
Figure 2: Clinical features and radiological findings of anti-melanoma differentiation-associated gene 5 syndrome.
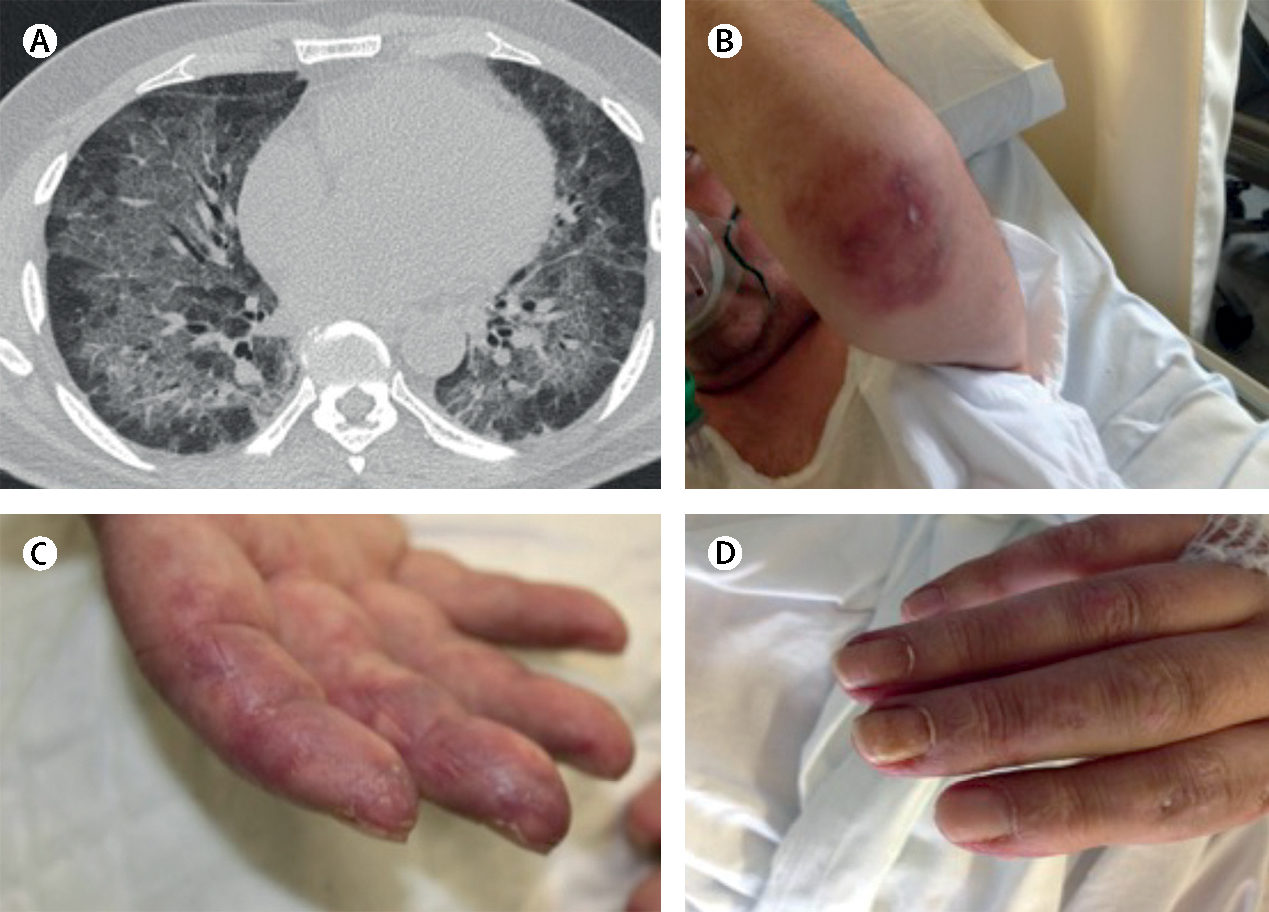
A man aged 52 years presented with progressive dyspnoea that had been present for 2 months. At the emergency room, he was hypoxemic with a ratio of arterial oxygen partial pressure to fractional inspired oxygen of less than 300 (normal >500). The patient was positive for high concentrations of anti-melanoma differentiation-associated gene-5 autoantibodies . (A) A high-resolution chest CT scan showed alveolar infiltrate in both lungs. Infectious and neoplastic causes were ruled out. (B) Characteristic skin lesion ulcer on elbow, (C) fingers suggesting vasculopathy , and (D) erythematous skin changes due to dermatomyositis. The patient was intubated and mechanic ventilation was started at the intensive care unit. After treatment with polymyxin-B haemoperfusion, glucocorticoids, tacrolimus, plasmapheresis, and intravenous immunoglobulin, the patient’s general condition improved to the extent that the orotracheal tube was withdrawn and he was discharged to a conventional ward.