
Figure 1.
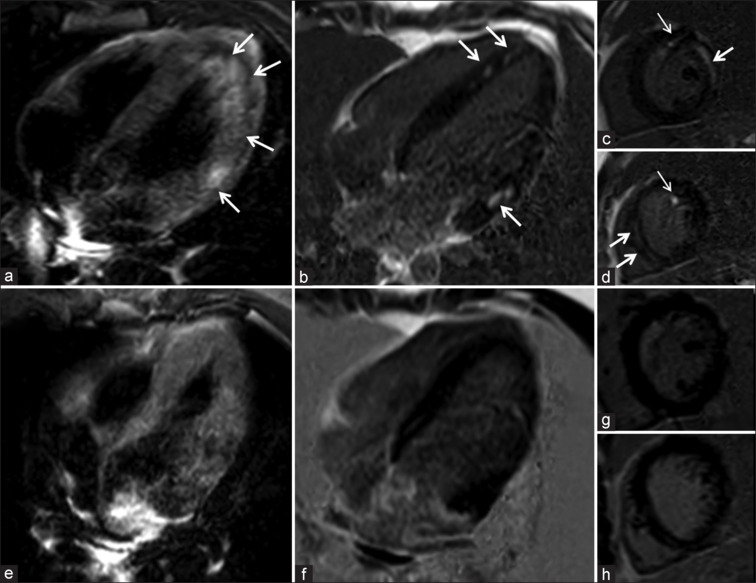
P1-A 14-year-old male patient with COVID-19 presented with sudden onset chest pain warranting admission to the emergency department. Electrographic-suggested inferior wall myocardial infarction requiring emergent catheter coronary angiography (CAA). CAA was unremarkable. Troponin levels were 4500 ng/L) a). Cardiac magnetic resonance imaging (CMR)-short-tau-inversion-recovery (STIR) horizontal long axis image shows confluent hyperintensities in LV lateral wall, apex, inferoseptum (arrows), (b-d) late gadolinium enhancement (LGE) horizontal long axis and short axis mid cavity and apex shows patches of mid myocardial enhancement co-localizing to areas of STIR hyperintensities (thick arrows). Note LGE in papillary muscle (thin arrows). Follow-up CMR images (e) STIR and LGE images (f-h) show complete resolution of abnormalities