
FIGURE 1.
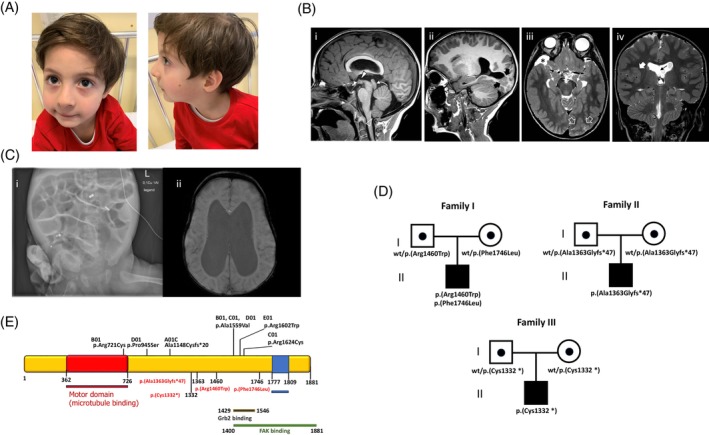
Clinical and genetic features of KIF26 patient. (A) Facial dysmorphism includes sparse eyebrows, almond‐shaped eyes, flat nasal bridge, thin lips, left mandibular hypoplasia with retrognathia, left‐sided helix hypoplasia, and bilateral lobe hypoplasia. (B) Brain MRI of the patient 1# performed at 6.5 years of age; (Bi–ii) Sagittal T1‐weighted images demonstrate cerebral aqueduct stenosis (curved arrow) associated with a small anterior commissure (dashed arrow) and hypothalamic adhesion (full arrowhead). There are several nodules of gray matter heterotopia extending from the parieto‐occipital cortex to the ventricle (thick black arrows). Note the caudal displacement of the cerebellar tonsils (empty arrowhead). (Biii) Axial T2‐weighted image shows bilateral incomplete hippocampal rotation. Note that the cortex overlying the nodular heterotopias is abnormal, showing a focal area of polymicrogyria (empty white arrows). (Biv) coronal T2‐weighted image depict enlargement of the lateral ventricles associated with focal fenestration of the septum pellucidum (thin black arrow). There is an additional area of polymicrogyria in the left insula (thick white arrow). (C) Brain MRI in patient #2: Hydrocephalus with obliterated aqueduct, hypoplasia of corpus callosum, agenesis of septum pellucidum. (Ci) x‐say: Intestinal dilatation due to distal obstruction. (Cii) Brain MRI: Dilatation of lateral. (D) Pedigree of the families showing the segregation of KIF26A variants in the proband and healthy parents. (E) Localization of previously reported (black) and novel (red) KIF26 variant in the protein.