STAR cohorts
| Null model, coefficient (95% CI) | Main-effects model, coefficient (95% CI) | |
|---|---|---|
|
| ||
| Fixed effects | ||
| Intercept | 0·019 (−0·101 to 0·148) | −0·041 (−0·151 to 0·069) |
| Baseline age (continuous), years | −0·044 (−0·049 to −0·039) | −0·045 (−0·049 to −0·040) |
| Gender | ||
| Man (ref) | .. | .. |
| Woman | .. | 0·591 (0·524 to 0·659) |
| Race and ethnicity | ||
| Asian (ref) | .. | .. |
| Black | .. | −0·371 (−0·476 to −0·265) |
| Latinx | .. | −0·170 (−0·286 to −0·054) |
| White | .. | −0·062 (−0·172, 0·048) |
| Life-course financial mobility | ||
| Consistently high (ref) | .. | .. |
| Upwardly mobile | .. | −0·045 (−0·143 to 0·052) |
| Downwardly mobile | .. | −0·171 (−0·250 to −0·092) |
| Consistently low | .. | −0·162 (−0·273 to −0·051) |
| Time since baseline (continuous), years | −0·039 (−0·064 to −0·014) | −0·040 (−0·065 to −0·015) |
| Time by baseline age interaction | −0·003 (−0·005 to −0·001) | −0·003 (−0·005 to −0·001) |
| Random intercepts | ||
| Intersectional strata-level | 0·105 (0·060 to 0·186) | 0·001 (0·000 to 0·060) |
| Person-level | 0·451 (0·407 to 0·499) | 0·450 (0·407 to 0·497) |
| Random slopes | ||
| Intersectional strata-level | 0·000 (0·000 to 0·008) | 0·000 (0·000 to 0·006) |
| Person-level | 0·015 (0·008 to 0·026) | 0·015 (0·008 to 0·026) |
| VPC | ||
| Intersectional strata-level, % | 12% | 0·2% |
| Person-level, % | 63% | 58% |
The null and main-effects models are additionally adjusted for age at baseline, mother's education, father’s education, country of birth, and mode of interview. The VPC indicates the proportion of baseline memory variance attributable to differences between intersectional identity strata and differences between persons. VPC=variance partition coefficient.
In the main effects model, which additionally includes fixed effects for gender, race and ethnicity, and life-course financial mobility, the random intercept estimate for the intersectional identity clusters decreased to 0·001 (95% CI 0·000–0·060), corresponding to 0·2% of the total variance in verbal episodic memory (table 2). The random intercept estimate for individuals was similar to the estimate from the null model, at 0·450 (0·407–0·497), corresponding to 58% of the total variance in verbal episodic memory (table 2). As in the null model, differences between intersectional identity strata and individuals contributed little variance to the random slopes (table 2).
Visualising the decomposition in memory variance, shows that the majority of variance in memory was attributable to differences across waves and between individuals, rather than differences between intersectional identity strata (figure 1).
Figure 1: Decomposition in memory variance.
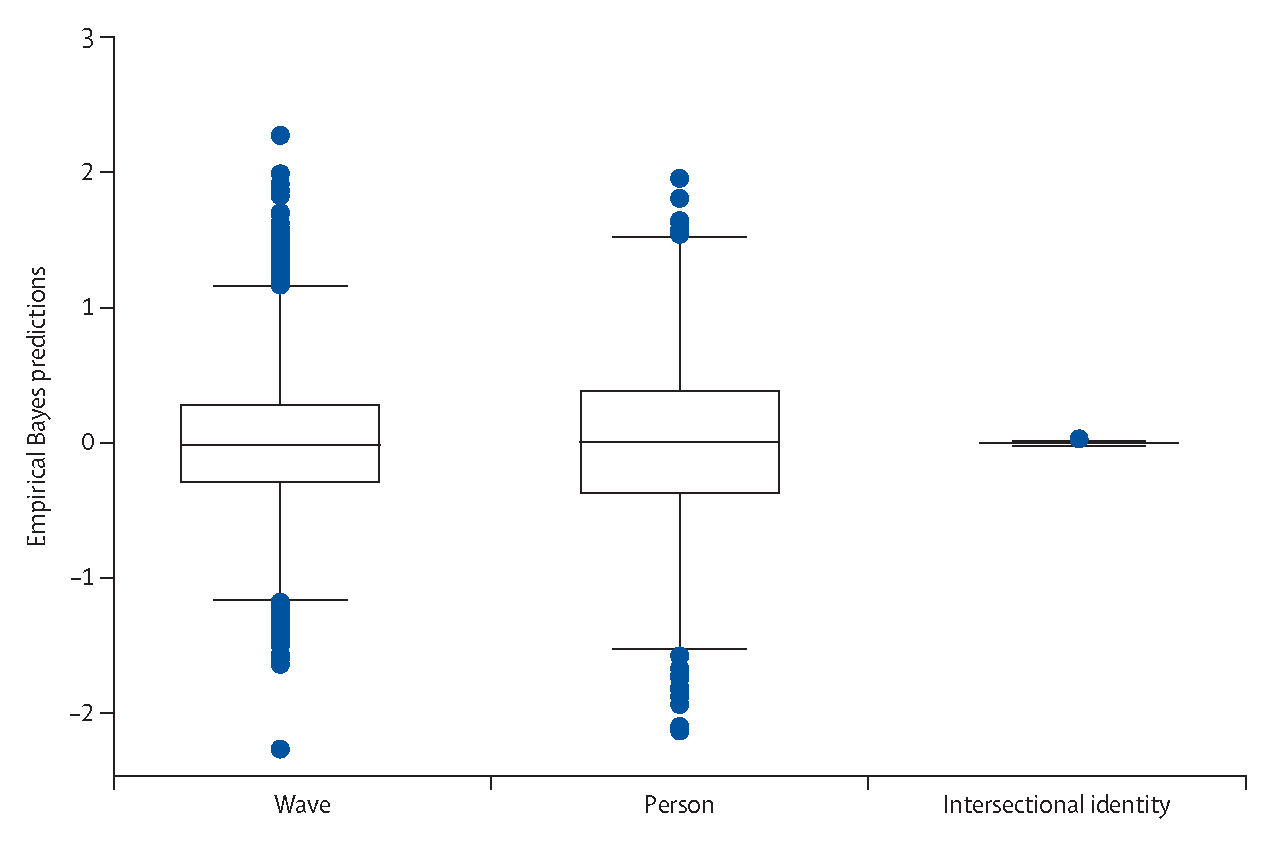
Box plots of empirical Bayes predictions for random intercepts at the wave-level (level 1), person-level (level 2), and intersectional identity-level (level 3), after accounting for early-life confounders (age at baseline, mother’s education, father’s education, and country of birth) and the individual fixed effects comprising the intersectional identity strata (gender, race and ethnicity, and life-course financial mobility).
Individuals with consistently low or downwardly mobile financial capital had lower mean verbal episodic memory scores at baseline than those with consistently high life-course financial capital (−0·162 SD units [95% CI −0·273 to −0·051] for consistently low financial capital and −0·171[−0·250 to −0·092] for downwardly mobile financial capital; table 2). These were strong magnitudes of association, equivalent to 4·1 times and 4·3 times the estimate for one year of chronological ageing (−0·040 SD units), respectively, for low and downwardly mobile financial capital. The person-specific memory intercepts and slopes according to each of the 32 intersectional identity strata illustrate heterogeneity in memory scores across individuals within each strata (figure 2).
Figure 2: Predicted person-specific longitudinal trajectories of verbal episodic memory scores by intersectional identities defined according to strata of gender, race and ethnicity, and life-course financial mobility.
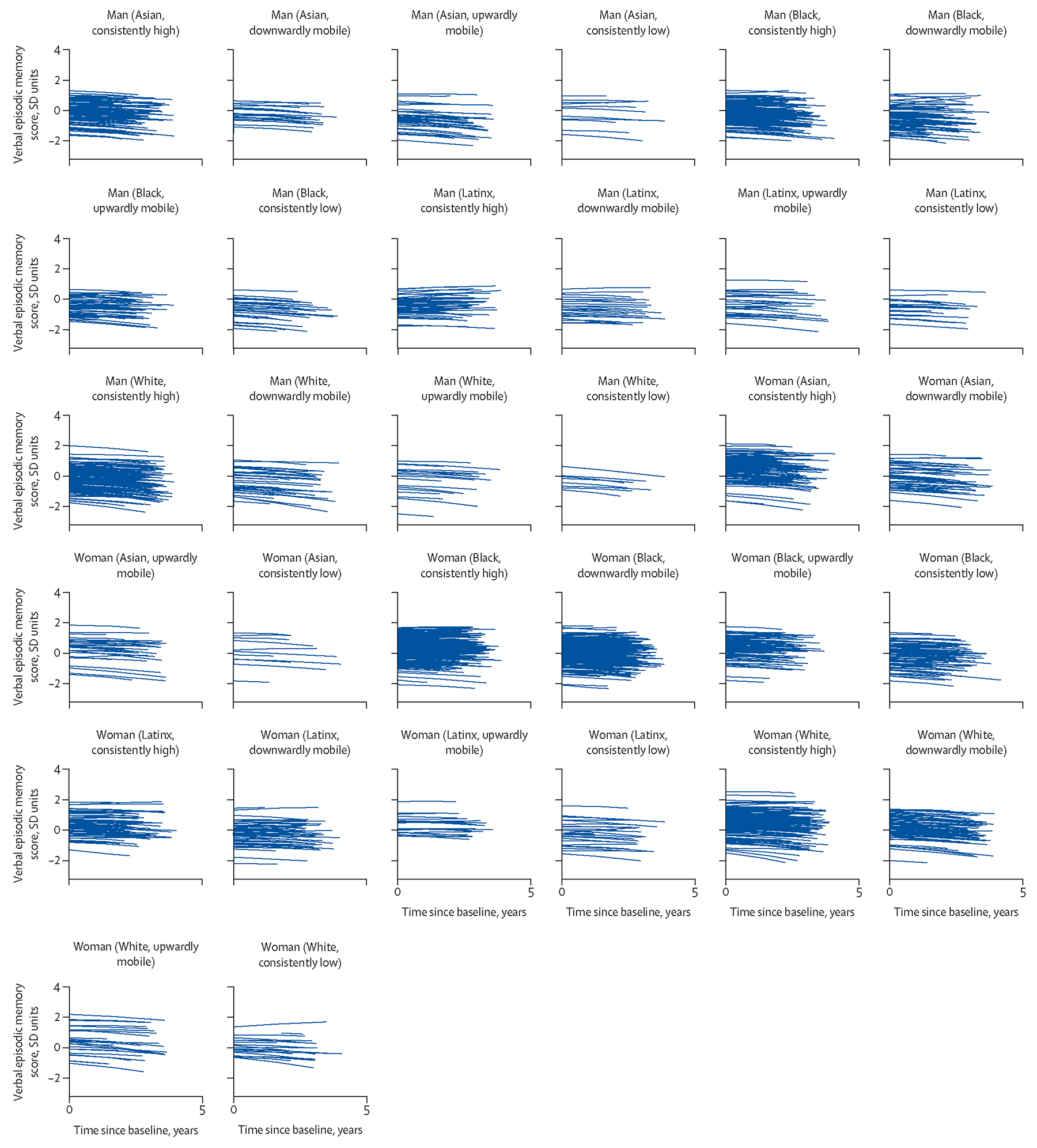
The model predictions represent a hypothetical person aged 73·6 years with mother’s education of high school or less, father’s education of high school or less, and who was born in the USA (ie, the reference values of model covariates). The density of trajectories within each subplot corresponds to the sample size within each stratum (range 33–839; appendix p 6).
Results from the sensitivity analyses were consistent with the main analysis when restricted to individuals born in the USA only (appendix p 7). When educational attainment was added to the models, the random effects estimates were consistent with the original analysis. The associations between downwardly and upwardly mobile financial capital and memory were also consistent with the main analysis, although the association between consistently low life-course financial capital and memory was attenuated (appendix p 8). Individuals with consistently high or upwardly mobile financial capital were more likely to hold a college or graduate degree than those with downwardly mobile or consistently low financial capital (appendix p 8). Results for the fixed effect of financial mobility were consistent with the main analysis when models were stratified by cohort (appendix p 9).
Discussion
In this intersectional analysis of two multiethnic longitudinal cohort studies, we found that consistently low financial capital and downward financial mobility across the life course were negatively associated with memory function, but not rate of memory change over time. The magnitudes of these associations were strong, equivalent to approximately 4·1 to 4·3 years of ageing, and they were consistent across intersectional identities defined by gender, and by race and ethnicity. Although inconsistent with intersectionality and resource substitution theories, this finding indicates that the intersection of gender with race and ethnicity in this study setting did not confer differential associations between life-course financial mobility and later-life memory. These results should be confirmed in other study settings and populations, and according to other socioeconomic measures and aspects of social identity.
Our results are consistent with literature indicating that disadvantaged socioeconomic conditions across the life course are associated with worse cognitive ageing outcomes.1–8,14 Our estimate for downwardly mobile financial capital was strong and in the negative direction, consistent with findings in similar studies.1,2,6,8 This finding was independent of education, whereas education appeared to explain the association between consistently low financial capital and worse later-life memory. Thus, education could be a partial mechanism for the link between life-course financial mobility and later-life memory. Our observed lack of association between financial mobility and rate of memory change over time is consistent with studies that also observe a range of socioeconomic exposures to be related to memory at baseline, but not over time.25–27 Socioeconomic exposures across the life course may play a larger role in shaping initial memory status in mid-to-later life than rate of decline over time. Our analysis should be replicated within the KHANDLE and STAR cohorts in the future to evaluate if our findings hold with a longer follow-up time. Our results are inconsistent with previous MAIHDA studies that have identified inequities in the outcomes of BMI and birthweight according to intersections of gender with race and ethnicity and other sociodemographic factors such as age and nativity among US adults,22,28 but consistent with MAIHDA analyses identifying no intersectional inequities in the risk of chronic obstructive pulmonary disease among middle-aged and older Swedish adults29 and depression among adolescents and young adults in the USA.30 Our study is the first, to our knowledge, to apply an intersectionality approach to investigate inequities in a cognitive ageing outcome. Intersectional health inequities could vary by health outcome and according to contextual differences across populations, such as levels of structural discrimination, social policies, and access to health care. Cross-population research might help to elucidate contextual factors that can modify intersectional health inequities.
An important methodological consideration in this study is that it consisted of long-term members of an integrated health-care delivery system in northern California, USA. This is a segment of the population that had consistent access to high-quality health insurance, most often through their own employment or a spouse’s employment. The experiences of this sample might not reflect those of the broader general population, in California or elsewhere. We might not have observed an intersectional effect in this sample, despite its racial and ethnic diversity, due to the relative socioeconomic advantages experienced by much of the sample regardless of race and ethnicity, including long-term access to health care. Additionally, given the heterogeneity with the Asian and Latinx groups in our sample, it is possible that our clustering of these groups masked additional differences within these groups.
Other limitations include that our measures of financial capital were retrospective and self-reported and could be subject to non-differential measurement error or differential recall bias if the accuracy of recall systematically varied by baseline memory status. Excluded individuals had lower baseline memory scores than those included in the study. Our results could therefore underestimate the true magnitudes of associations, if excluded individuals were also more likely to have consistently low or downwardly mobile financial mobility. In addition, the precision of the estimated memory slopes might be lower for STAR participants than KHANDLE participants, because the STAR cohort had three waves of memory observations whereas the KHANDLE cohort had four. Finally, although we accounted for early-life confounders as best possible, there can still be residual confounding by unmeasured early-life determinants of life course financial mobility and later-life memory.
Strengths of this study include its longitudinal design, large sample size, representation of older adults from multiple racial and ethnic groups, validated measures of verbal episodic memory in English and Spanish, robust accounting for practice effects in cognitive testing, and a theoretically informed approach to testing intersectionality theory as applied to memory ageing. The theoretical rationale supporting intersectionality theory is strong and has been shown to apply to other health outcomes. Future studies should apply an intersectionality approach to understanding how socioeconomic conditions could be associated with cognitive outcomes in other populations and settings. Future intersectionality studies should also incorporate direct measures of discrimination, which we did not include here.
In conclusion, low financial capital and downward financial mobilities across the life course were associated with lower baseline memory function, but not rate of memory decline over time, in this longitudinal multiethnic cohort of older adults. There was no unique effect of the intersections of gender, race and ethnicity, and life-course financial mobility on later-life memory in this study. Future studies should investigate these associations in other populations and settings, and according to other aspects of socioeconomic conditions and social identities.
Supplementary Material
Research in context.
Evidence before this study
Before undertaking this study, we systematically searched PubMed and Google Scholar databases to identify scientific articles reporting on socioeconomic trajectories across the life course in relation to later-life cognitive outcomes, including cognitive function, cognitive decline, and dementia. This search was initially conducted in May, 2022, and updated in February, 2024. Eligible articles reported on cross-sectional or longitudinal population-based studies of adults with neuropsychological cognitive assessments. Search terms for the exposure included “economic”, “socioeconomic”, “income”, “financial”, and “wealth”, and each of these terms combined with each of “status”, “mobility”, and “trajectories”. Search terms for the outcome included “cognition”, “cognitive”, “memory”, and each of the latter two terms combined with “status”, “outcomes”, “function”, “performance”, “decline”, and “aging”. Exposure and outcome search terms were linked with the “AND” operator. Relevant evidence finds that positive socioeconomic trajectories across the life course in addition to higher socioeconomic position measured at single points in time are associated with better later-life cognitive outcomes. Few studies examined financial mobility as the socioeconomic marker of interest, and none examined whether socioeconomic trajectories across the life course were differentially associated with later-life cognitive outcomes according to intersectional identities defined by gender, and race and ethnicity.
Added value of this study
To our knowledge, this study is the first to apply an intersectionality approach to investigate inequities in memory ageing in a multiethnic cohort study. We use a longitudinal approach to the multilevel analysis of individual heterogeneity and discriminatory accuracy (MAIHDA), which has not previously been applied to the study of cognitive ageing. MAIHDA formally incorporates intersectionality theory into statistical modelling, with many potential future applications beyond the present study. We found consistently low and downward life-course financial mobility are associated with lower later-life memory function. These associations were strong in magnitude, equivalent to approximately 4·1 to 4·3 years of chronological ageing, and they were consistent across intersectional identities defined by gender, and race and ethnicity.
Implications of all the available evidence
Our findings align with literature indicating that disadvantaged socioeconomic conditions across the life course are associated with worse cognitive ageing outcomes. Intersectional inequities in cognitive ageing in other populations and settings should be investigated further in future studies.
Acknowledgments
This work was supported by funding from the US National Institutes of Aging at the US National Institutes of Health (grant numbers: R01AG052132, R01AG050782, and R13AG030995).
Footnotes
Declaration of interests
PG and LCK report funding from the US National Institute on Aging at the US National Institutes of Health. ERM reports funding from the US National Institute on Aging at the US National Institutes of Health and the California Department of Public Health, consulting fees from consulting on grants funded by the US National Institutes of Health, honoraria for research talks at Columbia University and the XVII Symposium on Sleep and Breathing, and serving on the leadership committees for the Methods in Longitudinal Research on Dementia (MELODEM) Initiative and the Advanced Psychometrics Methods in Cognitive Aging Conference. RLP reports funding from the US National Institute on Aging at the US National Institutes of Health, honorarium for a symposium presentation at the University of California Davis Alzheimer’s Disease Research Center, and travel support from the Alzheimer’s Association Interdisciplinary Summer Research Institute. CES reports funding from the US National Institute on Aging at the US National Institutes of Health and serving as chair of the ISTAART PIA to Elevate Early Career Researchers (PEERs) and co-chair of the Sex and Gender Special Interest Group of the Diversity and Disparities PIA in ISTAART. RAW reports funding from the US National Institutes of Health and the Alzheimer’s Association, consulting fees from the University of Colorado and Genentech Pan Neuro, and serving on the Observational Monitoring Board for the Efficacy and Durability of Initial Combination Therapy for Type 2 Diabetes (EDICT) study and the Diabetes Prevention Program Outcomes Study (DPPOS), and the Data Monitoring Committee of the Add Health Study. XY, JA-R, PAA-H, CV-C, and EM declare no competing interests.
Contributor Information
Lindsay C Kobayashi, Center for Social Epidemiology and Population Health, Department of Epidemiology, University of Michigan, MI, USA.
Rachel L Peterson, School of Public and Community Health Sciences, University of Montana, Missoula, MT, USA.
Xuexin Yu, Center for Social Epidemiology and Population Health, Department of Epidemiology, University of Michigan, MI, USA.
Justina Avila-Rieger, Taub Institute for Research in Aging and Alzheimer’s Disease, Columbia University, New York, NY, USA.
Priscilla A Amofa-Ho, Department of Clinical and Health Psychology, University of Florida, Gainesville, FL, USA.
Clara Vila-Castelar, Massachusetts General Hospital, Harvard Medical School, Boston, MA, USA.
Erika Meza, Harvard Center for Population and Development Studies, Harvard T H Chan School of Public Health, MA, USA.
C Elizabeth Shaaban, Alzheimer’s Disease Research Center and Department of Epidemiology, University of Pittsburgh, Pittsburgh, PA, USA.
Rachel A Whitmer, Departments of Public Health Sciences and Neurology, University of California, Davis, CA, USA.
Paola Gilsanz, Kaiser Permanente Northern California Division of Research, Oakland, CA, USA.
Elizabeth Rose Mayeda, Department of Epidemiology, University of California, Davis, CA, USA.
Data sharing
De-identified individual participant data used in this analysis can be accessed by submitting a paper proposal form online (https://sites.google.com/g.ucla.edu/khandle-study-site/project-proposals-new-data-userregistration). Researchers who submit a methodologically sound proposal that does not substantially overlap with existing projects, unless the goal is replication, will be granted secure access to de-identified data and data dictionaries upon approval of their research proposal and completion of a data use agreement. Analytic code for the present analysis is available online (https://github.com/SEGA-UM/Intersectionality).
References
- 1.Grasset L, Glymour MM, Elfassy T, et al. Relation between 20-year income volatility and brain health in midlife: The CARDIA study. Neurology 2019; 93: e1890–99. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Zeki Al Hazzouri A, Elfassy T, Sidney S, Jacobs D, Pérez Stable EJ, Yaffe K. Sustained economic hardship and cognitive function: the coronary artery risk development in young adults study. Am J Prev Med 2017; 52: 1–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Zeki Al Hazzouri A, Haan MN, Kalbfleisch JD, Galea S, Lisabeth LD, Aiello AE. Life-course socioeconomic position and incidence of dementia and cognitive impairment without dementia in older Mexican Americans: results from the Sacramento area Latino study on aging. Am J Epidemiol 2011; 173: 1148–58. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Horvat P, Richards M, Malyutina S, et al. Life course socioeconomic position and mid-late life cognitive function in Eastern Europe. J Gerontol B Psychol Sci Soc Sci 2014; 69: 470–81. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Singh-Manoux A, Richards M, Marmot M. Socioeconomic position across the lifecourse: how does it relate to cognitive function in mid-life? Ann Epidemiol 2005; 15: 572–78. [DOI] [PubMed] [Google Scholar]
- 6.Marden JR, Tchetgen Tchetgen EJ, Kawachi I, Glymour MM. Contribution of socioeconomic status at 3 life-course periods to late-life memory function and decline: early and late predictors of dementia risk. Am J Epidemiol 2017; 186: 805–14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Mayeda ER, Mobley TM, Weiss RE, Murchland AR, Berkman LF, Sabbath EL. Association of work-family experience with mid- and late-life memory decline in US women. Neurology 2020; 95: e3072–80. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Kobayashi LC, Feldman JM. Employment trajectories in midlife and cognitive performance in later life: longitudinal study of older American men and women. J Epidemiol Community Health 2019; 73: 232–38. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Deckers K, Cadar D, van Boxtel MPJ, Verhey FRJ, Steptoe A, Köhler S. Modifiable risk factors explain socioeconomic inequalities in dementia risk: evidence from a population-based prospective cohort study. J Alzheimers Dis 2019; 71: 549–57. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Livingston G, Huntley J, Sommerlad A, et al. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. Lancet 2020; 396: 413–46. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Franks KH, Bransby L, Saling MM, Pase MP. Association of stress with risk of dementia and mild cognitive impairment: a systematic review and meta-analysis. J Alzheimers Dis 2021; 82: 1573–90. [DOI] [PubMed] [Google Scholar]
- 12.McMichael AJ, McGuinness B, Lee J, Minh HV, Woodside JV, McEvoy CT. Food insecurity and brain health in adults: a systematic review. Crit Rev Food Sci Nutr 2022; 62: 8728–43. [DOI] [PubMed] [Google Scholar]
- 13.Killin LOJ, Starr JM, Shiue IJ, Russ TC. Environmental risk factors for dementia: a systematic review. BMC Geriatr 2016; 16: 175. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Peterson RL, George KM, Gilsanz P, et al. Lifecourse socioeconomic changes and late-life cognition in a cohort of U.S.-born and U.S. immigrants: findings from the KHANDLE study. BMC Public Health 2021; 21: 920. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Hancock AM. Empirical intersectionality: a tale of two approaches. UC Irvine Law Rev 2013; 3: 259. [Google Scholar]
- 16.Agénor M Future Directions for incorporating intersectionality into quantitative population health research. Am J Public Health 2020; 110: 803–06. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Ross CE, Mirowsky J. Sex differences in the effect of education on depression: resource multiplication or resource substitution? Soc Sci Med 2006; 63: 1400–13. [DOI] [PubMed] [Google Scholar]
- 18.Ross CE, Mirowsky J. Gender and the health benefits of education. Sociol Q 2010; 51: 1–19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Mielke MM, Aggarwal NT, Vila-Castelar C, et al. Consideration of sex and gender in Alzheimer’s disease and related disorders from a global perspective. Alzheimers Dement 2022; 18: 2707–24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Hernandez Saucedo H, Whitmer RA, Glymour M, et al. Measuring cognitive health in ethnically diverse older adults. J Gerontol B Psychol Sci Soc Sci 2022; 77: 261–71. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Mungas D, Reed BR, Crane PK, Haan MN, González H. Spanish and English Neuropsychological Assessment Scales (SENAS): further development and psychometric characteristics. Psychol Assess 2004; 16: 347–59. [DOI] [PubMed] [Google Scholar]
- 22.Evans CR, Williams DR, Onnela JP, Subramanian SV. A multilevel approach to modeling health inequalities at the intersection of multiple social identities. Soc Sci Med 2018; 203: 64–73. [DOI] [PubMed] [Google Scholar]
- 23.Merlo J Multilevel analysis of individual heterogeneity and discriminatory accuracy (MAIHDA) within an intersectional framework. Soc Sci Med 2018; 203: 74–80. [DOI] [PubMed] [Google Scholar]
- 24.Chen R, Calmasini C, Swinnerton K, et al. Pragmatic approaches to handling practice effects in longitudinal cognitive aging research. Alzheimers Dement 2023; 19: 4028–36. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Soh Y, Eng CW, Mayeda ER, et al. Association of primary lifetime occupational cognitive complexity and cognitive decline in a diverse cohort: results from the KHANDLE study. Alzheimers Dement 2023; 19: 3926–35. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Yu X, Langa KM, Cho TC, Kobayashi LC. Association of perceived job insecurity with subsequent memory function and decline among adults 55 years or older in England and the US, 2006 to 2016. JAMA Netw Open 2022; 5: e227060. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Zahodne LB, Glymour MM, Sparks C, et al. Education does not slow cognitive decline with aging: 12-year evidence from the Victoria Longitudinal Study. J Int Neuropsychol Soc 2011; 17: 1039–46. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Evans CR, Nieves CI, Erickson N, Borrell LN. Intersectional inequities in the birthweight gap between twin and singleton births: a random effects MAIHDA analysis of 2012–2018 New York City birth data. Soc Sci Med 2023; 331: 116063. [DOI] [PubMed] [Google Scholar]
- 29.Axelsson Fisk S, Mulinari S, Wemrell M, Leckie G, Perez Vicente R, Merlo J. Chronic obstructive pulmonary disease in Sweden: an intersectional multilevel analysis of individual heterogeneity and discriminatory accuracy. SSM Popul Health 2018; 4: 334–46. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Evans CR, Erickson N. Intersectionality and depression in adolescence and early adulthood: a MAIHDA analysis of the national longitudinal study of adolescent to adult health, 1995–2008. Soc Sci Med 2019; 220: 1–11. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
De-identified individual participant data used in this analysis can be accessed by submitting a paper proposal form online (https://sites.google.com/g.ucla.edu/khandle-study-site/project-proposals-new-data-userregistration). Researchers who submit a methodologically sound proposal that does not substantially overlap with existing projects, unless the goal is replication, will be granted secure access to de-identified data and data dictionaries upon approval of their research proposal and completion of a data use agreement. Analytic code for the present analysis is available online (https://github.com/SEGA-UM/Intersectionality).