
Figure 1 –
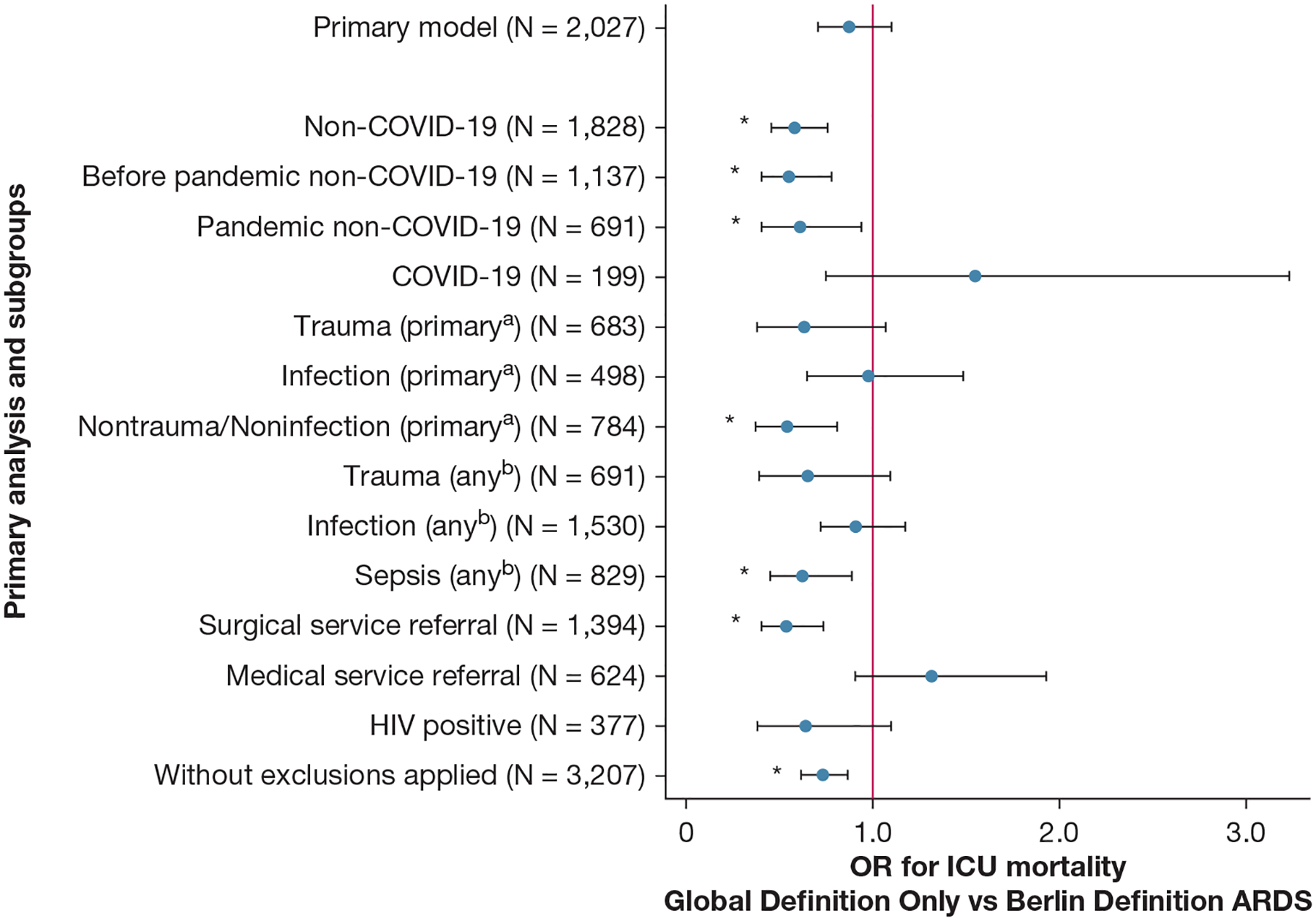
Forest plot showing ICU mortality according to only the global definition ARDS vs the Berlin definition of ARDS by subgroups. After adjustment for hospital-level factors, patients who met only the global definition of ARDS criteria (ie, who would not have been captured by the Berlin definition) showed no statistically significant different ICU mortality vs patients meeting the Berlin definition of ARDS criteria (21.7% [95% CI, 18.9%−24.4%] vs 23.8% [95% CI, 21.5%−26.2%]; OR, 0.88 [95% CI, 0.70–1.10]; P = .25). However, prespecified exploratory subgroup analyses revealed heterogeneity. Patients without COVID-19 meeting only the global definition of ARDS criteria showed reduced ICU mortality (14.2% [95% CI, 11.6%−16.9%] vs 22.2% [95% CI, 19.8%−24.6%]; OR, 0.58 [95% CI, 0.45–0.75]; P < .0005) compared with patients without COVID-19 and meeting the Berlin definition of ARDS, whereas patients with COVID-19 meeting only the global definition of ARDS criteria showed a suggestion of increased ICU mortality that did not reach statistical significance (58.6% [95% CI, 51.0%−66.2%] vs 48.7% [95% CI, 34.1%−63.3%]; OR, 1.55 [95% CI, 0.74–3.24]; P = .25) compared with patients with COVID-19 meeting the Berlin definition of ARDS. aPrimary refers to the primary indication for ICU admission as determined by the admitting ICU team as part of real-time routine care. bAny refers to acute active diagnoses and processes present at the time of ICU admission (but not necessarily the primary indication for ICU admission) as determined by the admitting ICU team as part of real-time routine care. *P < .05.