
Fig. 1.
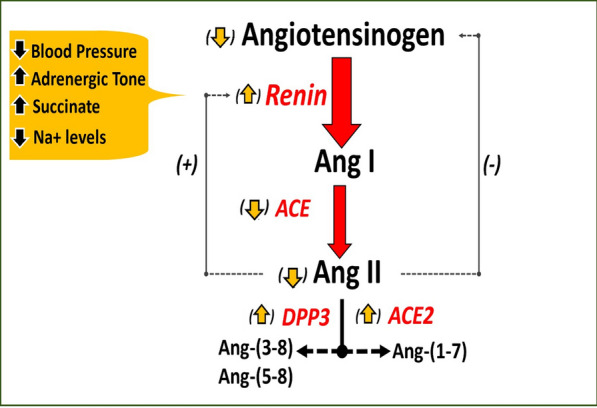
Dysregulation of the RAS in sepsis and septic shock. Circulating angiotensinogen is processed by renin to angiotensin I (Ang I), which is immediately converted to Ang II by ACE. Ang II is metabolized by dipeptidyl peptidase 3 (DPP3) to Ang-(3–8) and Ang-(5–8) while ACE2 converts Ang II to Ang-(1–7). Ang II inhibits the release of renin while Ang II stimulates the release of angiotensinogen. In sepsis and septic shock, lower blood pressure and tubular Na + but higher adrenergic tone and succinate stimulate renin release. Reduced levels of ACE but higher DPP3 and ACE2 contribute to blunted Ang II levels despite increased renin levels. Reduced Ang II and AT1 receptor (AT1R) responsiveness, as well as high renin levels may lead to lower circulating angiotensinogen, which may further depress the generation of Ang II. Lower Ang II and AT1R may also stimulate the release of renin. [6]
Adapted from Schaich et al.