

Abstract
Objective
To assess the effect of electrically heated mittens on physical hand function in people with osteoarthritis of the hands compared with control mittens.
Design
Randomised controlled trial.
Setting
Osteoarthritis outpatient clinic, Copenhagen, Denmark.
Participants
200 people with hand osteoarthritis aged 42-90 years. 100 participants were assigned to the intervention group and 100 to the control group.
Interventions
Electrically heated mittens or control mittens (heating elements disconnected) worn for at least 15 minutes daily for six weeks.
Main outcome measures
The primary outcome was change in hand function measured on the function subscale of the Australian/Canadian hand osteoarthritis index (AUSCAN; score 0-100 points) at six weeks. Key secondary outcomes included changes in the AUSCAN hand pain subscale (score 0-100 points), global rating of hand osteoarthritis related problems (0-100 visual analogue scale), and grip strength (newtons) at six weeks. Analysis of secondary outcomes was performed using a hierarchical gatekeeping approach.
Results
91 participants in the intervention group and 95 in the control group completed the trial. The mean age of participants was 71 years, 87% (n=173) were women, and mean body mass index was 24.9 (SD 4.4). Median disease duration was 10 years (interquartile range 5-15 years). The between group difference for change in AUSCAN function at week 6 was 3.0 points (95% confidence interval (CI) −0.4 to 6.3; P=0.09) in favour of heated mittens. For the key secondary outcome, change in AUSCAN hand pain score from baseline, a group difference was observed of 5.9 points (95% CI 2.2 to 9.5) in favour of heated mittens. Changes in global rating of hand osteoarthritis related problems and grip strength did not differ between the groups with an observed difference between groups of 2.8 points (95% CI −3.7 to 9.2) and 2.3 newtons (95% CI −16.3 to 21.0) in favour of heated mittens, respectively.
Conclusion
Use of electrically heated mittens for six weeks was not related to a positive change in physical hand function compared with control mittens. Heated mittens provided no additional benefits on global rating of hand osteoarthritis related problems and grip strength. A small benefit was detected for hand pain, but this could have been overestimated.
Trial registration
ClinicalTrials.gov NCT04576403.

Introduction
Osteoarthritis of the hands is a common, age related joint disease that primarily affects the first carpometacarpal and distal interphalangeal joints of the second to fifth fingers.1 Symptomatic hand osteoarthritis affects 16% of women and 8% of men aged 40-84 years, and incidence increases with age.2 3 People with hand osteoarthritis experience pain, impaired physical function, and reduced health related quality of life.4 5 6 Treatments are limited and include non-drug, drug, and surgical interventions, all of which have been shown to have small to moderate effects.7 8 Oral non-steroidal anti-inflammatory drugs are widely recommended and used to treat the symptoms of osteoarthritis but have considerable toxicity,9 especially among elderly people with comorbidities. With the ageing population and limited effectiveness and safety of current common interventions, effective and safe treatments for the symptoms of hand osteoarthritis are needed.
Heat therapy has a long tradition in the management of arthritis and has been studied in various forms, including paraffin baths,10 11 12 13 mud packs,14 warm baths,15 infrared radiation,16 and low dose radiation therapy.17 The mechanisms for symptomatic relief from heat are not fully understood, but heat therapy has been shown to increase blood flow and oxygen and nutrient supply to joints and surrounding tissues.18 Systematic reviews looked at the effect of these treatments, with the overall conclusion that a symptom moderating effect was possible.19 20 21 In the 2020 American College of Rheumatology guidelines for the management of hand osteoarthritis, heat was recommended as a symptom moderation tool. The recommendation was conditional based on the limited number and low methodological quality of the underlying randomised controlled trials.7 In line with this, no consensus on the use of heat was found in a systematic review of 11 clinical practice guidelines for the treatment of osteoarthritis.22
Current heat therapies can be considered impractical, as they require specialised equipment and time consuming visits to clinics or other specialised facilities. However, mittens with inbuilt battery driven heat elements are now commercially available and offer an easy means of delivering heat therapy to patients with hand osteoarthritis in an accessible manner outside of clinics. The use of heated mittens as a symptom moderation tool to treat hand osteoarthritis has never been tested.
In this trial, we assessed the effect of electrically heated mittens on core outcomes in people with hand osteoarthritis, including hand function and other important symptoms, compared with control mittens (heating elements disconnected). We hypothesised that wearing heated mittens would result in greater improvement in hand function and relief of symptoms than wearing control mittens in people with hand osteoarthritis.
Methods
Design
This was a randomised controlled trial with two parallel groups and outcomes assessed at baseline and repeated after two, four, and six weeks (primary outcome). All participants provided signed informed consent before trial participation.
Participants visited the clinic twice—at baseline and after six weeks, with the intervention delivered between these visits. At two and four weeks, the participants were telephoned to resolve any difficulties with the mittens, remind them to fill out a diary of mitten and analgesics’ use, and administer an online questionnaire. These questionnaires were delivered by secure email using a web based electronic data capturing system (REDCap).23 24
At the screening and baseline visits, the participants were informed that the aim of the trial was to assess if it would be beneficial to wear heated mittens for hand osteoarthritis. The participants were told that they would receive a pair of mittens, either with or without heat (control treatment).
The six week intervention was restricted to the coldest months in Denmark (1 October to 31 March) on the basis that any potential benefits of heat would be more noticeable during this period. Consequently, the trial was completed in the winter seasons of 2020-21, 2021-22, and 2022-23.
Participants
We recruited participants from the osteoarthritis outpatient clinic at Copenhagen University Hospital Bispebjerg and Frederiksberg, Denmark, through advertisements via the Danish arthritis patient association and through the local newspaper. Recruitment was from October 2020 until January 2023.
Participants were considered eligible for inclusion if they met the American College of Rheumatology classification criteria for hand osteoarthritis, defined as hand pain and difficulties in hand function during the previous four weeks and at least three of the following: hard tissue enlargement of two or more of the 10 selected joints, fewer than three swollen metacarpophalangeal joints, and deformity of at least one of the 10 selected joints. The 10 selected joints were the second and third distal interphalangeal joints, the second and third proximal interphalangeal joints, and the first carpometacarpal joints in both hands.25 Participants also had to have an Australian/Canadian hand osteoarthritis index26 (AUSCAN) function subscale score of ≥40 points (normalised 0-100 points; 100 worst). Key exclusion criteria included other diseases affecting the hand joints (eg, rheumatoid arthritis, psoriatic arthritis, neuropathy), widespread or generalised pain syndrome (eg, fibromyalgia), and steroid injections in the finger joints within the past month. A rheumatologist or doctor assessed the criteria for participation at the baseline visit. The eligibility criteria are described in detail in the trial protocol (see supplementary file).
Interventions
Participants received a pair of mittens at the end of the baseline visit and were asked to wear them for at least 15 minutes daily during the six week trial period, preferably when symptoms were worst (typically in the morning).27 The minimum wear time of 15 minutes was primarily based on patients’ reference to morning stiffness and pain, together with clinical experience. A study suggested that peak skin temperature is reached after 15 minutes.28
The mittens used in this trial are commercially available (Nordic Heat, Denmark). The heating element in the mittens was placed on the dorsal side, providing heat primarily to the back of the hands and fingers. Heat intensity, which could be adjusted using a button on top of each mitten, was indicated by an LED (light emitting diode) light, with red, yellow, and green denoting maximum, medium, and low heat, respectively.
The wiring from the battery to the heating element in the control mittens was disconnected, but the LED light remained active and could react to the button being pushed. The mittens were available in four sizes—small, medium, large, and extra large—and a secretary at the clinic supplied participants with the appropriate size. The supplementary file shows the mittens.
To optimise treatment adherence, all participants received a diary and were requested to note daily wear time (date, number of times, duration of each use (minutes), and applied intensity (red, yellow, or green LED light). The importance of wearing the mittens and noting wear time in the diary was emphasised.
One of three physiotherapists, masked to treatment group, provided participants with the same instructions. These instructions were based on a rehearsed protocol, and the physiotherapists took part in frequent group discussions to ensure that participants were given similar information. Between them, the physiotherapists had 12 to 33 years’ experience.
Randomisation and masking
After baseline measurements had been obtained, we randomised participants in a 1:1 ratio based on permuted random blocks of variable sizes (2-6 in each block) generated before enrolment. A biostatistician (RC) not involved in recruitment or data collection, prepared and uploaded the randomisation list into the REDCap database. Allocation was concealed until participants had completed baseline assessments, and a masked third party (a secretary) assigned a pair of mittens to each participant using an electronic trial management system. The mittens were coded A or B to conceal the allocation from participants, clinical and non-clinical staff, and outcome assessors. The participants were aware that the purpose of the study was to compare mittens with or without heat. Masking was maintained until the trial database was locked and all analyses (see supplementary file for statistical analysis plan) had been done and interpreted. Successful masking of participants was assessed by asking them to guess their group allocation at two and four weeks and after six weeks.
Outcome measures
Primary outcome
The primary outcome was change in the AUSCAN function subscale from baseline to after six weeks (ie, week 7 from allocation),26 29 as recommended by our patient research partners and the stakeholders from the Outcome Measures in Rheumatology (OMERACT) initiative.30 AUSCAN is a validated questionnaire comprising 15 items divided into three subscales assessing function (nine items), stiffness (one item), and pain (five items) during the past 48 hours. The questionnaire concerns both hands, with validation limited to people who are right hand dominant.23 We used the Danish version of AUSCAN with a 0-100 mm visual analogue scale format, with lower scores indicating better function, less stiffness, and less pain. Each subscale score was normalised to a score of 0-100 points (0 better; 100 worst). The questionnaire is copyrighted, but further information is available at www.womac.com. Currently, no estimate of a minimal important difference exists.
Secondary outcomes
The main secondary outcome was change from baseline to more than six weeks in the pain subscale of AUSCAN, patient global rating of hand related problems using a 0-100 mm visual analogue scale (0 indicating no problems), and bilateral measures of grip strength using a dynamometer (Grippit; Detektor, Gothenburg, Sweden).31
Other secondary outcomes were changes from baseline to more than six weeks in the stiffness subscale of AUSCAN, tender joint count, swollen joint count, hand pain (0-100 mm visual analogue scale; 0 indicating no pain), number of participants who stopped using analgesics, as well as treatment response according to the OMERACT-Osteoarthritis Research Society International (OARSI) response criteria (≥50% and ≥20 points absolute improvement in AUSCAN pain or function subscales, or at least two of the following: ≥20% and ≥10 points absolute improvement in AUSCAN pain, AUSCAN function, or patient global assessment).30 The use of analgesics and OMERACT-OARSI response criteria were not prespecified in the protocol but were added to the a priori statistical analysis plan. All data are presented in this paper.
The AUSCAN questionnaire was administered at baseline, two and four weeks, and after six weeks. All other outcomes were assessed at baseline and after six weeks. A doctor or physiotherapist performed the tender and swollen joint counts using the European Alliance of Associations for Rheumatology handbook32 in a binary manner (yes or no). The assessment included bilateral examination of 16 joints of the hands: Wrist, first carpometacarpal and interphalangeal joints, first to fifth metacarpophalangeal joints, and proximal and distal interphalangeal joints. The tender and swollen joint counts each ranged from 0 to 32 or from 0 to 30, when scoring of the wrist was omitted. Information on participants’ use of analgesis was obtained at the baseline visit, when they were requested to keep a diary of their weekly use of analgesics during the six week intervention period.
Adverse events
Adverse events were recorded on the basis of spontaneous reports during telephone interviews with the participants at two and four weeks, and at the clinic visit after six weeks. An adverse event was defined as any problem experienced during trial participation. A doctor assessed the association between an adverse event and mitten use.
Sample size
No minimal important difference for the AUSCAN function score existed to inform the sample size calculation. The power calculation was based on a two sample pooled t test for the normal mean difference, with a two sided significance level of 0.05 (P<0.05), assuming a standard deviation of 1933 34 in AUSCAN function scores, and 180 participants providing 80.2% power to detect an 8 point mean difference in AUSCAN function scores. After accounting for potential dropouts, we determined that we would need a total of 200 participants.
Statistical analysis
The statistical analysis was performed according to the a priori statistical analysis plan that was finalised and closed before the last participant’s final visit (see supplemental file for details). Baseline information is presented as means and standard deviations (SDs) for normally distributed data and as medians and interquartile ranges (IQRs) for skewed data. Dichotomous and categorical data are presented as numbers and proportions.
The primary analysis was performed using the intention-to-treat population—that is, participants were assessed and analysed according to the group to which they had been randomised, irrespective of adherence to the treatment. Continuous outcomes with repeated measures (ie, AUSCAN pain, function, and stiffness subscales) were analysed using repeated measures mixed linear models, including participants as random effects, with fixed effect factors for group and week and the corresponding interaction, while adjusting for baseline values.35 Results are reported as least squares means and standard errors (SEs), and differences between least squares means are reported with two sided 95% confidence intervals (CIs). In the intention-to-treat analysis, we used repeated measurements mixed linear models to handle missing data. Continuous data, measured only at baseline and after six weeks, were analysed using analysis of covariance models, with group as fixed effect factor adjusted for the baseline value. For these measures not collected as repeated measures, missing data were handled using multiple imputation with chained equations (100 imputations).36 Numbers of responders to OMERACT-OARSI and participants who stopped analgesics are presented as numbers and simple proportions for each group (as observed; no imputation of missing data) with risk difference based on the intention-to-treat population and missing data handled using multiple imputation with chained equations (100 imputations).36 No explicit adjustments for multiplicity were applied—rather the statistical analysis plan prespecified that the key secondary outcome measures were analysed and interpreted in a prioritised order using a gatekeeping approach to minimise false positives.37
Two sensitivity analyses were performed. Firstly, we repeated the primary analyses with missing data after six weeks replaced with the baseline values (ie, a non-responder imputation). Secondly, we performed the analyses based on the per protocol population, predefined as participants who reported mitten use of at least 15 minutes daily for at least 30 days and had no major protocol violations (defined as primary outcome assessment 43 to 50 days from baseline, major surgery, hand surgery, steroid injections, or use of oral steroids during the trial participation period).
Adherence data are presented as the average minutes daily with SD for each group, with mean group differences and 95% CIs for total mitten usage (in minutes) and days of mitten use. The frequency of mitten use (number of times mittens were used daily) is reported as medians with ranges and most frequently reported frequency. Mitten intensity (red, yellow, green LED light) was calculated as proportion (percentage) of use. The masking assessment was analysed using agreement statistics (κ) comparing the participants’ guesses with their actual allocation. The statistical analysis was performed using R (version 4.0.3) and SAS studio.
Patient and public involvement
A group interview with four patient research partners was carried out to inform the choice of outcomes in this trial. One patient research partner took part in the development of the protocol. The patient research partners acknowledged the idea and purpose of the trial and participated in the discussion of the feasibility of the investigational programme. The patient research partners have worked voluntarily and have been offered co-authorship of trial related publications according to the recommendations of the International Committee of Medical Journal Editors criteria. The patient research partners also read and approved this manuscript.
Results
Participant characteristics
Between 26 October 2020 and 12 January 2023, a total of 309 participants were assessed for eligibility. Overall, 200 participants were enrolled and randomised: 100 to heated mittens and 100 to control mittens. Ninety one participants in the intervention group and 95 in the control group completed the trial (fig 1). The mean age of participants was 71 years, 87% (n=173) were women, and mean body mass index was 24.9 (SD 4.4). Median disease duration was 10 years (IQR 5-15 years). The personal characteristics and outcomes of the two groups were well balanced at baseline (table 1).
Fig 1.

Flow of participants in study. ACR=American College of Rheumatology; AUSCAN=Australian/Canadian hand osteoarthritis index
Table 1.
Baseline characteristics in intention-to-treat population. Values are mean (standard deviation) unless stated otherwise
| Characteristics | Heated mittens (n=100) | Control mittens (n=100) | Total (n=200) |
|---|---|---|---|
| Age (years) | 72 (8.8) | 71 (9.7) | 71 (9.2) |
| No (%) female | 86 (86) | 87 (87) | 173 (87) |
| Height (m) | 166.2 (8.4) | 166.1 (8.8) | 166.1 (8.6) |
| Weight (kg) | 70.3 (14.7) | 67.6 (12.4) | 68.9 (13.7) |
| Body mass index | 25.4 (4.9) | 24.4 (3.8) | 24.9 (4.4) |
| Median (IQR) disease duration (years) | 10 (6.5-19) | 10 (5-15) | 10 (5-15) |
| AUSCAN scores (0-100) | |||
| Function* | 68.9 (15.6) | 67.6 (14.7) | 68.2 (15.1) |
| Pain | 63.9 (16.9) | 64.4 (15.5) | 64.1 (16.2) |
| Stiffness | 66.4 (22.1) | 68.0 (19.6) | 67.2 (20.8) |
| Clinical assessments | |||
| Median (IQR) tender joint count (0-32) | 4.5 (2-10) | 5.0 (2-8) | 5.0 (2-9) |
| Median (IQR) swollen joint count (0-32) | 2.5 (1-6) | 3.0 (1-6) | 3.0 (1-6) |
| No (%) by 1st CMC dislocations (0-2): | |||
| 0 | 54 (54) | 62 (62) | 116 (58) |
| 1 | 8 (8) | 7 (7) | 15 (8) |
| 2 | 38 (38) | 31 (31) | 69 (35) |
| Visual analogue scales (0-100) | |||
| Hand pain | 62.7 (18.6) | 64.3 (17.9) | 63.5 (18.2) |
| Global rating of hand osteoarthritis related problems | 44.6 (26.2) | 49.9 (23.5) | 47.2 (24.9) |
| Performance measure: Grip strength (newtons) | |||
| Right hand | 133.9 (65.9) | 136.3 (64.1) | 135.1 (64.8) |
| Left hand | 128.7 (63.9) | 124.3 (64.4) | 126.5 (64.0) |
| Analgesics | |||
| No (%) using analgesics | 42 (42) | 50 (50) | 92 (46) |
| Type of analgesic (No (%))†: | |||
| Paracetamol | 37 (37) | 45 (45) | 82 (41) |
| NSAID | 11 (11) | 20 (20) | 31 (15.5) |
| Other | 9 (9) | 8 (20) | 17 (8.5) |
AUSCAN=Australian/Canadian osteoarthritis hand index; CMC=carpometacarpal; IQR=interquartile range; NSAID=non-steroidal anti-inflammatory drug.
Primary outcome measure.
Participants who reported taking paracetamol, NSAID, or other analgesics regularly (2-3 times weekly, almost daily, or daily).
Out of the 42 possible days participants were asked to wear the mittens, the mean number of reported days was 38 (SD 10.8) for the intervention group and 37 (12.0 SD) for the control group, with a group difference in self-reported mittens use of 1 day (95% CI 2.5 to 3.8 days) in favour of the intervention group. The median number of times the mittens were used daily was 1 (range 0-4) in the intervention group and 1 (range 0-3) in the control group. The mean daily wear time was 37 minutes (SD 20 minutes) in the intervention group and 25 (SD 15) minutes in the control group, with a group difference in daily wear time of 11.9 minutes/day (95% CI 6.8 to 17.1) in favour of the intervention group. The number of days the participants adhered to the protocolised wear time of a minimum 15 minutes daily was 36 (SD 10.7) days in the intervention group and 34 (SD 12.6) days in the control group. The most frequently used intensity was high (red LED light) in both groups (intervention group: 93% of the time; control group: 89% of the time).
Primary outcome
Both groups showed improvements in the primary outcome of change in the AUSCAN function subscale score from baseline to after six weeks (table 2). The mean between group difference was 3.0 points (95% CI −0.4 to 6.3; P=0.09), potentially in favour of the heated mittens. Figure 2 shows the trajectories of the AUSCAN function subscale over the six weeks.
Table 2.
Changes from baseline in primary and key secondary outcomes after six weeks in intention-to-treat population. Values are least squares mean (standard error) unless stated otherwise
| Heated mittens (n=100) | Control mittens (n=100) | Between group difference (95% CI) | P value | |
|---|---|---|---|---|
| Primary outcome | ||||
| AUSCAN function (score 0-100) | −6.3 (1.2) | −3.3 (1.2) | 3.0 (−0.4 to 6.3) | 0.09 |
| Key secondary outcomes | ||||
| AUSCAN pain (score 0-100) | −8.2 (1.3) | −2.3 (1.3) | 5.9 (2.2 to 9.5) | – |
| Global rating of hand osteoarthritis related problems (VAS score 0-100) | −3.2 (2.3) | −0.4 (2.2) | 2.8 (−3.7 to 9.2) | – |
| Grip strength: | ||||
| Right hand (newtons) | 8.0 (7.3) | 5.7 (5.8) | 2.3 (−16.3 to 21.0) | – |
| Left hand (newtons) | 11.4 (7.7) | 6.7 (5.9) | 4.7 (−14.1 to 23.5) | – |
| Other secondary outcomes | ||||
| AUSCAN stiffness (score 0-100) | −9.3 (1.7) | −3.0 (1.7) | 6.3 (1.6 to 11.1) | – |
| Tender joint count (0-30) | 2.4 (1.0) | 3.5 (0.9) | 1.2 (−1.5 to 3.8) | – |
| Swollen joint count (0-30) | −1.2 (0.6) | −1.5 (0.4) | −0.3 (−1.8 to 1.3) | – |
| Hand pain (VAS score 0-100) | −7.9 (2.2) | −3.3 (2.1) | 4.6 (−1.5 to 10.7) | – |
Continuous outcomes with repeated measures (ie, AUSCAN subscores) were analysed using linear mixed models with group and week, and their interaction as factors, and the baseline value as covariate. Missing data were handled implicitly by the mixed model. Continuous outcomes without repeated measures were analysed using an analysis of covariance model with group as factor, and the baseline value as covariate. Missing data were handled using multiple imputation and estimates were pooled across 100 imputed datasets.
Key secondary outcomes were analysed in prioritised order—a gatekeeping procedure.
Group estimates are reported as simple numbers and proportions as observed, and the difference between groups is risk difference based on multiple imputed data. To ease interpretation of between group differences, positive values are reported when in favour of heated mittens and negative values when in favour of control mittens.
AUSCAN=Australian/Canadian Osteoarthritis Hand Index; CI=confidence interval; VAS=visual analogue scale.
Fig 2.
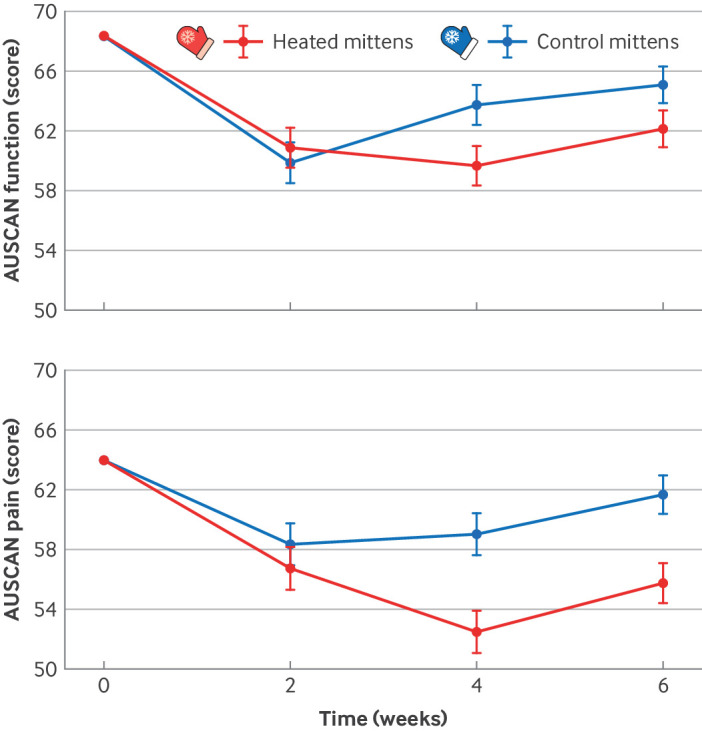
Trajectories from baseline to six weeks’ follow-up for primary efficacy outcome measure (AUSCAN function) and key secondary outcome (AUSCAN pain) in intention-to-treat population. AUSCAN=Australian/Canadian osteoarthritis hand index
Secondary outcomes
For the key secondary outcomes, a group difference was observed from baseline in AUSCAN pain score of 5.9 points (95% CI 2.2 to 9.5) in favour of the intervention group. Figure 2 shows the trajectories of AUSCAN pain score over the six weeks. No difference was observed for the other key secondary outcomes—global rating of hand osteoarthritis related problems and grip strength. Among the other secondary outcomes, a group difference in change from baseline in AUSCAN stiffness score of 6.3 points (95% CI 1.6 to 11.1) was observed in favour of the intervention group (table 2). After six weeks, 26 participants (26%) in the intervention group and 21 (24%) in the control group met the OMERACT-OARSI responder criteria.
At baseline, 42 (42%) participants in the intervention group and 50 (50%) in the control group used analgesics. After six weeks, 15 (36%) participants in the intervention group and 23 (46%) in the control group reported stopping analgesics, corresponding to a risk difference of −0.10 (95% CI −0.30 to 0.10). The remaining secondary outcomes were all in favour of the intervention group but with no significant between group differences (table 2). The prespecified sensitivity analyses confirmed the robustness of the primary analyses (see supplementary file tables 1 and 2).
Adverse events
A total of three adverse events were reported; all in the intervention group: one participant had elective hand surgery during the trial period (not related to intervention), one broke a hand (not related), and one experienced itching (resulting from mitten use).
Masking of participants
Group allocation was correctly guessed by 166 (83%) participants at two weeks, 164 (82%) at four weeks, and 181 (91%) at six weeks. The corresponding number of participants who did not provide a guess was 17 (9%), 23 (12%), and 13 (7%). The κ statistic at two weeks (κ=0.8), four weeks (κ=0.8), and six weeks (κ=0.9) suggested that masking was not successful.
Discussion
This trial found no statistically significant difference between heated mittens and control mittens after six weeks’ use on the AUSCAN function subscale in patients with hand osteoarthritis. For the secondary outcomes it appeared that heated mittens might provide minor benefits in the AUSCAN pain and stiffness subscales. No difference between groups was observed for the remaining outcomes (symptoms, grip strength, tender joint count, and swollen joint count).
The lack of difference in function between groups has also been observed in other studies assessing heat as a form of treatment.19 20 21 Despite the scarce evidence of small beneficial effects, however, heat is recommended because of its safety and simplicity of use.
A difference was observed for the secondary outcomes of pain and stiffness; however, as masking was unsuccessful these observed differences should be interpreted with caution owing to the risk of the effect being overestimated, particularly when using patient reported outcomes.38 We have identified studies with control groups or heat as a supplement to an existing treatment but not studies comparing heat with sham treatment. Studies using low level laser therapy39 or low dose radiation therapy17 have been performed with successful masking,17 but with small effects at best.19 20
Although both groups in the current study used the mittens for a similar number of days according to the prespecified wear time of 15 minutes/day (36 days for heated mittens, 34 for control mittens), mean daily wear time differed by 11.9 minutes/day between the groups. The difference could be a result of the control group being less inclined to wear the mittens owing to unsuccessful masking. In clinical meetings, many participants expressed a positive experience from use of heat. It is therefore reasonable to assume that participants allocated to the intervention group were more enthusiastic about the mittens, which also could have contributed to an overestimation of the true effect.
Skin temperature typically peaks after about 15 minutes when hot packs are applied,28 suggesting that wear time of more than 15 minutes may be necessary to elicit symptom moderating effects. In the present trial, mean wear time was 37 minutes in the intervention group and 25 minutes in the control group, suggesting that the mittens were worn for a sufficient time to elicit a potential effect.
The six week intervention period was chosen based on experience from studies of other non-drug interventions in osteoarthritis, such as exercise, where the main improvements in symptoms occur over the initial six week period.40 As patients with hand osteoarthritis often experience symptoms for years (in this trial an average of 10 years), the intervention period might have been too short to observe a change in function.
Our patient research partners chose the primary outcome. During their discussions, concerning the most important outcome, both pain and function were highlighted as being almost equally important; however, function was ultimately chosen. As both pain and function are listed as core outcomes in osteoarthritis41 and important domains for patients,42 function seemed an appropriate primary outcome. Currently, no optimal treatment for the symptoms of hand osteoarthritis exists. Both drug and surgical treatments offer some benefit but are also associated with important harms,9 43 44 45 and therefore treatments that can alleviate the symptoms of hand osteoarthritis are much needed. Only one adverse reaction (itching) was recorded in association with the mittens, so the use of electrically heated mittens seems to be safe. Furthermore, in contrast with previously examined heat treatments, the heated mittens are easily transportable and can be used in patients’ homes.
Strengths and limitations of this study
The strengths of this trial include the relatively large sample size and its methodological and rigorous conduct, which is required in the specialty of research into the management of hand osteoarthritis.20 The use of control mittens with the heating elements disconnected, in contrast with no intervention, is also a strength of our design.
It was not possible to mask the participants throughout the trial, which is a major limitation. This is not surprising as heated mittens would become warmer shortly after switching on the heating element, and the control mittens would not, despite the LED lights being active. Unsuccessful masking and use of patient reported outcomes could have led to an overestimation of effects,38 which is an inherent weakness and challenge when assessing effects of physical treatments in clinical trials. Notwithstanding, participants adhered to the protocol, indicating that use of mittens is possible. The adverse events were reported spontaneously, which might have resulted in an underestimation of occurence. However, participants were asked at two and four weeks and at the final visit after six weeks if they had experienced problems with the mittens.
It is also worth noting that we did not record unilateral or bilateral involvement of the hands, which might have influenced the outcomes, although the AUSCAN questionnaire does relate to both hands. Furthermore, although we asked participants to wear the mittens on both hands, we did not ask if they had adhered to this instruction.
We powered our trial for detecting an 8 point difference in our primary outcome of score on the AUSCAN function subscale, which might have been overly ambitious. The minimal clinically important change (used for individual patients or within group changes) for AUSCAN function has been estimated to be 4 points (on a 0-100 scale),46 and no robust estimates of minimal clinically important differences (used for group comparisons) exist, except for an estimated decrease of 8 points.47 The minimal clinically important difference for improvement is likely smaller than our target of 8 points, and therefore it is possible that our trial was underpowered for detecting small but potentially clinically relevant between group differences.
Practice implications
The high adherence to mitten use in both groups suggests that mittens could be used for some symptomatic relief in this patient population. The study mittens were designed for outdoor sports use, not for the treatment of hand osteoarthritis. Several participants reported that the mittens were too big, although different sizes were available. This discrepancy in size might have increased the distance from the heating elements to the finger joints, possibly resulting in less effective heating. Some participants did report that a more concentrated heat around the joints would have been preferable. Furthermore, the batteries required regular charging, and some participants found this cumbersome. This feature is especially relevant for people with hand osteoarthritis, and it is possible the inconvenience led to less mitten use among some participants. Developing mittens specifically for people with hand osteoarthritis, with a better, possibly customised fit and easier battery recharging system, might help to enhance the effect of heated mittens.
Heat is recommended as treatment for hand osteoarthritis, and mittens may be a feasible means of delivering heat therapy. However, the results from this trial show that electrically heated mittens do not provide additional benefits for people with symptoms of hand osteoarthritis over standard mittens. Future studies on heat treatment for hand osteoarthritis should focus on optimal masking of participants.
Conclusion
Use of heated mittens for six weeks was not related to a positive change in physical hand function compared with control mittens. For the key secondary outcomes, a difference was observed for hand pain, but not for global rating of hand osteoarthritis related problems and grip strength. As masking was unsuccessful and no effect was observed for the primary endpoint, the difference observed for pain is likely to have been overestimated. Only one adverse event (itching) was reported, suggesting mittens are safe to use for the treatment of hand osteoarthritis.
What is already known on this topic
Hand osteoarthritis is common and causes pain and reduced function
Existing treatments have small to moderate effects
Heat is conditionally recommended as a symptom moderation tool, but the supporting evidence is of low quality
What this study adds
Electrically heated mittens used daily for six weeks were not associated with additional improvements in the primary outcome of hand function compared with control mittens (heating elements disconnected)
Nor did the heated mittens provide additional benefits in global rating of hand osteoarthritis related problems and grip strength
A small additional benefit was detected for hand pain, but this was likely overestimated
Acknowledgments
We thank the patients who participated in the development of the trial protocol (interview and reading the protocol and commenting) and a special thanks to Karen Hjerdem for commenting on the results from this trial. The protocol was prospectively registered on www.clinicaltrials.gov on 5 October 2020 (NCT04576403) before inclusion of the first participant.
Web extra.
Extra material supplied by authors
Supplementary information: Protocol, pictures of the mittens, statistical analysis plan, protocol violation, and tables S1 and S2
Contributors: KE, HB, and BDS conceptualised the trial. KE, CB, MH, RC, SMN, AD, ZS, HB, KH, and BDS took part in writing and reviewing the manuscript. KE, CB, AD, ZS, and HB collected the clinical data. Primary analysis was performed by RC and SMN. All authors have read and approved the final manuscript. KE, HB, and CB are guarantors and accept full responsibility for the work and/or the conduct of the study, had access to the data, and controlled the decision to publish. The corresponding author attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted.
Funding: This trial was supported by the Danish Rheumatism Association (R192-A6735), Bispebjerg and Frederiksberg Hospital research foundation, A.P. Møllers fond (L-2021-00234). The Parker Institute is supported by a core grant from the OAK foundation (OCAY-18-774). The funding partners had no part in the planning, execution, or interpretation of this trial.
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/disclosure-of-interest/ and declare: Financial support was received from the Danish Rheumatism Association, Bispebjerg and Frederiksberg Hospital, A.P. Møllers fond for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years except for MH who declares relationship with Thuasne group and Osteoarthritis Research Society International; no other relationships or activities that could appear to have influenced the submitted work.
Transparency: The lead author (the manuscript’s guarantor) affirms that the manuscript is an honest, accurate, and transparent account of the trial being reported; that no important aspects of the trial have been omitted; and that any discrepancies from the trial as planned (and, if relevant, registered) have been explained.
Dissemination to participants and related patient and public communities: We plan to communicate the trial results to the trial participants at a dedicated participant debriefing meeting to be held at our institution by invitation. The results will be disseminated through an open access publication at The BMJ. We plan to share the findings with appropriate audiences, such as researchers, clinicians, and the general public, through various channels, including meetings of patient organisations, scientific conferences, and social media.
Provenance and peer review: Not commissioned; externally peer reviewed.
Ethics statements
Ethical approval
This project was deemed exempt from approval by the local Health Research Ethics Committee (ref: 20020569) and did not require approval from the Danish Medical Equipment Board (ref: 2020030890). The project was approved by the Danish Data Security Agency before the patients first visit (ref: P-2020-670).
Data availability statement
Data will be made available upon reasonable request to the corresponding author at cecilie.bartholdy.skjaldgaard@regionh.dk.
References
- 1. Zhang Y, Niu J, Kelly-Hayes M, Chaisson CE, Aliabadi P, Felson DT. Prevalence of symptomatic hand osteoarthritis and its impact on functional status among the elderly: The Framingham Study. Am J Epidemiol 2002;156:1021-7. 10.1093/aje/kwf141. [DOI] [PubMed] [Google Scholar]
- 2. Oliveria SA, Felson DT, Reed JI, Cirillo PA, Walker AM. Incidence of symptomatic hand, hip, and knee osteoarthritis among patients in a health maintenance organization. Arthritis Rheum 1995;38:1134-41. 10.1002/art.1780380817. [DOI] [PubMed] [Google Scholar]
- 3. Haugen IK, Englund M, Aliabadi P, et al. Prevalence, incidence and progression of hand osteoarthritis in the general population: the Framingham Osteoarthritis Study. Ann Rheum Dis 2011;70:1581-6. 10.1136/ard.2011.150078. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Kjeken I, Dagfinrud H, Slatkowsky-Christensen B, et al. Activity limitations and participation restrictions in women with hand osteoarthritis: patients’ descriptions and associations between dimensions of functioning. Ann Rheum Dis 2005;64:1633-8. 10.1136/ard.2004.034900. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Jones G, Cooley HM, Bellamy N. A cross-sectional study of the association between Heberden’s nodes, radiographic osteoarthritis of the hands, grip strength, disability and pain. Osteoarthritis Cartilage 2001;9:606-11. 10.1053/joca.2001.0460. [DOI] [PubMed] [Google Scholar]
- 6. Kwok WY, Vliet Vlieland TP, Rosendaal FR, Huizinga TW, Kloppenburg M. Limitations in daily activities are the major determinant of reduced health-related quality of life in patients with hand osteoarthritis. Ann Rheum Dis 2011;70:334-6. 10.1136/ard.2010.133603. [DOI] [PubMed] [Google Scholar]
- 7. Kolasinski SL, Neogi T, Hochberg MC, et al. 2019 American College of Rheumatology/Arthritis Foundation Guideline for the Management of Osteoarthritis of the Hand, Hip, and Knee. Arthritis Care Res (Hoboken) 2020;72:149-62. 10.1002/acr.24131. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Kloppenburg M, Kwok WY. Hand osteoarthritis–a heterogeneous disorder. Nat Rev Rheumatol 2011;8:22-31. 10.1038/nrrheum.2011.170. [DOI] [PubMed] [Google Scholar]
- 9. Richard MJ, Driban JB, McAlindon TE. Pharmaceutical treatment of osteoarthritis. Osteoarthritis Cartilage 2023;31:458-66. 10.1016/j.joca.2022.11.005. [DOI] [PubMed] [Google Scholar]
- 10. Kasapoğlu Aksoy M, Altan L. Short-term efficacy of paraffin therapy and home-based exercise programs in the treatment of symptomatic hand osteoarthritis. Turk J Phys Med Rehabil 2017;64:108-13. 10.5606/tftrd.2018.1535. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Dilek B, Gözüm M, Şahin E, et al. Efficacy of paraffin bath therapy in hand osteoarthritis: a single-blinded randomized controlled trial. Arch Phys Med Rehabil 2013;94:642-9. 10.1016/j.apmr.2012.11.024. [DOI] [PubMed] [Google Scholar]
- 12. Kang TW, Lee JH, Park DH, Cynn HS. Effects of a finger exercise program on hand function in automobile workers with hand osteoarthritis: A randomized controlled trial. Hand Surg Rehabil 2019;38:59-66. 10.1016/j.hansur.2018.09.007. [DOI] [PubMed] [Google Scholar]
- 13. Myrer JW, Johnson AW, Mitchell UH, Measom GJ, Fellingham GW. Topical analgesic added to paraffin enhances paraffin bath treatment of individuals with hand osteoarthritis. Disabil Rehabil 2011;33:467-74. 10.3109/09638288.2010.498552. [DOI] [PubMed] [Google Scholar]
- 14. Fioravanti A, Tenti S, Giannitti C, Fortunati NA, Galeazzi M. Short- and long-term effects of mud-bath treatment on hand osteoarthritis: a randomized clinical trial. Int J Biometeorol 2014;58:79-86. 10.1007/s00484-012-0627-6. [DOI] [PubMed] [Google Scholar]
- 15. Kovács C, Pecze M, Tihanyi Á, Kovács L, Balogh S, Bender T. The effect of sulphurous water in patients with osteoarthritis of hand. Double-blind, randomized, controlled follow-up study. Clin Rheumatol 2012;31:1437-42. 10.1007/s10067-012-2026-0. [DOI] [PubMed] [Google Scholar]
- 16. Stange-Rezende L, Stamm TA, Schiffert T, et al. Clinical study on the effect of infrared radiation of a tiled stove on patients with hand osteoarthritis. Scand J Rheumatol 2006;35:476-80. 10.1080/03009740600906719. [DOI] [PubMed] [Google Scholar]
- 17. Minten MJM, Leseman-Hoogenboom MM, Kloppenburg M, et al. Lack of beneficial effects of low-dose radiation therapy on hand osteoarthritis symptoms and inflammation: a randomised, blinded, sham-controlled trial. Osteoarthritis Cartilage 2018;26:1283-90. 10.1016/j.joca.2018.06.010. [DOI] [PubMed] [Google Scholar]
- 18. Kim K, Monroe JC, Gavin TP, Roseguini BT. Skeletal muscle adaptations to heat therapy. J Appl Physiol (1985) 2020;128:1635-42. 10.1152/japplphysiol.00061.2020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Ye L, Kalichman L, Spittle A, Dobson F, Bennell K. Effects of rehabilitative interventions on pain, function and physical impairments in people with hand osteoarthritis: a systematic review. Arthritis Res Ther 2011;13:R28. 10.1186/ar3254. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Mi H, Oh C, Towheed T. Systematic Review of Non-surgical Therapies for Osteoarthritis of the Hand: An Update. Eur J Rheumatol 2023;11(Suppl 1):S53-67. 10.5152/eurjrheum.2023.21197. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Valdes K, Marik T. A systematic review of conservative interventions for osteoarthritis of the hand. J Hand Ther 2010;23:334-50, quiz 351. 10.1016/j.jht.2010.05.001. [DOI] [PubMed] [Google Scholar]
- 22. Conley B, Bunzli S, Bullen J, et al. Core Recommendations for Osteoarthritis Care: A Systematic Review of Clinical Practice Guidelines. Arthritis Care Res (Hoboken) 2023;75:1897-907. 10.1002/acr.25101. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)–a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform 2009;42:377-81. 10.1016/j.jbi.2008.08.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Harris PA, Taylor R, Minor BL, et al. REDCap Consortium . The REDCap consortium: Building an international community of software platform partners. J Biomed Inform 2019;95:103208. 10.1016/j.jbi.2019.103208. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Altman R, Alarcón G, Appelrouth D, et al. The American College of Rheumatology criteria for the classification and reporting of osteoarthritis of the hand. Arthritis Rheum 1990;33:1601-10. 10.1002/art.1780331101. [DOI] [PubMed] [Google Scholar]
- 26. Bellamy N, Campbell J, Haraoui B, et al. Dimensionality and clinical importance of pain and disability in hand osteoarthritis: Development of the Australian/Canadian (AUSCAN) Osteoarthritis Hand Index. Osteoarthritis Cartilage 2002;10:855-62. 10.1053/joca.2002.0837. [DOI] [PubMed] [Google Scholar]
- 27. van de Stadt LA, Haugen IK, Felson D, Kloppenburg M. Prolonged morning stiffness is common in hand OA and does not preclude a diagnosis of hand osteoarthritis. Osteoarthritis Cartilage 2023;31:529-33. 10.1016/j.joca.2022.10.022. [DOI] [PubMed] [Google Scholar]
- 28. Kominami K, Sato K, Takahashi N. Relationship between body composition indices and changes in body temperature due to hot pack use. J Physiol Anthropol 2022;41:40. 10.1186/s40101-022-00313-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Bellamy N, Campbell J, Haraoui B, et al. Clinimetric properties of the AUSCAN Osteoarthritis Hand Index: an evaluation of reliability, validity and responsiveness. Osteoarthritis Cartilage 2002;10:863-9. 10.1053/joca.2002.0838. [DOI] [PubMed] [Google Scholar]
- 30. Pham T, van der Heijde D, Altman RD, et al. OMERACT-OARSI initiative: Osteoarthritis Research Society International set of responder criteria for osteoarthritis clinical trials revisited. Osteoarthritis Cartilage 2004;12:389-99. 10.1016/j.joca.2004.02.001. [DOI] [PubMed] [Google Scholar]
- 31. Nordenskiöld UM, Grimby G. Grip force in patients with rheumatoid arthritis and fibromyalgia and in healthy subjects. A study with the Grippit instrument. Scand J Rheumatol 1993;22:14-9. 10.3109/03009749309095105. [DOI] [PubMed] [Google Scholar]
- 32. van Riel P. EULAR Handbook of Clinical Assessments in Rheumatoid Arthritis: On Behalf of the EULAR Standing Committee for International Clinical Studies Including Therapeutic Trials-ESCISIT. Van Zuiden, 2000. [Google Scholar]
- 33. Kedor C, Detert J, Rau R, et al. Hydroxychloroquine in patients with inflammatory and erosive osteoarthritis of the hands: results of the OA-TREAT study-a randomised, double-blind, placebo-controlled, multicentre, investigator-initiated trial. RMD Open 2021;7:e001660. 10.1136/rmdopen-2021-001660. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Verbruggen G, Wittoek R, Vander Cruyssen B, Elewaut D. Tumour necrosis factor blockade for the treatment of erosive osteoarthritis of the interphalangeal finger joints: a double blind, randomised trial on structure modification. Ann Rheum Dis 2012;71:891-8. 10.1136/ard.2011.149849. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. Detry MA, Ma Y. Analyzing Repeated Measurements Using Mixed Models. JAMA 2016;315:407-8. 10.1001/jama.2015.19394. [DOI] [PubMed] [Google Scholar]
- 36. Detry MA, Lewis RJ. The intention-to-treat principle: how to assess the true effect of choosing a medical treatment. JAMA 2014;312:85-6. 10.1001/jama.2014.7523. [DOI] [PubMed] [Google Scholar]
- 37. Yadav K, Lewis RJ. Gatekeeping Strategies for Avoiding False-Positive Results in Clinical Trials With Many Comparisons. JAMA 2017;318:1385-6. 10.1001/jama.2017.13276. [DOI] [PubMed] [Google Scholar]
- 38. Wang Y, Parpia S, Couban R, et al. Compelling evidence from meta-epidemiological studies demonstrates overestimation of effects in randomized trials that fail to optimize randomization and blind patients and outcome assessors. J Clin Epidemiol 2024;165:111211. 10.1016/j.jclinepi.2023.11.001. [DOI] [PubMed] [Google Scholar]
- 39. Brosseau L, Wells G, Marchand S, et al. Randomized controlled trial on low level laser therapy (LLLT) in the treatment of osteoarthritis (OA) of the hand. Lasers Surg Med 2005;36:210-9. 10.1002/lsm.20137. [DOI] [PubMed] [Google Scholar]
- 40. Bartholdy C, Klokker L, Bliddal H, et al. Standardized rescue training as part of an exercise program for knee osteoarthritis: Proof of concept. Osteoarthritis Cartilage 2014;22:S52 10.1016/j.joca.2014.02.112. [DOI] [Google Scholar]
- 41. Kloppenburg M, Maheu E, Kraus VB, et al. OARSI Hand Clinical Trial Recommendations Work Group . OARSI Clinical Trials Recommendations: Design and conduct of clinical trials for hand osteoarthritis. Osteoarthritis Cartilage 2015;23:772-86. 10.1016/j.joca.2015.03.007. [DOI] [PubMed] [Google Scholar]
- 42. Leung YY, Li JC, Thumboo J. Domains rated as important by patients with hand osteoarthritis. Int J Rheum Dis 2019;22:2045-51. 10.1111/1756-185X.13709. [DOI] [PubMed] [Google Scholar]
- 43. Tenti S, Bruyere O, Cheleschi S, et al. An update on the use of conventional and biological disease-modifying anti-rheumatic drugs in hand osteoarthritis. Ther Adv Musculoskelet Dis 2023;15:1759720X231158618. 10.1177/1759720X231158618 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44. van der Meulen C, van de Stadt LA, Claassen A, et al. Surgical denervation as a treatment strategy for pain in hand osteoarthritis: a systematic literature review. RMD Open 2023;9:e003134. 10.1136/rmdopen-2023-003134. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45. Oo WM, Hunter DJ. Efficacy, Safety, and Accuracy of Intra-articular Therapies for Hand Osteoarthritis: Current Evidence. Drugs Aging 2023;40:1-20. 10.1007/s40266-022-00994-3. [DOI] [PubMed] [Google Scholar]
- 46. Bellamy N, Hochberg M, Tubach F, et al. Development of multinational definitions of minimal clinically important improvement and patient acceptable symptomatic state in osteoarthritis. Arthritis Care Res (Hoboken) 2015;67:972-80. 10.1002/acr.22538. [DOI] [PubMed] [Google Scholar]
- 47. Siviero P, Limongi F, Gesmundo A, et al. EPOSA Research Group . Minimal clinically important decline in physical function over one year: EPOSA study. BMC Musculoskelet Disord 2019;20:227. 10.1186/s12891-019-2593-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supplementary information: Protocol, pictures of the mittens, statistical analysis plan, protocol violation, and tables S1 and S2
Data Availability Statement
Data will be made available upon reasonable request to the corresponding author at cecilie.bartholdy.skjaldgaard@regionh.dk.