

Abstract
Anterior Rotator cuff tears are one of the most common surgically addressed disorders, as the tears in the tendon can affect anyone regardless of risk factors or activity level. The rotator cuff is responsible for most of the shoulder motion, hence the tendon-bone interface experiences immense stress making it incredibly prone to failure. Rotator cuff tendon tears can either occur due to trauma or natural degeneration of the rotator cuff. To help mitigate effects of high stress on the rotator cuff tendon-bone interface, the rotator cuff is intrinsically designed to redistribute stress through protective mechanisms, such as the rotator crescent or coronal-transverse force. But when the tear goes through the intrinsic protective mechanisms, the glenohumeral joint is left unstable and thus is no longer capable of its normal range of motion. Location, size, and type of rotator cuff tendon tears are the strongest indicators for interventional therapy. Surgical therapies demonstrate low success rates, as seen by the significantly high recurrence rate of rotator cuff reinjury following initial repair. This is due to extrinsically healing of rotator cuff tendons, instead of the more intrinsic healing, which causes rotator cuff tendons to not undergo the necessary biomechanical remodeling to prevent reinjury leading to a mechanically and functionally inferior healed tendon. In this article, we thoroughly discussed the underlying pathophysiology of rotator cuff tears from onset to repair to healing, demonstrating that rotator cuff tendon healing is an intrinsically flawed process, irrespective of the risk factors, occurrence of rotator cuff tears, or surgical treatment. Rotator cuff healing can only be successful if rotator cuff tendon repair surgery is augmented with biologics to promote a successful intrinsic healing environment.
Keywords: Biomechanics, Inflammation, Infraspinatus tendon, Rotator cuff injury, Rotator cuff repair, Supraspinatus tendon, Tendinopathy
1. Introduction
The glenohumeral joint is a ball and socket joint composed of the humeral head and scapular glenoid fossa. Foundationally, the glenoid fossa is a quarter of the size of the articular surface of the humeral head making it an intrinsically unstable joint [1]. This extremely unstable joint is fully dependent on the rotator cuff muscles to provide the necessary stability required to keep the humeral head interfaced with the glenoid fossa.
The rotator cuff is composed of 4 muscles: subscapularis, supraspinatus, infraspinatus, and teres minor with respective tendons that come together to form the rotator cuff, a sheath which covers the head of the humerus as it sits in the glenohumeral joint. Subscapularis is responsible for internal rotation of the shoulder and prevents anterior dislocation of the humerus during abduction [2]. It originates on the anterior surface of the scapula in the subscapular fossa and inserts onto the lesser tuberosity of the humerus. The subscapularis tendon is the largest of the four tendons [1]. Supraspinatus is responsible for the initial 15° of shoulder abduction. It originates in the supraspinous fossa located on the posterior aspect of the scapula above the spine of the scapula and inserts onto the superior most portion of the greater tuberosity of the humerus. The supraspinatus tendon is the third largest of the four tendons [1]. Infraspinatus is responsible for the external rotation of the shoulder. It originates in the infraspinous fossa below the spine of the scapula and inserts onto the medial portion of the greater tuberosity of the humerus. The infraspinatus tendon is the second largest of the four tendons [1,3]. Teres Minor is responsible for external rotation of the shoulder. It originates on the posterior aspect of the lateral border of the scapula and inserts onto the inferior most portion of the greater tuberosity of the humerus. The teres minor tendon is the smallest of the four tendons [1].
The four muscles work together to abduct and rotate the humerus around the glenohumeral joint, thus allowing full range of motion [2]. The mobility of this joint comes at the cost of stability [4], making the rotator cuff the weakest point of the shoulder [5]. Over a 9-year period from 2007 to 2016, about 314,239 rotator cuff repairs were performed [6], making it “one of the most frequently encountered and surgically addressed diseases treated by an upper extremity surgeon” [7].
2. Clinical Presentation of Injury
Rotator cuff injury may start from trauma to the region. For younger individuals, this trauma usually is a sport related injury; for older individuals, this trauma usually comes from endogenous, age-related degeneration. Once there is trauma, patients will manage pain for as long as possible through compensatory actions, such as avoiding painful motion, reducing overall shoulder mobility, and/or by taking oral nonsteroidal anti-inflammatory drugs. Only when injury interferes with daily living or proves to be extremely painful will a patient seek physician intervention. At this stage, the patient may present with simple tendinopathy or further tendon damage from overuse, resulting in a partial or full tendon tear [4]. It is difficult to predict at what stage a patient will present as some tears may never progress beyond initial trauma, while some tears may increase in size. Those that do increase in size will do so gradually [7].
3. Risk Factors
In a study of 2738 symptomatic and asymptomatic shoulders, it was found that compared to patients without rotator cuff tears those with rotator cuff tears were older, were more likely to be a male, and had a greater BMI. There was also an increasing likelihood of rotator cuff tears with the presence of a previous diagnosis of carpal tunnel syndrome [8].
A meta-analysis of 26 articles from 14 countries consisting of 3164 patients and 6645 controls identified older age (≥ 60 years), greater BMI, dominant arm, greater height, and heavier weight as demographic factors associated with symptomatic rotator cuff tears. Disease factors such as history of shoulder trauma and hypertension were also associated with symptomatic rotator cuff tear. On imaging studies, greater acromion index, greater critical shoulder angle (≥ 35), and smaller glenoid version angle were identified factors associated with symptomatic rotator cuff tear [9-10].
A full analysis cohort of 292,666 rotator cuff repair patients showed that patients with diabetes mellitus were 48% more likely to need rotator cuff repair surgery than patients without diabetes mellitus [11]. Additionally, other metabolic factors, such as hyperlipidemia, have significant effect on the biomechanics of the shoulder rotator cuff before and after the repair [4,5,12]. Diabetes, hyperlipidemia, smoking, and hypoxia induce inflammatory response with increase in the activation of inflammasomes and release of inflammatory cytokines, HMGB1, and other factors that lead to pathological changes, including collagen disorganization, alteration in the expression of other matrix components, and change in the exosomal contents of the tendon and surrounding fat in the rotator cuff [13-17]. Indeed, many genes are interconnected in the activation of various kinases, transcription factors, and karyopherins that lead to alterations in the transcription and translation of the pathological molecules with the involvement of epigenetic factors and microRNAs, resulting in pain and pathogenesis of tendinopathy and glenohumeral arthritis [18-22].
In older studies, smoking as a risk factor has been linked to rotator cuff tears, as it is a common risk factor in other musculoskeletal disorders [8,22]. The understanding is that nicotine reduces blood flow, therefore reducing oxygen delivery to the rotator cuff which prevents natural tendon healing from occurring [23]. In a study by Baumgarten et al. of 584 patients with and without rotator cuff tears, patients with rotator cuff tears were significantly more likely to have a positive history of daily tobacco smoking compared to those without rotator cuff tears [22].
With an abundance of risk factors, the average person, regardless of activity level, is at risk of a rotator cuff injury. Risk factors, such as gender, cannot be changed, while lifestyle risk factors are highly prevalent in many populations and cannot be radically improved. For that reason, even after rotator cuff repair, patients will struggle to achieve successful tendon healing due to risk factors.
4. Clinical Classification of Rotator Cuff Tear
Rotator cuff tears can be defined by size, depth, tear pattern [24]. Depth wise, a tear can be either partial or full thickness. Tear pattern can be L shaped, U shaped, or crescent shaped. Partial thickness tears are defined by Ellman’s classification system where grade I is < 3 mm deep (25% of tendon thickness), grade II = 3 - 6 mm deep (25-50% of tendon thickness), and grade III ≥ 6 mm deep (>50% of tendon thickness). These partial tears can be articular sided, bursal sided, or intratendinous [25,26]. Full thickness tears can be defined by Cofield’s classification system where a small tear is < 1 cm, a medium tear is between 1 - 3 cm, a large tear is 3 - 5 cm, and a massive tear is > 5 cm [27].
Another critical aspect that informs tendon health and surgical outcomes for a rotator cuff tear is how much fatty degeneration has occurred to the tendon. Fatty degeneration is characterized by atrophy of muscle fibers, fibrosis, and fatty accumulation within and around the rotator cuff muscles. Goutallier’s classification for fatty degeneration represents the relationship between muscle health and fatty degeneration, where an increase in stage number represents an increase in muscle atrophy and increase in conversion of muscle into fat and fibrosis. At stage 0 the muscles are normal, stage 1 some fatty streaks present, stage 2 the amount of muscle is greater than fatty infiltration, stage 3 the amount of muscle is equal to fatty infiltration, stage 4 the amount of fatty infiltration is greater than muscle [25]. Fatty degeneration is rarely reversible, is likely to progress to further stages with or without intervention, and there are currently no treatments for fatty degeneration [13,28,29].
Another aspect that helps provide information about rotator cuff tear is acromiohumeral distance (AHD), which is a measure of subacromial space. As a radiographic diagnostic tool, it has high specificity but low sensitivity. AHD is measured as the shortest distance between the humeral head and acromion, with normal AHD being approximately 10 mm. AHD ≤ 7 mm suggests a large rotator cuff tear. AHD < 6 mm indicates a full thickness tear. A smaller AHD than normal means the humeral head is migrating superiorly; therefore, it can be assumed there is a rotator cuff tear. A small AHD after rotator cuff repair can indicate an inadequate repair or subpar rotator cuff tendon healing [20,31].
The most used rotator cuff tear classification systems have been discussed (Table 1), as these are crucial for characterizing rotator cuff pathology for surgical intervention. There are more classification systems beyond what is listed here as rotator cuff tears are extremely complex to characterize with many variations in tears from person to person. Imaging via CT, ultrasound, and MRI have limitations that prevent accurate and through visualization of rotator cuff pathology, therefore multiple classification systems must be enlisted to capture the complexity of rotator cuff injury.
Table 1:
Common Clinical Classifications of Rotator Cuff Tears.
| Tear Pattern | L-Shape, U-Shape, or Crescent Shape |
|---|---|
| Ellman’s Classification System: Partial Thickness Tear Size | Grade I → < 3 mm deep; 25% of tendon thickness Grade II → 3 - 6 mm deep; 25 - 50% of tendon thickness Grade III → ≥ 6 mm deep; Greater than 50% of tendon thickness |
| Cofield’s Classification System: Full thickness Tear Size | Small Tear → < 1 cm Medium Tear → 1 - 3 cm Large Tear → 3 - 5 cm Massive Tear → > 5 cm |
| Goutallier’s Classification: Fatty Degeneration | Stage 0 → Muscles are normal Stage 1 → Some fatty streaks present on the muscle Stage 2 → the amount of muscle is greater than fatty infiltration Stage 3 → the amount of muscle is equal to fatty infiltration Stage 4 → the amount of fatty infiltration is greater than muscle Normal → Approx. 10 mm |
| Acromiohumeral Distance (AHD) | Suggests a Full Thickness Rotator Cuff Tear → ≤ 7 mm Indicates a Full Thickness Tear → < 6 mm |
5. Rotator Cuff Stabilizing Mechanics
Rotator cuff injuries can affect anyone, as it is prevalent in both symptomatic and asymptomatic shoulders. With 272,148 rotator cuff repairs performed annually in the United States [8], rotator cuff anatomy and mechanics make it extremely vulnerable to damage and injury. This is why the rotator cuff muscles play a crucial role in shoulder mechanics by keeping the humeral head centered and stabilized in the glenoid fossa. These stabilizing forces create a fulcrum at the glenohumeral joint, enabling the humerus to abduct and rotate effectively.
The ability of the rotator cuff to center, stabilize, and fix the shoulder joint arises from force coupling. This involves the coordinated action of agonist and antagonist muscles, which generate opposing or synergistic forces to control joint position and movement. This coordination ensures stability, allowing for smooth and efficient joint motion.
The shoulder has two key force couples, coronal and transverse (Table 2). The coronal force couple (Figure 1) is the opposing force relationship between the deltoid muscle and subscapularis-infraspinatus- teres minor muscles. Deltoid pulls the humeral head upward during abduction, thus creating an upward and outward rotational force that needs to be counteracted to prevent the humeral head from moving out of the glenoid fossa. Subscapularis-infraspinatus-teres minor apply a stabilizing, opposing downward and inward counterforce that stabilizes the humeral head against the upward pull of the deltoid. The coronal force couple helps maintain the glenohumeral joint as a fulcrum for humerus motion [32,33].
Table 2:
Coronal and Transverse Force Couple Dynamics for Stabilizing the Glenohumeral Joint.
| Coronal Force | Opposing force relationship between the deltoid muscle and subscapularis- infraspinatus-teres minor Deltoid pulls the humeral head into abduction, while subscapularis- infraspinatus-teres minor apply a stabilizing, opposing downward and inward counter force. |
| Transverse Force | Opposing force relationship between subscapularis and infraspinatus-teres minor Subscapularis pulls the humeral head anteriorly during internal rotation, while infraspinatus-teres minor apply a stabilizing, opposing inward counterforce. |
Figure 1:
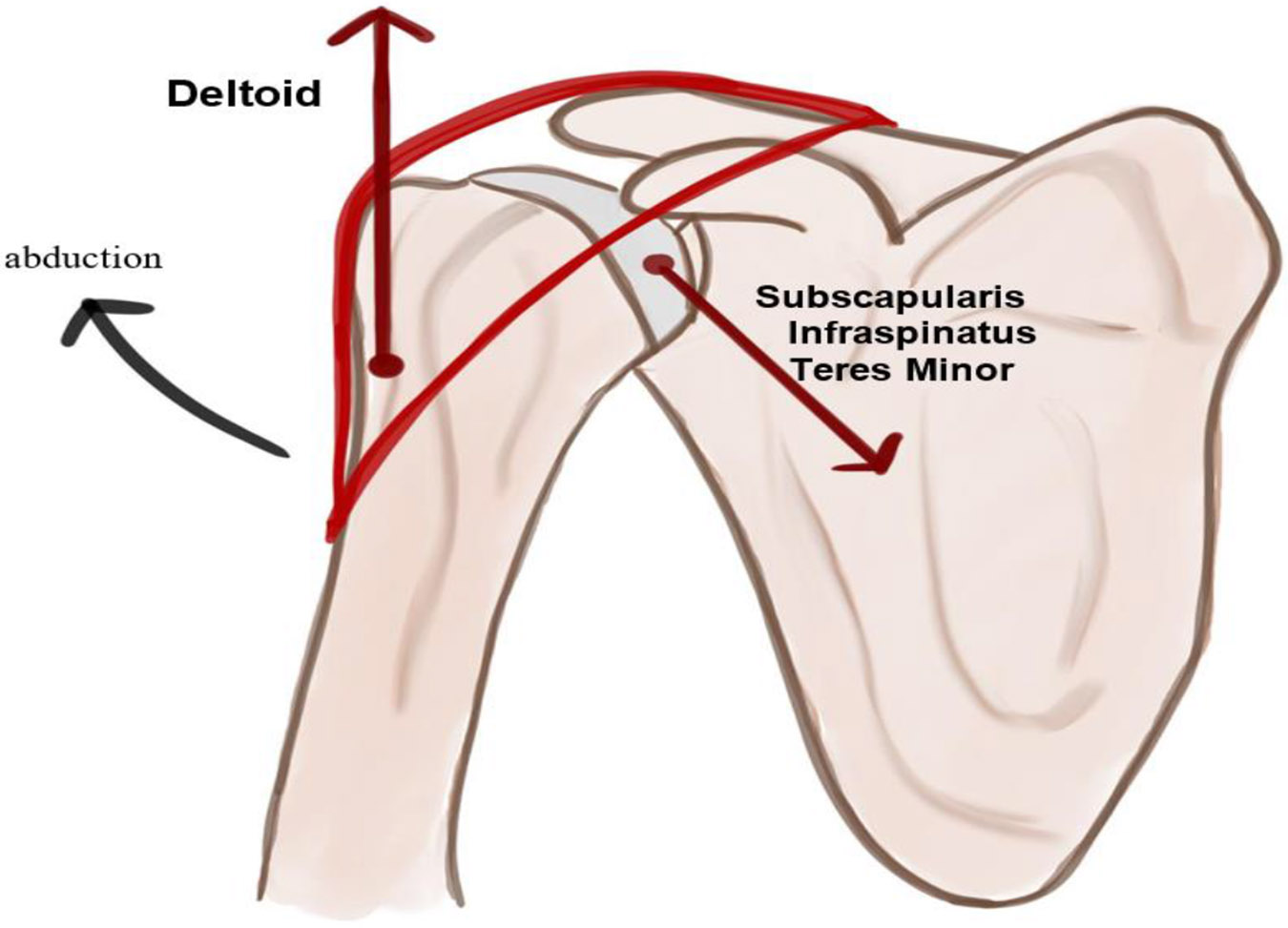
Coronal Force Couple showing opposite force relationship between the deltoid muscle and subscapularis-infraspinatus-teres minor muscles.
The transverse force couple (Figure 2) is an opposing force relationship that maintains downward stability through the motions of subscapularis and infraspinatus-teres minor. Subscapularis pulls the humeral head anteriorly during internal rotation, thus creating a rotational force that needs to be counteracted to prevent the humeral head from moving out of the glenoid fossa. Infraspinatus-teres minor applies the necessary posterior, inward counterforce that prevents the humeral head from sliding out of the glenoid fossa anteriorly. This relationship works both ways with subscapularis providing a counterforce when infraspinatus-teres minor externally rotates. The transverse force combined with the coronal force couple provides stability at the glenohumeral joint [33-35].
Figure 2:
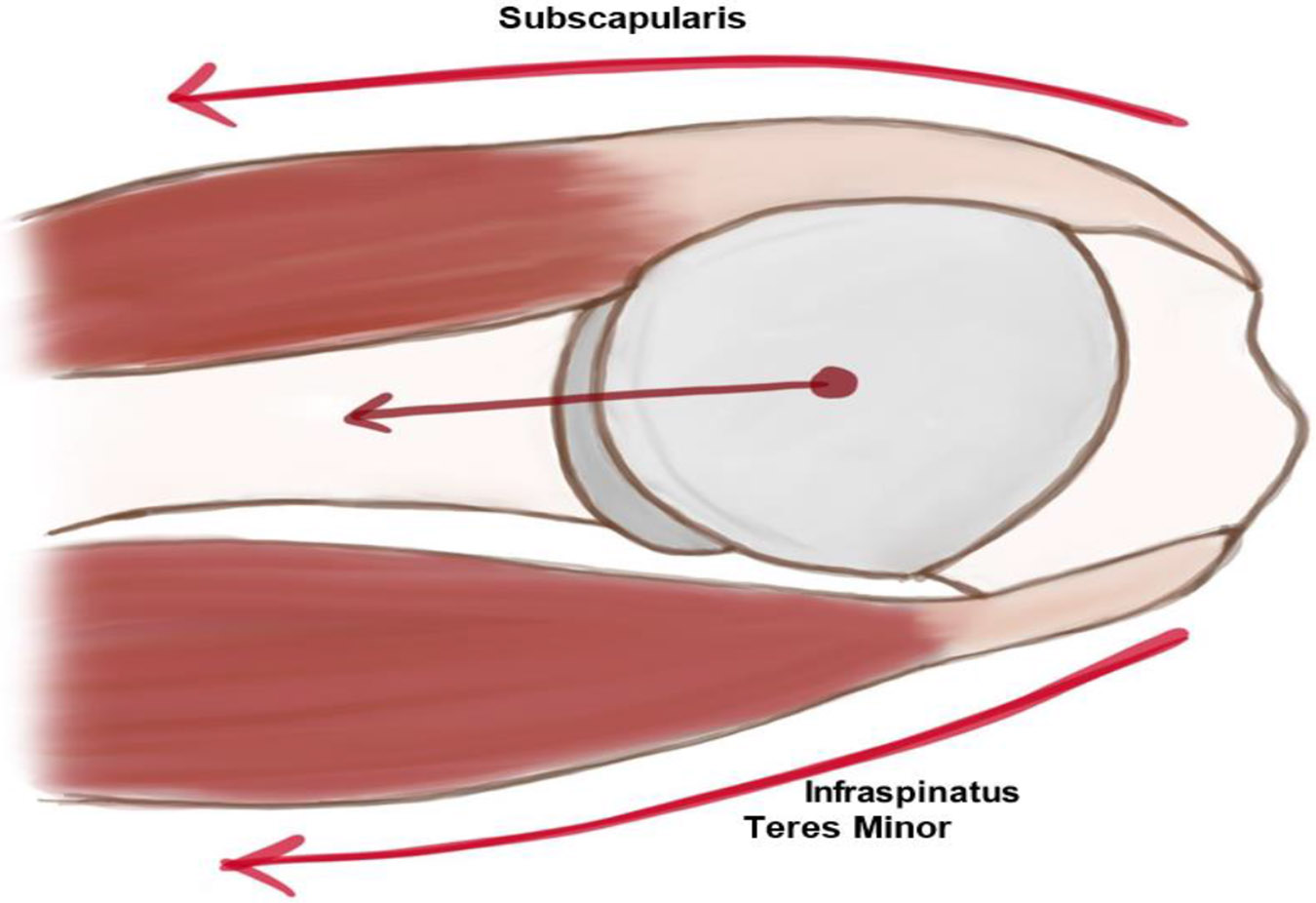
Transverse Force Couple showing opposite force relationship to maintain downward stability through the motions of subscapularis and infraspinatus-teres minor.
Piepers et al. [36] took CT images of 27 non-pathologic shoulders to measure the muscle volume of subscapularis and infraspinatus-teres minor. The study concluded that there is no significant difference between the muscle volume of subscapularis and infraspinatus-teres minor. This result was independent of changes in shoulder positioning into adduction and elevation. Subscapularis and infraspinatus-teres minor muscle volumes being equal indicates that the respective muscle force must also be equal, therefore supporting the conclusion that the transverse force couple exists and plays a critical role in glenohumeral joint stability [36].
6. Presentations of Asymptomatic, Symptomatic with Trauma, and Symptomatic without Trauma Rotator Cuff Injury
Rotator cuff injuries can be categorized (Figure 3) as asymptomatic or symptomatic. Asymptomatic rotator cuff injuries can be defined as a patient who never demonstrates any symptoms of injury but upon imaging, rotator cuff injury is present. Asymptomatic rotator cuff injuries can be explained through the compensatory rotator cable-rotator crescent relationship masking a rotator cuff tear. Symptomatic rotator cuff injury can be defined as a patient who presents with symptoms of rotator cuff injury and there is clear presence of rotator cuff injury. The injury itself can be either caused by trauma or natural degenerative damage of rotator cuff tendons. If the injury is traumatic in nature, it is due to a disruption of either the coronal or transverse force couple that maintains glenohumeral joint stability. If the injury is due to natural degeneration, it can be explained by extrinsic or intrinsic factor theory weakening rotator cuff tendons causing failure to occur.
Figure 3:
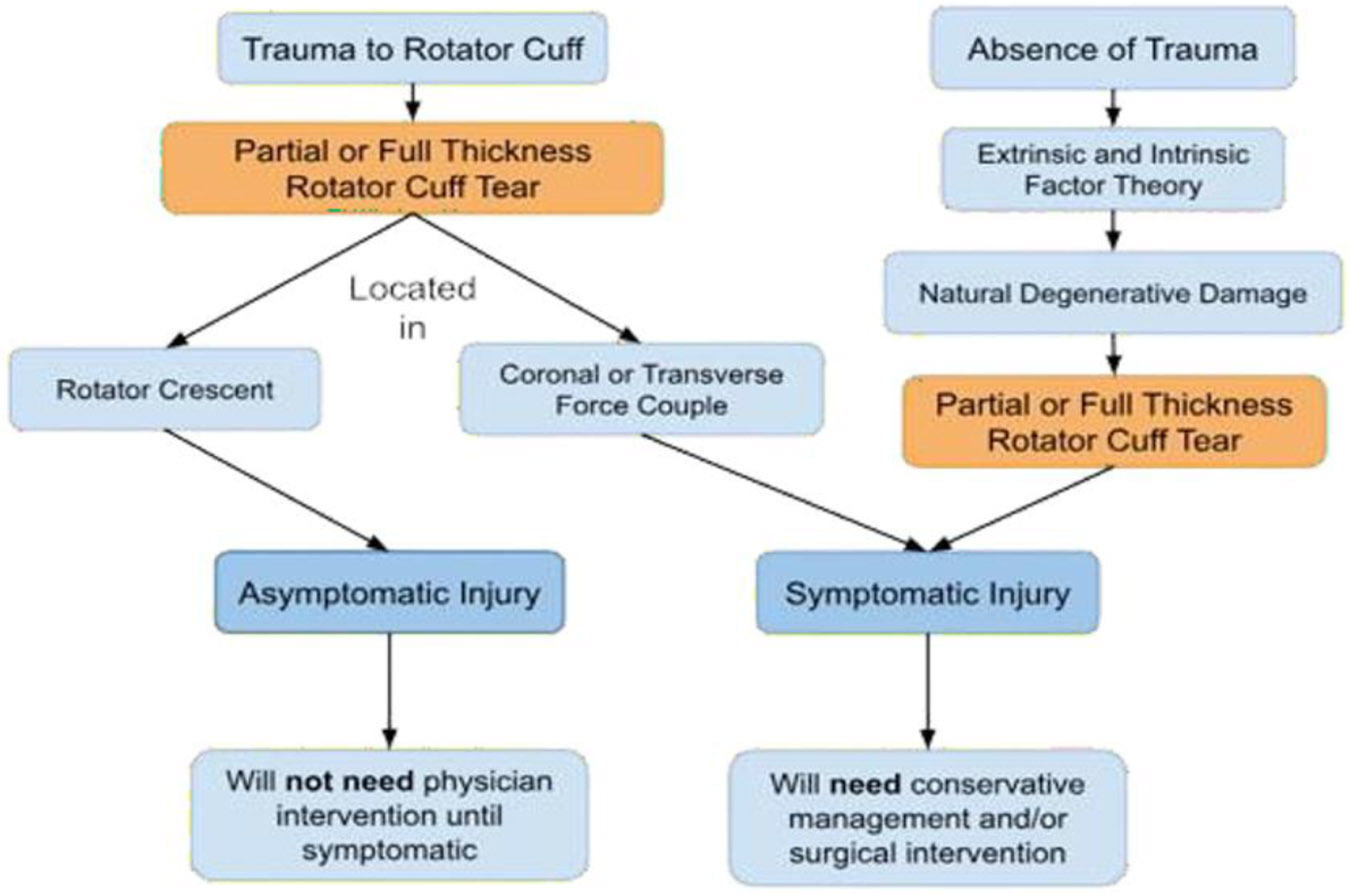
Presentation of Asymptomatic and Symptomatic Rotator Cuff Injury, underlying Pathology, and Clinical Intervention.
7. Asymptomatic Shoulders with Rotator Cuff Injury
In a study of 411 aged 50 - 80+ asymptomatic shoulders, which are patients who had no symptoms of shoulder pain, 23% of patients were found to have full thickness rotator cuff tear. The presence of rotator cuff tear had no significant correlation with sex, arm dominance, or activity levels, thus demonstrating age degeneration of the rotator cuff can exist as a normal condition of asymptomatic shoulders [37]. It is in individuals without shoulder pain, 5 - 40% have full thickness rotator cuff tears [38]. The prevalence of rotator cuff injury in asymptomatic shoulders can be explained by the rotator cable and rotator crescent relationship.
The rotator crescent is defined as an avascular zone beneath the intersection of supraspinatus and infraspinatus tendons. The margin of the rotator crescent has thick bundles of fiber called the rotator cable (Figure 4). The rotator cable provides support and absorbs excess mechanical load placed on the rotator cuff, thus shielding the more delicate rotator crescent from any excess mechanical stress. Whether it’s partial or complete tear, most rotator cuff tears occur within this rotator crescent [39].
Figure 4:
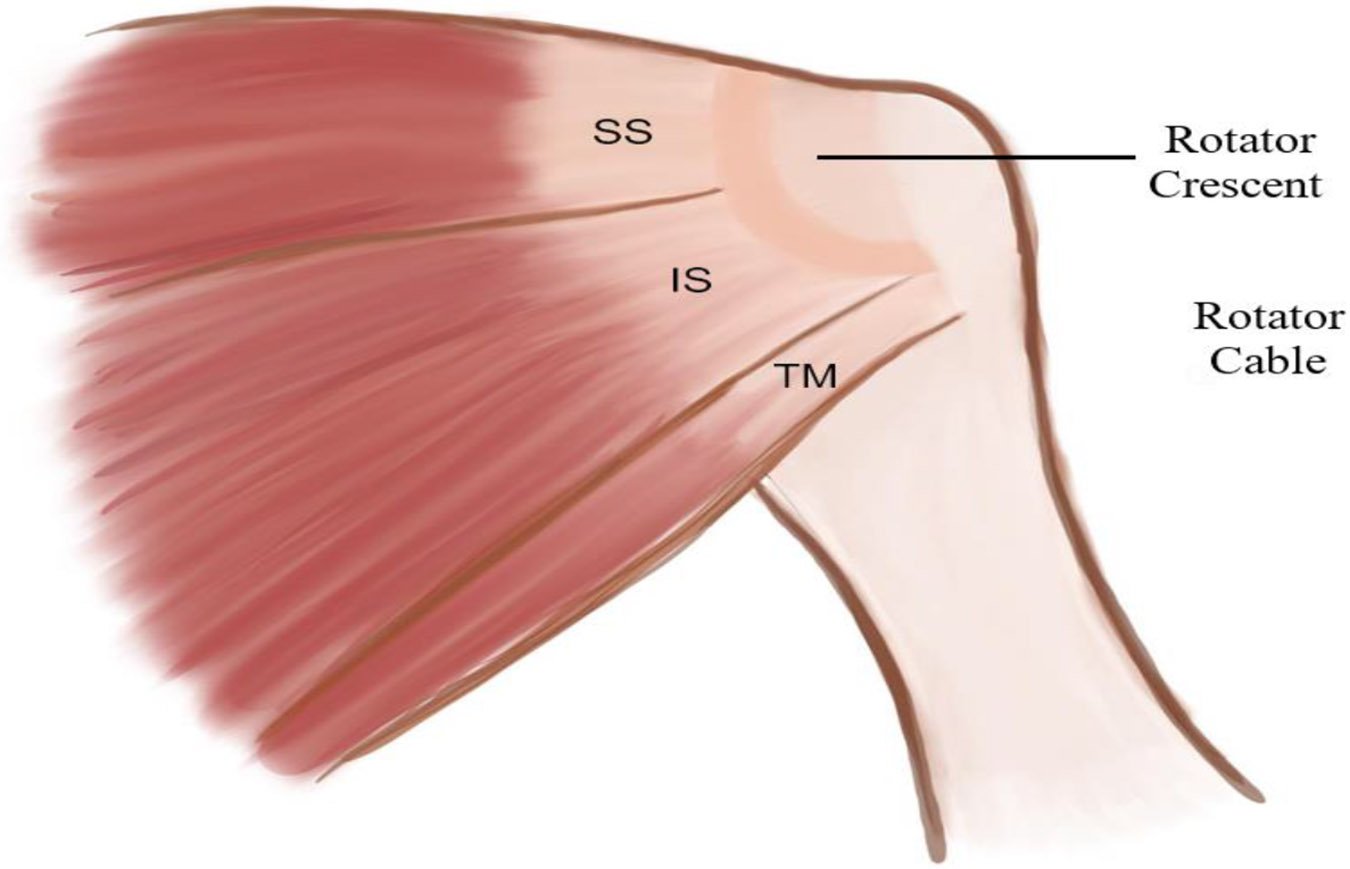
Schematic diagram showing Rotator Cable-Rotator Crescent Relationship. The margin of the rotator crescent has thick bundles of rotator cable fibers. SS = Supraspinatus, IS = Infraspinatus, TM = Teres Minor.
Analogizing the rotator cuff to a suspension bridge (Figure 5), the rotator cable is comparable to the main cable of a suspension bridge, while supraspinatus and infraspinatus tendons are comparable to the main towers on the anterior and posterior side of the suspension bridge. This suspension bridge analogy demonstrates how the stress shielding effect of the rotator cable works. Any tear that occurs in the rotator crescent can be compensated for by the rotator cable, supraspinatus, and infraspinatus tendons. Working together, they redistribute any mechanical stress placed on the bone-tendon interface to the respective tendons thus keeping the humeral head compressed within the glenoid fossa. If the tear propagates through the rotator cable and/or affects one of the tendons, the rotator cable-rotator crescent relationship is destroyed and can no longer maintain glenohumeral stability [39,40].
Figure 5:
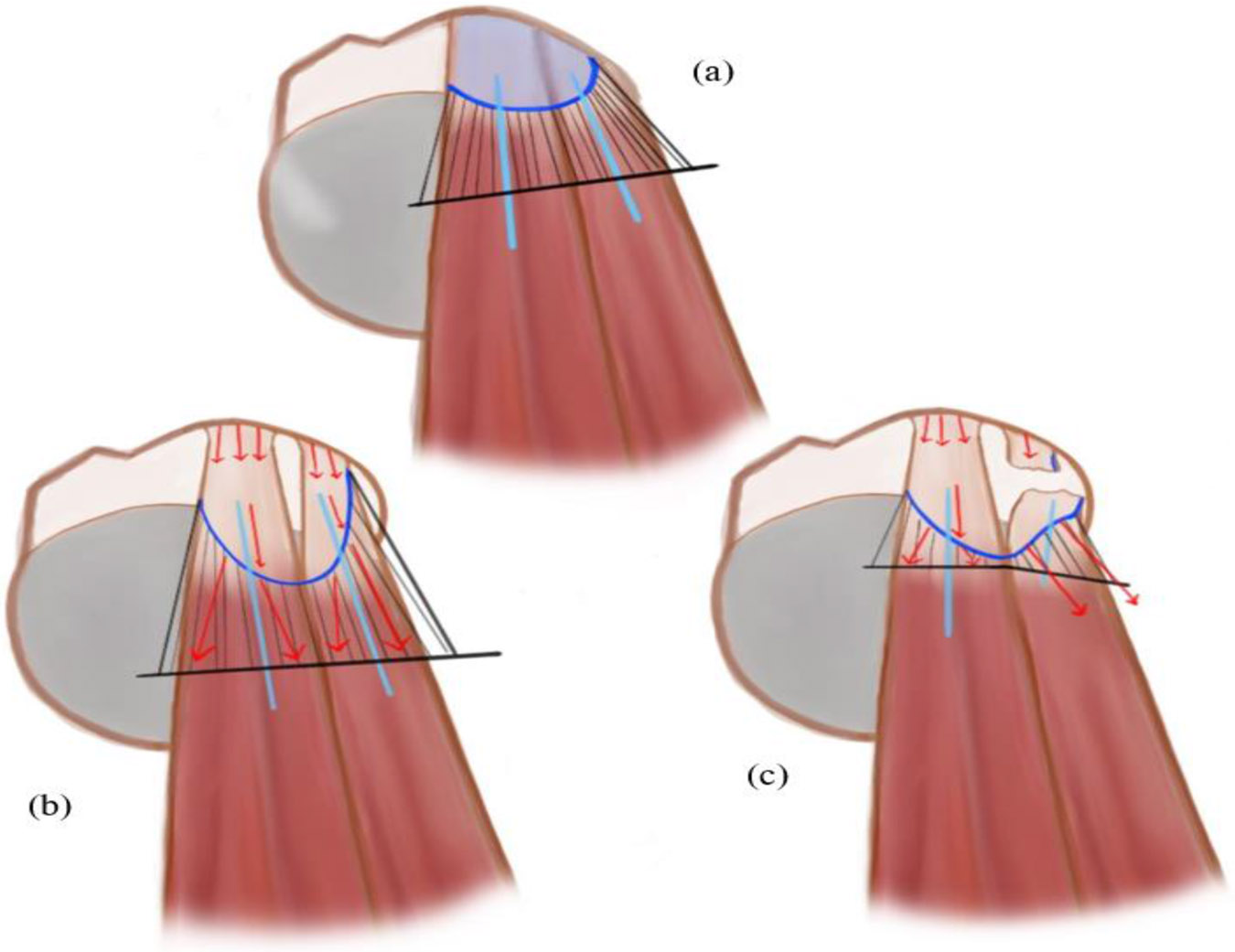
Schematic diagram showing Rotator Bridge Analogy to Suspension Bridge. (a) light blue shaded region = rotator crescent, dark blue line = rotator cable, light blue line = main towers of suspension bridge running in direction of muscle belly, (b) When supraspinatus and infraspinatus tendons are mechanically strained at the bone tendon interface, there is a high chance a rotator cuff tear will occur due to the plastic deformation of the tendon and rotator crescent. The rotator cable prevents this by redistributing the stress (red arrow) from the strained bone-tendon interface to the muscle belly of infraspinatus and supraspinatus. (c) If there is complete damage to either supraspinatus or infraspinatus tendons, then the rotator cable is rendered useless as there is no longer a redistribution of mechanical forces through the rotator cable into the respective muscle belly. The rotator cuff is now unstable as seen by the direction of forces (red arrow) in the torn infraspinatus.
Since the first establishment of the rotator crescent-rotator cable relationship by Clark et al. and Harryman [41] and Burkhart et al. [9,42], there has been conflicting research about whether the rotator crescent thins with age. Regardless of that fact, rotator cable thickening has been positively correlated with increasing age in both shoulders with or without rotator crescent thinning. This relationship confirms that over a person's lifespan the rotator cuff increasingly relies on the rotator cable to redistribute mechanical stress in order to prevent injury to the rotator crescent.
Burkhart et al. [39,42] used a Material Testing System to apply a symmetric 648.0 N force to 7 cadaveric shoulders with a tear in supraspinatus and half tear in infraspinatus. The study results revealed that when mechanical stress was applied to the tear, the tear only extended through the rotator cable and did not extend anteriorly or posteriorly into the remaining rotator cuff muscles.
Halder et al. [43] created various tears to the supraspinatus tendon in 10 fresh frozen cadavers to study the relationship between shoulder strength and rotator cuff tear. The results showed that an incision detaching either ⅓ or ⅔ of supraspinatus tendon causes only a minor effect on force transmission. The complete study suggested that a significant decrease in force transmission would occur only when total detachment of the supraspinatus tendon occurred. The study results reveals that minor tears in supraspinatus or infraspinatus tendons can be compensated for by the rotator cable; while large tears, such as complete detachment of supraspinatus or infraspinatus, that destroy the rotator cable cannot be compensated for as there is no longer a mechanism available to redistribute mechanical stress experienced by the rotator cuff [43].
The results of Burkhart et al. [39,42] and Halder et al. [43] studies demonstrate that the rotator cable-rotator crescent relationship allows injury to exist within the rotator cuff by using compensatory mechanisms to redistribute mechanical stress to maintain glenohumeral stability and motion. This relationship is how patients with asymptomatic rotator cuff tears can go about daily shoulder motions without any awareness of any rotator cuff trauma.
8. Symptomatic Shoulders with Trauma Causing Rotator Cuff Injury
The prevalence of rotator cuff injuries in symptomatic shoulders can be explained by damage to more than one rotator cuff muscle and/or tendon.
The rotator cuff can compensate for minor injury because the four muscles work together in coronal or transverse force couples to create either synergistic or opposing forces that maintain the stability of the glenohumeral joint. The moment there is damage to more than one rotator cuff muscle, the crucial coronal and transverse force couples can no longer keep the humeral head centered in the glenoid fossa leading to rotator cuff instability and injury [34,39].
Parson et al. [34] conducted a study with 14 cadavers, in which a dynamic shoulder testing apparatus was employed to understand the relationship between rotator cuff tears and reaction forces by using 5 conditions of rotator cuff tears: intact, incomplete supraspinatus tear, complete supraspinatus tear, supraspinatus-infraspinatus tear, and global tear. Reaction forces are two opposing forces with magnitude and direction that exist when an object remains stationary or moves uniformly. The study found that there was no significant difference in the reaction force magnitude for the incomplete and complete supraspinatus tendon tear conditions when compared to the intact condition. The supraspinatus-infraspinatus tear condition leads to a significant decrease in reaction force with changes to force direction. The lack of reduction in reaction force magnitude for incomplete and complete supraspinatus tears show the importance of the transverse force couple. Damage to only supraspinatus leaves the subscapularis and infraspinatus-teres minor relationship unaffected, which allows them to produce enough compensatory force to maintain similar conditions to “normal” or intact condition. Once both supraspinatus and infraspinatus are damaged, the transverse force couple is disturbed and there is an absence of a stable fulcrum at the glenohumeral joint– causing a significant reduction in reaction force magnitude. The force direction now points posteriorly as subscapularis must support an increased mechanical load during motion due to lack of counterforce from supraspinatus and infraspinatus. In the absence of supraspinatus-infraspinatus, subscapularis’ unbalanced joint motions shift the humeral head away from being stable and centered in the glenoid fossa [34].
9. Symptomatic Shoulders with an Absence of Trauma Having Rotator Cuff Injury
The only explanation for cases of symptomatic shoulders with tendinopathy but without clear trauma or multi-muscle damage is that the rotator cuff has experienced degenerative changes that have weakened the rotator cuff--which ultimately leads to partial or full thickness tears [33]. Tendinopathy, usually the first stage of progressive rotator cuff injury, is clinical defined as acute or chronic pain associated with inflammation. However, histological studies of patients with rotator cuff disease have found minimal inflammatory cells on rotator cuff tendons [44,45], thus implying that tendinopathy and progressive tendon degeneration must occur due to reasons other than inflammation. It has been proposed that these degenerative changes must either be from intrinsic, extrinsic factors, or both [33,45].
Extrinsic factor theory proposes that the primary contributor to degenerative weakening of the rotator cuff are factors external to the tendon, which are any anatomical or mechanical factors that increase stress on rotator cuff muscles [45,46]. These are factors such as mechanical compression from the acromion or coracoacromial ligament pressing onto the rotator cuff tendons, repetitive overhead activities, overuse, muscle imbalance, and poor biomechanics [45].
Intrinsic factor theory proposes that the primary contributor to destabilizing and degenerative weakening of the rotator cuff originates within the tendon. These are factors such as age-related degeneration, hypovascularity of tendon, cellular changes in collagen composition, and increased presence of degenerative cells [45,46].
Both extrinsic and intrinsic factors can mutually agonize each other. Extrinsic damage to the rotator cuff can increase intrinsic tendon degeneration and intrinsic degeneration can weaken the tendon making it more susceptible to failure from extrinsic mechanical stress [45].
10. Biomechanics of Rotator Cuff Tendons
Connecting muscle to bone, tendons play a critical role in transmitting and displacing forces between muscles and bones to stabilize joints. Tendons are also responsible for absorbing external forces to limit muscle damage [47-50], meaning they are exposed to extreme mechanical stress [51]. The tensile strength of a tendon is related to its thickness and collagen content. A tendon with a cross-sectional area of 1 cm2 can withstand 500-1000 kg of force [48,53]. While tendons can withstand high forces, the speed at which the load is applied determines the risk of tendon failure. Fast or angled tension on tendons with microtears, or during eccentric (muscle lengthening) contractions, greatly increases rupture risk [48,49,54].
The stress-strain curve of a tendon is shown in Figure 6. At rest, collagen fibers and fibrils display a crimped configuration. At the toe region, where the tendon is strained 2%, these crimps begin to straighten. At the linear region, where the tendon is strained between 2 - 4%, the crimp pattern is flattened, and deformation is due to the intramolecular sliding of the collagen triple helices. This is where the helices are sliding relative to each other allowing the collagen fibers to align more parallel to the direction of the strain [48,49,55]. If the strain is below 4%, the tendon behaves elastically and can return to its original shape after the load is removed [48,49]. Strains above 4% cause microscopic damage. Strains between 8-10% result in macroscopic failure, where there is noticeable damage and tears to the tendon [49,56]. Beyond 10% strain, there will likely be tendon rupture [57,58].
Figure 6:
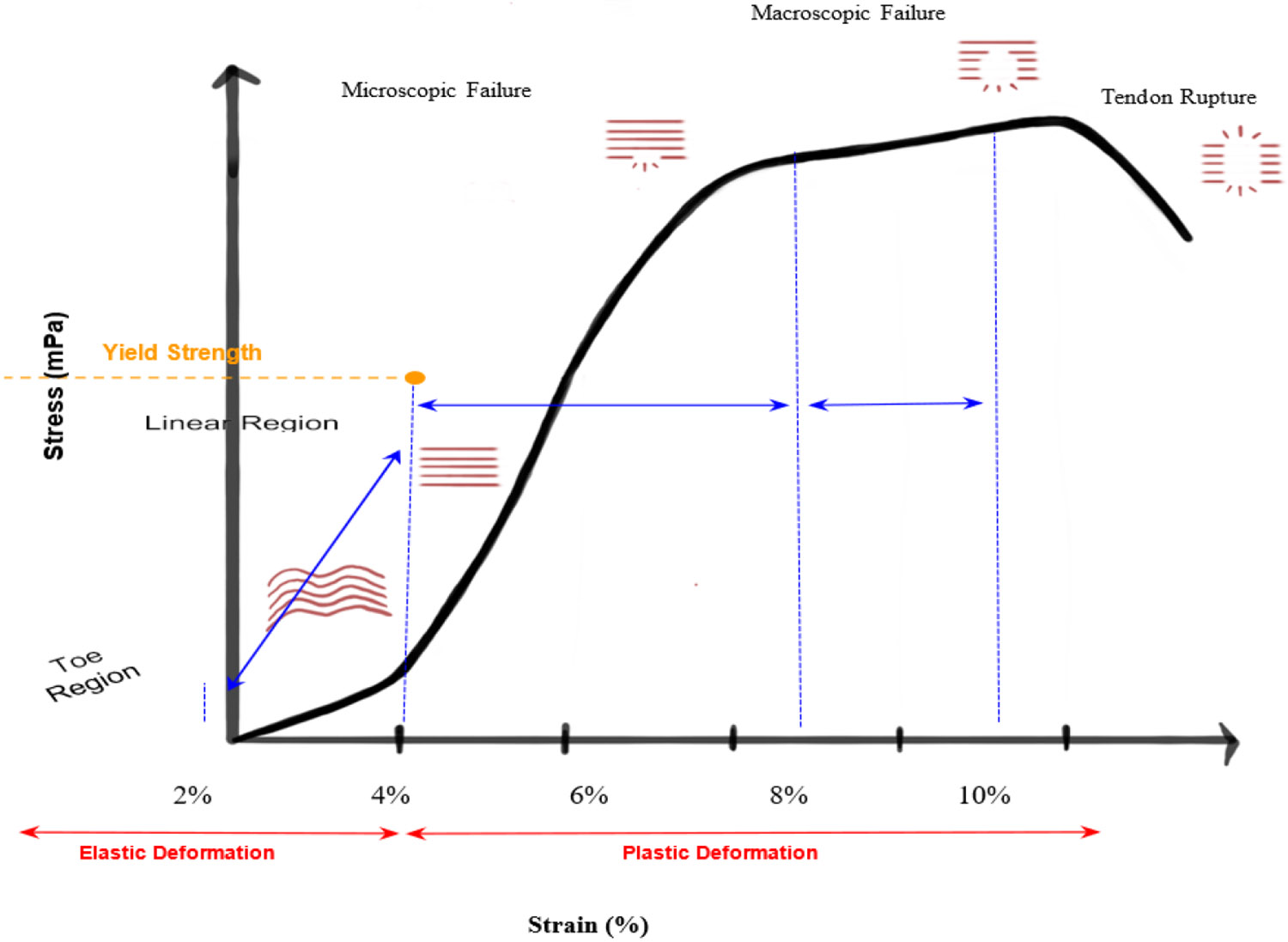
Stress/Strain Curve for Tendon. At rest, collagen fibers exist in a crimped configuration. Toe region, 0 - 2%, the collagen fibers begin to straighten. Linear region, 2 - 4%, the crimp pattern disappears, and the collagen fibers are straightened. 4% strain and below marks elastic deformation in which the tendon can still return to its original shape. Yield strength is at 4%. Strains above 4% mark the start of plastic deformation, where the tendon will undergo microscopic or macroscopic damage and can no longer return to its original shape when load is removed. 10% strain marks the fracture point and any strain beyond 10% will result in tendon rupture.
11. Tendon Composition
The ability of tendons to withstand mechanical strain comes from the composition of tendons, which allows for stable but adaptable structural integrity [52]. Tendons are composed of tenoblasts and tenocytes lying within a network of extracellular matrices. Tenoblasts are immature tendon cells that mature to form tenocytes. Tenocytes synthesize extracellular matrices, consisting of collagen, and are active in energy generation. Tendons are layered structures composed of collagen molecules, fibrils, fiber bundles, fascicles, and tendon units. The bundles of fascicles are surrounded by a connective tissue sheath called epitenon. The epitenon contains the vascular, lymphatic, and nerve supply to the tendon. The epitenon is surrounded by another layer of connective tissue called paratenon. Together, the epitenon and paratenon make up the peritenon. The configuration of epitenon and paratenon around a tendon helps reduce friction with adjacent tissues, allowing for smooth motion in areas of high stress [58-60].
With age, tendons switch from aerobic energy generation to anaerobic, where oxygen consumption in tendons is 7.5 times lower than skeletal muscles. Anaerobic energy production allows tendons to carry loads and maintain tension for extended periods of time, all while avoiding ischemia and necrosis [48,49,61]. This beneficial anaerobic environment proves disadvantageous during injury, resulting in slower healing after injury.
12. Tendon Damage
Tendons form micro-injury or microtrauma when repetitive stress is placed on the tendon– even if it is within physiological limits. With trauma, if tenocytes have time to repair any sustained tendon micro- injuries, then, tendons can maintain structural and biomechanical integrity. But if there is continuous repetitive stress without any time for tenocytes to synthesize new extracellular matrices or break down damaged cells, then the tendon is unable to repair itself. Microtrauma causes abnormal loading conditions during tendon motion leading to non-uniform deformation and stress distribution resulting in localized fiber damage and continued tendon degeneration [47-49,62].
While intrinsic and extrinsic factors can weaken a tendon, excessive mechanical loading of tendons is a main causative factor of degeneration. The repetitive overloading of the tendon results in inflammation of the paratenon, degeneration of the tendon body, or both [49,58,63].
13. Tendon Rebuilding and Healing
Overall, tendon healing can occur intrinsically or extrinsically. Intrinsic healing consists of wound proliferation by epitenon and endotenon tenocytes. Extrinsic healing consists of migration and wound proliferation by cells from surrounding sheath and synovium, such as fibroblasts and myofibroblasts [49,64-67]. Intrinsic versus extrinsic healing determines how a tendon will heal and its resultant biomechanics, as tenocytes and fibroblasts have differing mechanisms of repair.
Cells from the tendon sheath (external cells) have a higher production rate of extracellular matrix components, particularly collagen when compared to epitenon and endotenon cells. Extrinsic healing mechanism also begins earlier in the healing process while the intrinsic mechanism occurs later. Overall, this means an earlier thus prolonged inflammatory response occurs with extrinsic healing, leading to sustained activation of fibroblasts and myofibroblasts which results in a longer onset of continued collagen synthesis [68-73].
Intrinsic healing results in improved biomechanics and fewer complications. In intrinsic healing, tendon gliding mechanics are preserved– which allows for smooth motion of the tendon, efficient stress distribution between muscle and bone, protection of tendon from trauma, and reduced friction with surrounding tissues [48,49,74]. In extrinsic healing, the excess collagen production from fibroblasts results in adhesion formation disrupting tendon gliding mechanics, thus forming tendons that are biomechanically compromised [47-50]. There is no predictor, beside tissue type, for when intrinsic versus extrinsic healing occurs. For torn rotator cuffs, extrinsic healing tends to prevail [47-49,58]. Tendon healing occurs in three overlapping phases: inflammatory, repairing, remodeling (Table 3) [49,58].
Table 3:
Intrinsic vs. Extrinsic Healing. A comparison of the unique differences between intrinsic and extrinsic healing through the stages of tendon healing.
| Intrinsic Healing Tendon | Extrinsic Healing Tendon | |
|---|---|---|
| Inflammatory Phase → first 24 hours after injury | Proliferation of tenocytes from epitenon and endotenon | Proliferation of fibroblasts and myofibroblasts from surrounding sheath and synovium |
| Repairing or Proliferative Phase → few days to 6 weeks after injury | Slow collagen synthesis from tenocytes | Rapid type III collagen synthesis from fibroblasts and healing process begins earlier ↓ Formation of adhesions |
| Remodeling Phase → 6 weeks after injury to final healing | Balanced MMP/TIMP ↓ Collagen fibers aligned in direction of tension |
Unbalanced MMP/TIMP ↓ Disorganized and unaligned collagen fibrils even after remodeling |
| Final Outcome | Healed tendon with improved biomechanics and preserved tendon gliding mechanics | Tendon with adhesions, poor tendon gliding mechanics, and is biomechanically compromised. |
14. Initial inflammatory phase: First 24 hours after injury
Erythrocytes, platelets, and inflammatory cells (neutrophils, monocytes, macrophages) proliferate the injury and phagocytosis of damaged tissue begins [48,49].
In intrinsic healing, tenocytes, activated by inflammatory signals, proliferate and migrate to the wound. In extrinsic healing, fibroblasts from the nearby tissues migrate to the tendon signaled by tendon release of cytokines and growth factor. Both tenocytes and fibroblasts initiate type III collagen synthesis [48,49,75].
Type I and III collagen make up most of the extracellular matrix. Type III collagen is more prevalent during the inflammatory phase of tendon healing as it produces thin, less durable fibers with a higher turnover– making it important for wound healing and tissue regeneration [69,71,76,77]. Type I collagen is more prevalent in a healed or normal functioning tendon as it forms thick fibers that have a lower turnover rate. Type I forms the scaffold found within the extracellular matrix, critical for maintenance of tensile strength [69,76,77].
15. Repairing or Proliferative Phase: A few days to 6 weeks after injury
During the repairing stage, type III collagen formation peaks due to tenocyte or fibroblast presence, forming a disorganized, provisional matrix to stabilize injury [48,49,75]. Activation, proliferation, and migration of tenocytes continues into the repair phase.
For an extrinsically healing rotator cuff tendon, it is key to note that fibroblasts inherently have less activation steps, therefore are able continue to proliferate and produce collagen type III in excess compared to the tenocyte function [78]. The significant imbalance in collagen type I/III facilitates the start of scar tissue formation. The lower quantities of type I collagen indicate formation of a tendon with less tensile strength, a property of tendons that comes from type I collagen [69,79]. The abundance of collagen in extrinsic healing can lead to adhesions, where fibrous bands of collagen connect the tendon to surrounding tissues. Development of adhesions restrict normal tendon movement and gliding mechanics [48-50].
Remodeling phase: 6 weeks after injury to final healing
After six weeks, the remodeling stage begins, and the healing tissue changes in size and shape. The remodeling phase initially has a consolidation phase that lasts about four weeks, where the tissue changes from cellular to fibrous. This is marked by reduction in infiltration and proliferation of cellular components (such as tenocytes, fibroblasts, and immune cells) and increased synthesis of type I collagen [80]. The tendon at this stage is now a fibrous, collagen rich matrix. Enzymes, such as matrix metalloproteinases (MMPs), break down the initial disorganized collagen and extracellular matrix. This enables collagen fibers to remodel, resulting in alignment of the fibers and fibrils in the direction of stress by the end of the process [47-50]. The transition from cellular to fibrous is critical for restoration of tendon function and mechanical strength post injury. It also aids in the formation of a tendon that has increased resilience to functional demands of motion and load bearing activities, thus reducing the likelihood of re-injury. After 10 weeks, the maturation stage is defined by the gradual change of fibrous tissue to tendon scar tissue [48]. Remodeling continues over the course of at least a year with the initially formed scar tissue gradually being replaced by a more organized functional tendon tissue [48,49,58].
MMPs break down the initial collagen matrix and any excess collagen, facilitating scarless healing. MMPs activity is regulated by tissue inhibitors of metalloproteinases (TIMPs). A balanced ratio of MMPs and TIMPs is critical for tendon homeostasis, as an unbalanced ratio impairs tendon healing ability [81,82]. Intrinsically healed tendons have a more balanced MMPs/TIMPs ratio which leads to a more organized collagen formation, therefore healthy, functional tendon healing. Extrinsically healed tendons have an unbalanced MMPs/TIMPs ratio caused by fibroblasts producing IL-2 which activates TGF-β1, an inhibitor of MMP synthesis. In intrinsic healing, TGF-β1 is suppressed by macrophages which allows for scarless healing [81,83], but in extrinsic healing the excess of TGF-β1 during healing causes scar tissue formation due to excess collagen type III, contributing to the formation of adhesions and an overall mechanically weak healed tendon [81,84,85].
Adhesions formed during the repair/proliferative phase will continue to mature, becoming thick and fibrotic. These mature adhesions are not responsive to remodeling efforts, thus creating a structural integrity issue within the tendon as the adhesions physically prevent collagen fibers from aligning with the direction of stress. Adhesions naturally tether the tendon to surrounding structures, thus restricting its gliding mechanism [47-49]. This impairs the range of motion and can lead to chronic pain and stiffness [86].
At the end of the intrinsically healing process, the tendon collagen fibers align in the direction of tension and increase covalent bonding between collagen fibers resulting in a healed tendon with higher stiffness and tensile strength. This allows for tendons to adapt to mechanical loads, thus preventing injury from reoccurring [57].
At the end of the extrinsically healing process, such as for a rotator cuff tendon, the initial tendon scar tissue does not get replaced even with remodeling efforts. The collagen fibers within the now tendon scar tissue remain disorganized and unaligned [68]. This tendon scar tissue is thick, dense, and rigid with reduced elastic properties. Overall, extrinsically healed tendons have decreased mechanical strength, stress response functions, and functionality [87].
There are many factors during healing that must align for injured tendons to heal with appropriate biomechanics that prevent re-injury and mechanical failure. Rotator cuff tendons inherently, due to extrinsic healing properties, cannot heal tendon damage successfully; the natural healing ability of a rotator cuff tendon is slow, subpar, and biomechanically weak. Natural tendon healing takes a lengthy duration, a timeline of one year, in which the average person must take precaution to not cause re-injury. The healing timeline is incompatible with the average working individual’s lifestyle thus adding increased likeness of damage to the already poorly healing, structurally weak rotator cuff tendon. This is why conservative treatment may or may not prove to be beneficial for the patient. Considering the complex nature of rotator cuff tendon healing, any surgical interventions must consider tendon structure, composition, and biomechanics to support post tear recovery.
16. Repair Techniques for Rotator Cuff Injury
Conservative/non-operative treatment:
The goal of conservative treatments is to prevent further progression of rotator cuff injury and to stop the onset of rotator cuff arthropathy. Conservative treatments include ice, non-steroidal inflammatory drugs [88], activity modification, corticosteroid treatment, and physical therapy to strengthen accessory shoulder muscles, such as the deltoid. The subacromial corticosteroid injection is a combination corticosteroid and anesthetic injected using a posterolateral approach into the acromion to the rotator cuff bursal area. The corticosteroid injection helps decrease inflammation during rehabilitation to help with injury healing [89]. Those who respond to nonsurgical management will typically do so within the first 6 to 12 weeks [90].
Moosmayer et al. [91] split 103 patients with a rotator cuff tear not exceeding 3 cm (small to medium tears) into two groups, primary tendon repair or physiotherapy with optional secondary repair. The patients were followed up with at 6 months, then 1, 2, 5, and 10 years. 14 patients reported that physiotherapy, a form of conservative treatment, was not enough and crossed over to secondary surgery. Out of the 14 patients, 9 crossed over within the first year, with another 3 patients following between years 1 and 2. When a sonographic tear assessment was conducted at years 5 and 10 for the conservative treatment group, the tear size had increased both times in all participants. At the 10-year follow-up for conservative treatment group, 59% of patients had a tear size increase exceeding 5 mm and 41% of patients had an increase exceeding 10 mm. The study results conclude that in a comparison of treatment efficacy between the study groups over 10 years, primary tendon repair showed better results at all follow ups, indicating shoulder function remained stable in the surgical group but declined in the physiotherapy group. The study proposes that cuff tear arthropathy and muscle degeneration may have developed in unrepaired tears over the 10 years [91]. The study demonstrates the very issue with conservative treatment where it may improve clinical outcomes by addressing rotator cuff symptoms but does not repair injury and does not prevent further degeneration.
Surgical Interventions:
Partial repair, open repair, mini open repair, arthroscopic assisted surgery all have similar surgical steps but use different approaches to gain access to the rotator cuff tear. The common critical steps are [92-94]:
Debridement. This involves removal of damaged tissue, including frayed tendon edges, inflamed synovium, and any bone spurs that may be impinging on the rotator cuff.
Tendon mobilization. The damaged tendon(s) must be mobilized to better visualize the repair site.
Footprint formation. A footprint is the area of bone where the tendon will be reattached, thus the site must be surgically prepared by soft tissue removal and encouragement of vascularization.
Anchor placement. Surgeons place suture anchors, a biodegradable screw, into the humerus close to the site of repair. Sutures are passed through the tendon and are secured via the anchor, thus pulling the tendon onto the footprint to create a strong bone-tendon interface. This method is used both with a single row or double row suture technique.
The goal of any of the following surgical techniques is to secure the partial or fully torn rotator cuff tendon(s) back to the original location on the glenohumeral joint, thus allowing for natural tendon healing.
17. Partial Repair Operative Techniques
Debridement only
An ideal patient for debridement procedure only would be one that has an irreparable defect due to its lesion size, lacks osteoarthrosis, is not suitable for tendon transfer, and suffers from significant pain that is not manageable from conservative treatment [95]. This is most likely a patient of advanced age with low level of activity, has good remaining mobility, and experiences severe pain. This is ideal for tendons with grade I or II tears (< 6mm, < 50% of tendon thickness) [95]. The goal of debriding intervention is to help reduce pain and improve mobility, but there will not be a restoration of strength.
Partial Repair
Partial repair is used for partial thickness tears where only part of the tendon is damaged, an ideal patient would have a grade III tear (> 6 mm, > 50% of tendon thickness) and is unresponsive to conservative treatment [90]. Partial repair is generally performed using an arthroscope inserted into the joint to visualize the shoulder structures and confirm the diagnosis. The surgeon proceeds with debridement, tendon mobilization, anchor placement, tendon reattachment, and closure.
Complete Repair Operative Techniques
Complete repair is performed for full thickness tears in which the tendon is completely detached from the bone.
Open Repair Surgery
For open repair surgery, a large (4-6 cm) incision is made to directly access the deltoid, which is then detached to open the rotator cuff. Then the surgeon proceeds with debridement, if necessary, tendon mobilization, footprint preparation, anchor placement, tendon reattachment, deltoid reattachment, then closure [94].
Mini Open Repair Surgery
A mini-open can be viewed as an intermediate between open repair surgery and arthroscopic assisted surgery. An arthroscope is first used to visualize and assess the tear; debridement is performed, as necessary. A 3-4 cm incision is made parallel to the lateral border of the rotator cuff and the deltoid is then split, allowing the surgeon to see the damaged tendon(s). This incision is smaller than what is used for open repair surgery. The surgeon proceeds with tendon mobilization, footprint preparation, anchor placement, tendon reattachment, then closure [94].
Arthroscopic Assisted Repair Surgery
During arthroscopic repair, an arthroscope is inserted through a small incision (4-7 mm) and is used to visualize and assess the tear. The deltoid does not need to be moved or split. 2-3 more small incisions are made anterior, posterior, laterally at the level of the rotator cuff to allow tools to enter the surgical site. Debridement is performed as necessary, followed by tendon mobilization, footprint preparation, anchor placement, tendon reattachment, then closure [94].
Suture Anchor Techniques: Single Row vs Double Row
Single row repair uses only a single row of suture anchors along the medial edge of the rotator cuff footprint tied in a simple stitch pattern. This is a simpler technique with a shorter operative time and less hardware [96].
Double row repair uses two sets of suture anchors. The first row of anchors is placed on the medial edge of the rotator cuff footprint and is tied with a mattress stitch. The second row of anchors is placed superiorly or laterally near the greater tuberosity and is tied with a simple stitch pattern. This allows a larger surface area of the tendon to be in contact with the bone, therefore enhancing healing and improving footprint restoration post-operatively. Double row repair offers better biomechanical strength and allows healing tendon(s) to withstand forces normal to rotator cuff motion without risking retear. The surgical complexity of double-row repair makes it more technically demanding with a longer operative time when compared to single-row repair [96,97].
Patient Criteria for Interventional Methods
The American Academy of Orthopedic Surgeons developed an Appropriate Use Criteria for varying rotator cuff tear interventions. “Appropriate” indicates greater benefit than risk, “maybe appropriate” indicates benefit equal to risk, and “rarely appropriate” indicates benefit less than risk for each clinical scenario [98]. Out of all factors, rotator cuff tear size plays a significant role in determining appropriateness of debridement only, partial repair, complete repair, and reconstruction [90].
Non-operative treatment is always appropriate when patients demonstrate a positive response to conservative treatment. If patients do not respond to conservative treatment, partial repair/debridement was maybe appropriate for medium to massive tears, regardless of if it was a chronic tear or not [90].
Partial repair/debridement is rarely appropriate for a small tear, but maybe appropriate for a medium to massive tear. With the most ideal tear for partial repair being a grade III (>50%) tear [90].
Open or arthroscopic repair is maybe appropriate for a healthy patient with moderate or severe pain who is not responsive to nonoperative care [90].
It does matter whether the patient undergoes debridement, partial repair, open repair, or arthroscopic repair, what determines whether the surgery will be successful is how well the repaired tendon heals. The most ideal patient with optimal tendon healing outcomes is a non-smoking patient younger than 65 with a recent tear that has an AHD greater than 6 mm and a Goutallier scale grade of the infraspinatus or subscapularis muscle less than 2 [99-101].
With the substantial risk of rotator cuff retear and current limitations to improving the healing environment, understanding appropriate patient selection prior to surgery is critical. Careful evaluation of the patient, including age and risk factors, symptoms, and imaging study findings is crucial to optimize treatment decisions [99].
Reasons for Failure of Tear
It has been established throughout this paper that the timeline for successful natural tendon healing is lengthy and the extrinsic healing nature of rotator cuff tendons makes post-operative healing a delicate process. Often, rotator cuff repair results in retear which means a failure of successful surgical intervention. Varying surgical procedures steps have been studied to find the most ideal suture anchor pattern, suture configuration, and footprint preparation. Human factors such as tear morphology, fatty atrophy, muscle paralysis, and inflammatory cascades have also been well studied. Despite studying and manipulating these numerous factors to improve surgical outcomes, rotator cuff retear rates remain high [102].
In a pooled analysis of arthroscopic and open rotator cuff repairs with a minimum follow up of 9 years, Plachel et al. [103] found that there was no significant difference in postoperative functional scores, complications, and retear rates after failed rotator cuff repairs between arthroscopic and open/mini-open repair groups. The retear rate was 41% without significant difference between groups. The study results demonstrate that post-operative rotator cuff retears are going to occur regardless of surgical technique chosen.
Sugaya et al. [104] studied 80 shoulders in 78 patients with full thickness rotator cuff tears at an average of 35 months post arthroscopic rotator cuff repair. 39 shoulders were repaired with single-row technique and 41 shoulders were repaired using double-row technique. The study concluded that there were no statistical differences between the two groups demonstrating that surgical techniques truly do not change postoperative outcomes, as there are too many risk factors to control for [104].
Even if an ideal rotator cuff injury patient undergoes repair, healing can be compromised by any number of risk factor such as older age, nonsteroidal anti-inflammatory drug usage, smoking, AHD < 7 mm, fatty degeneration greater than stage 2, diabetes mellitus, and rheumatoid arthritis [99].
As most tears occur within the first 6 months after repair [90], retears are more likely caused by surgical repair that does not sufficiently support tendon healing. Miller et al. [102] postoperatively conducted an ultrasound of 22 patients who had undergone arthroscopic repair of large (3 - 5 cm) or massive (> 5 cm) rotator cuff tears at 2 days, 2 weeks, 6 weeks, 3 months, 6 months, 12 months, and 24 weeks. All patients were immobilized in a sling for the first 4 weeks postoperatively, rehabilitation protocol began with passive range of motion 4 - 6 weeks after surgery with active range of motion after 6 weeks. The sling was discontinued at 6 weeks. The results of the study support that many tears occur early in the first 6 months, with 29% of these early re-tears occurring within the 4-week immobilization [102]. An average re-tear size is 45% of the original tear surface area.
Rotator cuff repair surgery has a notable failure rate ranging from 13.1% to 79% depending on initial tear size, tendon involvement, and degree of muscle atrophy [105]. When rotator repair fails, biological healing has gone awry and factors that will impede proper healing, such as scar tissue, adhesions, fatty infiltration, muscle atrophy, decreased bone mineral density and inflammatory factors, prevail within the rotator cuff [106]. The complication rate after rotator cuff revision is twice the published rate for primary rotator cuff repair, making it imperative that a rotator cuff repair be done right the first time [107].
Current Dilemma and Future Directions
With poor tendon healing mechanisms, countless lifestyle risk factors impeding healing, high surgical failure rate, and poor patient outcomes post rotator cuff failure, the current standard of rotator cuff surgery must be improved to decrease postoperative retear risk. The best way to improve rotator cuff repair outcomes is to artificially promote intrinsic healing of the rotator cuff. Intrinsic healing creates an ideal environment that encourages scar-less tendon healing, thereby forming a tendon with biomechanics capable of withstanding stress distribution during and after healing.
Patch augmentation proves to be a simple but effective solution to improving rotator cuff outcomes. The aim of patch augmentation is to encourage native tissue growth, provide mechanical support, and create an optimal environment for rotator cuff healing. Patches can encourage tissue infiltration and incorporation of desirable factors that encourage natural rotator cuff healing [108]. Patches can also bridge the gap between a torn tendon and its native footprint, thus restoring natural bone-tendon connection that otherwise would not be possible [109].
The patch material is one of three types: animal, human, or synthetic. These patches can be seeded with biologics such as platelet rich plasma, mesenchymal stem cells, cytokines, and growth factors. Adding a patch operatively requires minimal deviation from standard arthroscopic, mini open, or open repair procedure. The augmented patch can either be implemented as a part of the repair or sutured over the repaired tendon [110].
Avanzi et al. [111] conducted a single-center, prospective, double blind, randomized control trial of 92 small to medium rotator cuff tear patients. Patients were divided into two groups that underwent rotator cuff repair using a single-row technique: one group which received surgical augmentation with a porcine dermal patch, while the other group did not receive any augmentation. Follow ups were conducted at 1, 3, 6, 12, and 24 months. The study results showed that within 2 years post-operative 97.6% of the augmented group had a successfully healed rotator cuff tear, compared to the 59.6% success rate of the standard repair group. The augmented repair group also showed improvement in repaired tendon thickness, footprint coverage, and healing rate.
Better rotator cuff repair outcomes are not only limited to xenografts, synthetic grafts and allografts both also show significant results. Cai et al. [112] conducted a prospective, randomized control of 112 moderate to large rotator cuff tear patients. Patients were divided into two groups that underwent rotator cuff repair using suture-bridge technique: one group which received surgical augmentation with 3D type I collagen scaffold, while the other group did not receive any augmentation. The study results showed that graft augmentation with 3D collagen resulted in improved clinical outcomes and decrease in retear rate after rotator cuff repair, with postoperative retear rate being 34% in the control group and 13.7% in the study group. The technique also promoted better tendon-bone integration and more aligned fibers with larger diameters in the study group over the control group. 3D collagen augmentation produces minor to no inflammation within host tissues and can successfully encourage active remodeling of collagen fibers [112,113].
Lee et al. [114] conducted a prospective, single blinded, randomized, controlled trial of 60 large-sized rotator cuff tear patients. Patients were divided into two groups that underwent arthroscopic rotator cuff repair using suture-bridge technique: one group received surgical augmentation with CGDerm allograft, an acellular human dermal matrix derived from cadaveric skin, while the other group did not receive any augmentation. The study results showed that retear rate within the allograft group was 9.1%, while the control group was 38.1% [114]. Augmenting rotator cuff repair with human dermal allograft increases healing capabilities and biomechanical strength of the repair, as shown in studies by Barber et al. [115,116].
The future of rotator cuff repair surgery lies in improving the post-operative success rate, thus decreasing rotator cuff retear rates. Patch augmentation, whether animal, human, or synthetic, has consistently demonstrated improved outcomes post-rotator cuff repair compared to non-augmentation.
18. Key points, Outstanding questions and Challenges
Rotator cuff pathology following shoulder injury is a 3rd most common musculoskeletal problem due to significant cause of pain, disability, and socioeconomic cost in the United States and around the world.
Due to extrinsic instead of intrinsic healing of rotator cuff tendons resulting in ineffective biomechanical remodeling, surgical therapies demonstrate low success rates, as seen by the significantly high recurrence rate of rotator cuff reinjury following initial repair.
One of the most significant factors predictive of structural failure following surgical repair is fatty infiltration of the rotator cuff tissue which is associated with severe inflammation, rotator cuff tendon stiffness, and re-tear.
Metabolic syndrome, including obesity, type 2 diabetes mellitus and hyperlipidemia, poses a greater risk of tendon rupture and poor tendon healing due to increased inflammation, impaired collagen reorganization and tendon stiffness and relates to fatty infiltration.
There is higher prevalence rate of rotator cuff injury in diabetics compared to general population.
Rotator cuff injury due to partial or complete tear could be asymptomatic or symptomatic and can be explained by rotator cable and rotator crescent relationship, by damage to rotator cuff muscle or tendon, or by degenerative changes without trauma.
Rotator cuff tendon is elastic and can return to its original shape after removal of load at a strain of less than 4% but may induce microscopic and macroscopic changes at higher strain and may undergo rupture beyond 10% strain.
Tendon healing can occur intrinsically or extrinsically with appropriate biomechanics if the collagen fibers align in the direction of mechanical load and there is increased covalent bonding between collagen fibers.
Since environmental and lifestyle factors significantly affect healing response, there is a need for increased awareness and development of better preventive and therapeutic approaches to avoid re-tear following surgery.
Advancement in the development of better technology, such as patch augmentation with or without biologics, is warranted to relieve pain and improve shoulder stiffness following surgery and improve post-operative success with decrease in the rates of rotator cuff retear.
Funding:
The research work of DKA is supported by the R01 HL144125 and R01 HL147662 grants from the National Institutes of Health, USA. The contents of this article are solely the responsibility of the authors and do not necessarily represent the official views of the National Institutes of Health.
Footnotes
Competing interests: All authors have read the manuscript and declare no conflict of interest. No writing assistance was utilized in the production of this manuscript.
Consent for publication: All authors have read the manuscript and consented for publication.
References
- 1.Akhtar A, Richards J, Monga P. The biomechanics of the rotator cuff in health and disease - A narrative review. J Clin Orthop Trauma 18 (2021): 150–156. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Merlin Rajesh Lal LP, Agrawal DK. Biomechanical forces in the tissue engineering and regeneration of shoulder, hip, knee, and ankle joints. J Biotech Biomed 6 (2023): 491–500. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Huegel J, Williams AA, Soslowsky LJ. Rotator cuff biology and biomechanics: a review of normal and pathological conditions. Curr Rheumatol Rep 17 (2015): 476. [DOI] [PubMed] [Google Scholar]
- 4.Merlin Rajesh Lal LP, Radwan MM, Thankam FG, Agrawal DK. Rotator cuff tendon repair after injury in hyperlipidemic swine decreases biomechanical properties. J Ortho Sports Med 5 (2023): 398–405 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Yazdani AN, Rai V, Agrawal DK. Rotator cuff health, pathology, and repair in the perspective of hyperlipidemia. J Orthop Sports Med 4 (2022): 263–275. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Yanik EL, Chamberlain AM, Keener JD. Trends in rotator cuff repair rates and comorbidity burden among commercially insured patients younger than the age of 65 years, United States 2007-2016. JSES Rev Rep Tech 1 (2021): 309–316. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Schmidt CC, Jarrett CD, Brown BT. Management of Rotator Cuff Tears. The Journal of Hand Surgery 40 (2015): 399408. [DOI] [PubMed] [Google Scholar]
- 8.Song A, Cannon D, Kim P, et al. Risk factors for degenerative, symptomatic rotator cuff tears: a case-control study. J Shoulder Elbow Surg 31 (2022): 806–812. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Zhao J, Luo M, Liang G, et al. What Factors Are Associated with Symptomatic Rotator Cuff Tears: A Meta-analysis. Clin Orthop Relat Res 480 (2022): 96–105. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Zhao J, Zeng L, Liang G, et al. Risk factors for symptomatic rotator cuff tears: a retrospective case-control study. Front Med (Lausanne) 10 (2024): 1321939. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Smith JM, Presson AP, Zhang C, et al. Does diabetes mellitus predispose to both rotator cuff surgery and subsequent failure? JSES Int 5 (2021): 636–641. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Merlin Rajesh Lal LP, Agrawal DK. Hyperlipidemia lowers the biomechanical properties of rotator cuff tendon. J Ortho Sports Med 5 (2023): 391–397. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Hoangvi Li, Rai V, Agrawal DK. Inflammation and fatty infiltration correlates with rotator cuff muscle atrophy in hypercholesterolemic Yucatan microswine. J Ortho Sports Med 6 (2024): 198–213. [Google Scholar]
- 14.Fang W, Sekhon S, Teramoto D, et al. Pathological alterations in the expression status of rotator cuff tendon matrix components in hyperlipidemia. Mol Cell Biochem 478 (2023): 1887–1898. [DOI] [PubMed] [Google Scholar]
- 15.Thankam FG, Agrawal DK. Hypoxia-driven secretion of extracellular matrix proteins in the exosomes reflects the asymptomatic pathology of rotator cuff tendinopathies. Can J Physiol Pharmacol 99 (2021): 224–230. [DOI] [PubMed] [Google Scholar]
- 16.Thankam FG, Roesch ZK, Dilisio MF, et al. HMGB1 priming triggers NLRP3 inflammasomes in the rotator cuff tendon injury. Sci Reports (Nature) 8 (2018): 8918. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Thankam FG, Dilisio MF, Dietz NE, Agrawal DK. TREM-1, HMGB1 and RAGE in the shoulder tendon: Dual mechanisms for inflammation based on the coincidence of glenohumeral arthritis. PLoS One 11 (2016): e0165492. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Thankam FG, Boosani CS, Dilisio MF, et al. Genes interconnecting AMPK and TREM-1 and associated microRNAs in rotator cuff tendon injuries. Mol Cell Biochem 454 (2019): 97–109. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Raney EB, Thankam FG, Dilisio MF, Agrawal DK. Pain and the pathogenesis of biceps tendinopathy. Am J Translational Res 9 (2017): 2668–2683. [PMC free article] [PubMed] [Google Scholar]
- 20.Thankam FG, Boosani CS, Dilisio MF, Agrawal DK. MicroRNAs associated with inflammation in shoulder tendinopathy and glenohumeral arthritis. Mol Cell Biochem 437 (2018): 81–97. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Thankam FG, Boosani CS, Dilisio MF, Agrawal DK. Epigenetic mechanisms and implications in tendon inflammation. Int J Molec Med 43 (2019): 3–14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Connor D, Thankam FG, Agrawal DK. Karyopherins in the remodeling of extracellular matrix: Implications in tendon injury. J Ortho Sports Med 5 (2023): 357–374. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Baumgarten KM, Gerlach D, Galatz LM, et al. Cigarette smoking increases the risk for rotator cuff tears. Clin Orthop Relat Res 468 (2010): 1534–1541. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Mosely LH, Finseth F. Cigarette smoking: impairment of digital blood flow and wound healing in the hand. Hand 9 (1977): 97–101. [DOI] [PubMed] [Google Scholar]
- 25.Lädermann A, Burkhart SS, Hoffmeyer P, et al. Classification of full-thickness rotator cuff lesions: a review. EFORT Open Rev 1 (2017): 420–430. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Ellman H. Diagnosis and treatment of incomplete rotator cuff tears. Clin Orthop Relat Res 254 (1990): 64–74. [PubMed] [Google Scholar]
- 27.Collin P, Matsumura N, Lädermann A, et al. Relationship between massive chronic rotator cuff tear pattern and loss of active shoulder range of motion. Journal of Shoulder and Elbow Surgery 23 (2014): 1195–1202. [DOI] [PubMed] [Google Scholar]
- 28.Bogdanov J, Lan R, Chu TN, et al. Degeneration of the rotator cuff: pathogenesis, clinical implications, and future treatment. JSES Rev Rep Tech 1 (2021): 301–308. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Thankam FG, Dilisio MF, Agrawal DK. Immunobiological factors aggravating the fatty infiltration on tendons and muscles in rotator cuff lesions. Mol Cell Biochem 417 (2016):17–33. [DOI] [PubMed] [Google Scholar]
- 30.Sanguanjit P, Apivatgaroon A, Boonsun P, et al. The differences of the acromiohumeral interval between supine and upright radiographs of the shoulder. Sci Rep 12 (2022): 9404. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Goutallier D, Le Guilloux P, Postel JM, et al. Acromio humeral distance less than six millimeter: its meaning in fullthickness rotator cuff tear. Orthop Traumatol Surg Res 97 (2011): 246–251. [DOI] [PubMed] [Google Scholar]
- 32.Inman Verne T, Saunders JB, dec M, et al. Observations of the Function of the Shoulder Joint. Clinical Orthopaedics and Related Research 330 (1996): 3–12. [DOI] [PubMed] [Google Scholar]
- 33.Pandey V, Jaap Willems W. Rotator cuff tear: A detailed update. Asia Pac J Sports Med Arthrosc Rehabil Technol 2 (2015): 1–14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Parsons IV IM, Apreleva M, Fu FH, et al. The effect of rotator cuff tears on reaction forces at the glenohumeral joint. J Orthop Res 20 (2002): 439–446. [DOI] [PubMed] [Google Scholar]
- 35.Burkhart SS. Fluoroscopic Comparison of Kinematic Patterns in Massive Rotator Cuff Tears. Clinical Orthopaedics and Related Research 284 (1992): 144–152. [PubMed] [Google Scholar]
- 36.Piepers I, Boudt P, Van Tongel A, et al. Evaluation of the muscle volumes of the transverse rotator cuff force couple in nonpathologic shoulders. Journal of Shoulder and Elbow Surgery 23 (2014): e158–e162. [DOI] [PubMed] [Google Scholar]
- 37.Tempelhof S, Rupp S, Seil R. Age-related prevalence of rotator cuff tears in asymptomatic shoulders. Journal of Shoulder and Elbow Surgery 8 (1999): 296–299. [DOI] [PubMed] [Google Scholar]
- 38.Edwards P, Ebert J, Joss B, et al. Exercise rehabilitation in the non- operative management of rotator cuff tears: A review of the literature. Int J Sports Phys Ther 11 (2016): 279–301. [PMC free article] [PubMed] [Google Scholar]
- 39.Burkhart SS, Esch JC, Jolson RS. The rotator crescent and rotator cable: An anatomic description of the shoulder’s “suspension bridge”. Arthroscopy: The Journal of Arthroscopic & Related Surgery 9 (1993): 611–616. [DOI] [PubMed] [Google Scholar]
- 40.Gyftopoulos S, Bencardino JT, Immerman I, et al. The Rotator Cable: Magnetic Resonance Evaluation and Clinical Correlation. Magnetic Resonance Imaging Clinics of North America 20 (2012): 173–185. [DOI] [PubMed] [Google Scholar]
- 41.Clark JM, Harryman DT II: Tendons, ligaments, and capsule of the rotator cuff. Gross and microscopic anatomy. J Bone Joint Surg Am 74 (1992): 713–725. [PubMed] [Google Scholar]
- 42.Burkhart SS. Shoulder arthroscopy: a bridge from the past to the future. J Shoulder Elbow Surg 29 (2020): e287–e296. [DOI] [PubMed] [Google Scholar]
- 43.Halder AM, O'Driscoll SW, Heers G, et al. Biomechanical Comparison of Effects of Supraspinatus Tendon Detachments, Tendon Defects, and Muscle Retractions. The Journal of Bone & Joint Surgery 84 (2002): 780–785. [DOI] [PubMed] [Google Scholar]
- 44.Fukuda H, Hamada K, Yamanaka K. Pathology and pathogenesis of bursal-side rotator cuff tears viewed from enbloc histologic sections. Clin Orthop Relat Res (1990): 75–80. [PubMed] [Google Scholar]
- 45.Seitz AL, McClure PW, Finucane S, et al. Mechanisms of rotator cuff tendinopathy: Intrinsic, extrinsic, or both? Clinical Biomechanics 26 (2011): 1–12. [DOI] [PubMed] [Google Scholar]
- 46.Varacallo M, El Bitar Y, Sina RE, et al. Rotator Cuff Syndrome. [Updated 2024 Mar 5]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; (2024). [PubMed] [Google Scholar]
- 47.Rajalekshmi R, Agrawal DK. Understanding fibrous tissue in the effective healing of rotator cuff injury. J Surg Res (Hous) 7 (2024): 215–228. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Darrieutort-Laffite C, Blanchard F, Soslowsky LJ, et al. Biology and physiology of tendon healing. Joint Bone Spine 91 (2024):105696. [DOI] [PubMed] [Google Scholar]
- 49.Sharma P, Maffulli N. Biology of tendon injury: healing, modeling and remodeling. J Musculoskelet Neuronal Interact 6 (2006): 181–190. [PubMed] [Google Scholar]
- 50.Mohindra R, Mohindra R, Agrawal DK, et al. Bioactive extracellular matrix fragments in tendon repair. Cell and Tissue Research 390 (2022): 131–140. [DOI] [PubMed] [Google Scholar]
- 51.Lal MR LP, Agrawal DK. Biologically enhanced patch in the healing and mechanical stability of rotator cuff tears. J Biotechnol Biomed 7 (2024): 379–386. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Snedeker JG, Foolen J. Tendon injury and repair - A perspective on the basic mechanisms of tendon disease and future clinical therapy. Acta Biomater 63 (2017): 18–36. [DOI] [PubMed] [Google Scholar]
- 53.Shadwick RE. Elastic energy storage in tendons: mechanical differences related to function and age. J Appl Physiol (1985) 68 (1990): 1033–1040. [DOI] [PubMed] [Google Scholar]
- 54.Fyfe I, Stanish WD. The use of eccentric training and stretching in the treatment and prevention of tendon injuries. Clin Sports Med 11 (1992): 601–624. [PubMed] [Google Scholar]
- 55.Mosler E, Folkhard W, Knörzer E, et al. Stress- induced molecular rearrangement in tendon collagen. J Mol Biol 182 (1985): 589–596. [DOI] [PubMed] [Google Scholar]
- 56.Sasaki N, Shukunami N, Matsushima N, et al. Time-resolved X-ray diffraction from tendon collagen during creep using synchrotron radiation. J Biomech 32 (1999): 285–292. [DOI] [PubMed] [Google Scholar]
- 57.Butler DL, Grood ES, Noyes FR, et al. Biomechanics of ligaments and tendons. Exerc Sport Sci Rev 6 (1978): 125–181. [PubMed] [Google Scholar]
- 58.Wang JH. Mechanobiology of tendon. J Biomech 39 (2006): 1563–82. [DOI] [PubMed] [Google Scholar]
- 59.Schatzker J, Brånemark PI. Intravital observations on the microvascular anatomy and microcirculation of the tendon. Acta Orthop Scand Suppl 126 (1969): 1–23. [DOI] [PubMed] [Google Scholar]
- 60.Platt MA. Tendon repair and healing. Clin Podiatr Med Surg 22 (2005): 553–vi. [DOI] [PubMed] [Google Scholar]
- 61.Vailas AC, Tipton CM, Laughlin HL, et al. Physical activity and hypophysectomy on the aerobic capacity of ligaments and tendons. J Appl Physiol Respir Environ Exerc Physiol 44 (1978): 542–546. [DOI] [PubMed] [Google Scholar]
- 62.Arndt AN, Komi PV, Brüggemann GP, et al. Individual muscle contributions to the in vivo achilles tendon force. Clin Biomech (Bristol, Avon) 3 (1998): 532–541. [DOI] [PubMed] [Google Scholar]
- 63.Benazzo F, Maffulli N. An operative approach to Achilles tendinopathy. Sports Med Arthrosc Rev 8 (2000): 96–101. [Google Scholar]
- 64.Yazdani AN, Abdi A, Patel P, et al. Mitochondrial biogenesis as a therapeutic target for rotator cuff tendon tears. J Ortho Sports Med 5 (2023): 442–449. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Fang W, Agrawal DK, Thankam FG. ‘Smart-Exosomes’: A smart approach for tendon regeneration. Tissue Eng Part B 28 (2022): 613–625. [DOI] [PubMed] [Google Scholar]
- 66.Connor DE, Paulus JA, Dabestani PJ, et al. Therapeutic potential of exosomes in rotator cuff tendon healing. J Bone Miner Metab 37 (2019): 759–767. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Thankam FG, Chandra IS, Kovilam AN, et al. Amplification of mitochondrial activity in the healing response following rotator cuff tendon injury. Sci Reports 8 (2018): 17027. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Chartier C, ElHawary H, Baradaran A, et al. Tendon: Principles of Healing and Repair. Semin Plast Surg 35 (2021): 211–215. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Thankam FG, Dilisio MF, Gross RM, Agrawal DK. Collagen I: A kingpin for rotator cuff tendon pathology. Am J Translational Res 10 (2018): 3291–3309. [PMC free article] [PubMed] [Google Scholar]
- 70.Thankam FG, Diaz C, Chandra I, Agrawal DK. Hybrid interpenetrating hydrogel network favoring the bidirectional migration of tenocytes for rotator cuff tendon regeneration. J Biomed Mater Res B Appl Biomater 110 (2022): 467–477. [DOI] [PubMed] [Google Scholar]
- 71.Thankam FG, Evan DK, Agrawal DK, Dilisio MF. Collagen type III content of the long head of the biceps tendon as an indicator of glenohumeral arthritis. Mol Cell Biochem. 454 (2019): 25–31. [DOI] [PubMed] [Google Scholar]
- 72.Thankam FG, Dilisio MF, Agrawal DK. All in one hydrogel approach: A translationally worthwhile scenario for rotator cuff tendinopathies. Trends in Biomaterials and Artificial Organs 32 (2018): 46–48. [Google Scholar]
- 73.Beredjiklian PK. Biologic aspects of flexor tendon laceration and repair. J Bone Joint Surg Am 85 (2003): 539–550. [DOI] [PubMed] [Google Scholar]
- 74.Koob TJ, Summers AP. Tendon--bridging the gap. Comp Biochem Physiol A Mol Integr Physiol 133 (2002): 905–909. [DOI] [PubMed] [Google Scholar]
- 75.BW. Tissue healing and repair: tendons and ligaments. In: Frontera WR, ed. Rehabilitation of Sports Injuries: Scientific Basis. Oxford, UK: Blackwell Science; (2003): 56–98. [Google Scholar]
- 76.Singh D, Rai V, Agrawal DK. Regulation of Collagen I and Collagen III in Tissue Injury and Regeneration. Cardiol Cardiovasc Med 7 (2023): 5–16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Holm Nielsen S, Jonasson L, Kalogeropoulos K, et al. Exploring the role of extracellular matrix proteins to develop biomarkers of plaque vulnerability and outcome. J Intern Med 287 (2020): 493–513. [DOI] [PubMed] [Google Scholar]
- 78.Riederer-Henderson MA, Gauger A, Olson L, et al. Attachment and extracellular matrix differences between tendon and synovial fibroblastic cells. In Vitro 19 (1983): 127–133. [DOI] [PubMed] [Google Scholar]
- 79.Wynn TA. Cellular and molecular mechanisms of fibrosis. J Pathol 214 (2008): 199–210. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80.Schulze-Tanzil GG, Delgado-Calcares M, Stange R, et al. Tendon healing: a concise review on cellular and molecular mechanisms with a particular focus on the Achilles tendon. Bone Joint Res 11 (2022): 561–574. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 81.Mailey B, O'Shea G, Romanelli M, et al. Systemic Immunosuppression for Prevention of Recurrent Tendon Adhesions. Plast Reconstr Surg Glob Open 9 (2021): e3834. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82.Minkwitz S, Schmock A, Kurtoglu A, et al. Time-Dependent Alterations of MMPs, TIMPs and Tendon Structure in Human Achilles Tendons after Acute Rupture. Int J Mol Sci 18 (2017): 2199. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83.Potenza AD. Tendon healing within the flexor digital sheath in the dog. J Bone Joint Surg Am 44-A (1962): 49–64. [PubMed] [Google Scholar]
- 84.Pakyari M, Farrokhi A, Maharlooei MK, et al. Critical Role of Transforming Growth Factor Beta in Different Phases of Wound Healing. Adv Wound Care (New Rochelle) 2 (2013): 215–224. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 85.Doersch KM, DelloStritto DJ, Newell-Rogers MK. The contribution of interleukin-2 to effective wound healing. Exp Biol Med (Maywood) 242 (2017): 384–396. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86.Legrand A, Kaufman Y, Long C, et al. Molecular Biology of Flexor Tendon Healing in Relation to Reduction of Tendon Adhesions. The Journal of Hand Surgery (2017): S0363502317309607. [DOI] [PubMed] [Google Scholar]
- 87.Buschmann J. Biomechanics of Tendons and Ligaments ∥ Role of cellular response in the healing process of tendons and ligaments (2017): 301–317. [Google Scholar]
- 88.Zhang C, Wu J, Li X, et al. Current Biological Strategies to Enhance Surgical Treatment for Rotator Cuff Repair. Front Bioeng Biotechnol 9 (2021): 657584. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 89.Tafti D, Schultz D. Shoulder Joint Injection. [Updated 2023 Jul 24]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; (2024). [PubMed] [Google Scholar]
- 90.Schmidt CC, Morrey BF. Management of full-thickness rotator cuff tears: appropriate use criteria. Journal of Shoulder and Elbow Surgery (2015): S1058274615002876. [DOI] [PubMed] [Google Scholar]
- 91.Moosmayer S, Lund G, Seljom U, et al. At a 10-Year Follow-up, Tendon Repair Is Superior to Physiotherapy in the Treatment of Small and Medium-Sized Rotator Cuff Tears. The Journal of Bone and Joint Surgery 101 (2019): 10501060. [DOI] [PubMed] [Google Scholar]
- 92.He HB, Wang T, Wang MC, et al. Tendon-to-bone healing after repairing full-thickness rotator cuff tear with a tripleloaded single-row method in young patients. BMC Musculoskelet Disord 22 (2021): 305. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 93.Thangarajah T, Lo IK, Sabo MT. Rotator cuff repair techniques: Current concepts. J Clin Orthop Trauma 17 (2021): 149–156. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 94.Ghodadra NS, Provencher MT, Verma NN, et al. Open, Mini-open, and All- Arthroscopic Rotator Cuff Repair Surgery: Indications and Implications for Rehabilitation. J Orthop Sports Phys Ther 39 (2009): 81–A6. [DOI] [PubMed] [Google Scholar]
- 95.Hawi N, Schmiddem U, Omar M, et al. Arthroscopic Debridement for Irreparable Rotator Cuff Tears. Open Orthop J 10 (2016): 324–329. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 96.Khoriati AA, Antonios T, Gulihar A, et al. Single Vs Double row repair in rotator cuff tears - A review and analysis of current evidence [published correction appears in J Clin Orthop Trauma 11 (2020): 1169–1171. doi: 10.1016/j.jcot.2020.09.032] [published correction appears in J Clin Orthop Trauma. 2020 Nov-Dec;11(6):1177. doi: ] [published correction appears in J Clin Orthop Trauma. 2020 Nov-Dec;11(6):1172-1174. doi: ] [published correction appears in J Clin Orthop Trauma. 2021 Aug 05;21:101557. doi:]. J Clin Orthop Trauma. 2019;10(2):236-240. doi: [DOI] [PMC free article] [PubMed] [Google Scholar]
- 97.Roth KM, Warth RJ, Lee JT, et al. Arthroscopic Single- Row Versus Double-Row Repair for Full-Thickness Posterosuperior Rotator Cuff Tears: A Critical Analysis Review. JBJS Reviews 2 (2014): e6–e6. [DOI] [PubMed] [Google Scholar]
- 98.9Murray JM, Gross L. Optimizing the management of full-thickness rotator cuff tears. J Am Acad Orthop Surg 21 (2013): 767–771. [DOI] [PubMed] [Google Scholar]
- 99.Favard L, Bacle G, Berhouet J. Rotator cuff repair. Joint Bone Spine 74 (2007): 551–557. [DOI] [PubMed] [Google Scholar]
- 100.Charousset C, Duranthon LD, Grimberg J, et al. Etude par arthroscanner de la cicatrisation tendineuse après reparation arthroscopique de la coiffe des rotateurs: analyse des facteurs predictifs à propos d'une série consécutive de 167 réparations [Arthro-C-scan analysis of rotator cuff tears healing after arthroscopic repair: analysis of predictive factors in a consecutive series of 167 arthroscopic repairs]. Rev Chir Orthop Reparatrice Appar Mot 92 (2006): 223–233. [DOI] [PubMed] [Google Scholar]
- 101.Goutallier D, Postel JM, Van Driessche S, et al. Tension-free cuff repairs with excision of macroscopic tendon lesions and muscular advancement: results in a prospective series with limited fatty muscular degeneration. J Shoulder Elbow Surg 15 2006: 164–172. [DOI] [PubMed] [Google Scholar]
- 102.Miller BS, Downie BK, Kohen RB, et al. When Do Rotator Cuff Repairs Fail? Serial Ultrasound Examination After Arthroscopic Repair of Large and Massive Rotator Cuff Tears. The American Journal of Sports Medicine 39 (2011): 2064–2070. [DOI] [PubMed] [Google Scholar]
- 103.Plachel F, Jo OI, Rüttershoff K, et al. A Systematic Review of Long-term Clinical and Radiological Outcomes of Arthroscopic and Open/Mini-open Rotator Cuff Repairs. Am J Sports Med 51 (2023): 1904–1913. [DOI] [PubMed] [Google Scholar]
- 104.Hiroyuki S, Kazuhiko M, Keisuke M, et al. Functional and Structural Outcome After Arthroscopic Full-Thickness Rotator Cuff Repair: Single-Row Versus Dual-Row Fixation 21 (2005): 1307–1316. [DOI] [PubMed] [Google Scholar]
- 105.Brochin RL, Zastrow R, Hussey-Andersen L; et al. Revision rotator cuff repair: a systematic review. Journal of Shoulder and Elbow Surgery (2019): S1058274619304641. [DOI] [PubMed] [Google Scholar]
- 106.Ferguson WJ, Field LD. Revision Rotator Cuff Repair: A Comprehensive Approach and Stepwise Technique. Arthrosc Tech 10 (2021): e1737–e1742. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 107.Parnes N, DeFranco M, Wells JH, et al. Complications after arthroscopic revision rotator cuff repair. Arthroscopy 29 (2013): 1479–1486. [DOI] [PubMed] [Google Scholar]
- 108.Cobb TE, Dimock RAC, Memon SD, et al. Rotator Cuff Repair With Patch Augmentation: What Do We Know? Arch Bone Jt Surg 10 (2022): 833–846. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 109.Chalmers PN, Tashjian RZ. Patch Augmentation in Rotator Cuff Repair. Curr Rev Musculoskelet Med 13 (2020): 561571. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 110.Di Benedetto P, Mancuso F, Tosolini L, et al. Treatment options for massive rotator cuff tears: a narrative review. Acta Biomed 92 (2021): e2021026. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 111.Avanzi P, Giudici Ld, Capone A, et al. Prospective randomized controlled trial for patch augmentation in rotator cuff repair: 24-month outcomes. Journal of Shoulder and Elbow Surgery 28 (2019): 1918–1927. [DOI] [PubMed] [Google Scholar]
- 112.Cai YZ, Zhang C, Jin RL, et al. Arthroscopic rotator cuff repair with graft augmentation of 3- dimensional biological collagen for moderate to large tears: a randomized controlled study. Am J Sports Med (2018). [DOI] [PubMed] [Google Scholar]
- 113.Ricchetti ET, Aurora A, Iannotti JP, et al. Scaffold devices for rotator cuff repair. J Shoulder Elbow Surg 21 (2012): 265. [DOI] [PubMed] [Google Scholar]
- 114.Lee GW, Kim JY, Lee HW, et al. Clinical and Anatomical Outcomes of Arthroscopic Repair of Large Rotator Cuff Tears with Allograft Patch Augmentation: A Prospective, Single-Blinded, Randomized Controlled Trial with a Longterm Follow-up. Clin Orthop Surg 14 (2022): 263–271. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 115.Hartzler RU, Softic D, Qin X, et al. The histology of a healed superior capsular reconstruction dermal allograft: a case report. Arthroscopy 35 (2019): 2950–2958. [DOI] [PubMed] [Google Scholar]
- 116.Barber FA, Herbert MA, Boothby MH. Ultimate tensile failure loads of a human dermal allograft rotator cuff augmentation. Arthroscopy. 2008; 24: 20–24. [DOI] [PubMed] [Google Scholar]