
FIGURE 1.
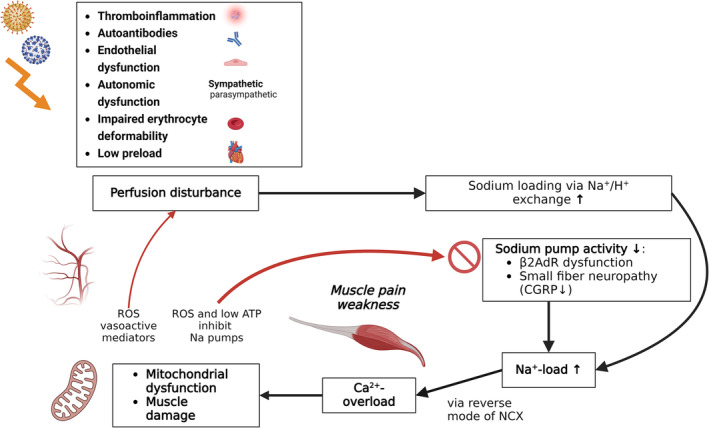
Several mechanisms triggered by an infection can result in circulatory disturbance and hypoperfusion of muscles including autoantibodies [41], inflammation [22], sympathetic overactivity [10], endothelial dysfunction [42], impaired red blood cell deformability [43] and diminished preload [10]. Upon exertion, hypoperfusion of skeletal muscles leads to rise in protons, intracellular sodium and calcium [12], muscle necrosis [9], mitochondrial damage and enhanced production of reactive oxygens [13, 22]. In ME/CFS, the activation of the sodium pump (Na+/K+‐ATPase) upon exertion may be diminished due to low ATP and dysfunctional ß2AdR and CGRP. At a certain level of intracellular sodium, the sodium‐calcium‐exchanger NCX changes its transport mode from calcium export to calcium import causing calcium overload that causes mitochondrial and myocyte damage. As a result, low ATP and ROS production further impair the sodium pump. ROS also impairs vascular function and perfusion. A vicious circle arises. ß2AdR: ß2‐adrenergic receptor; CGRP: calcitonin‐gene–related peptide; ROS: reactive oxygen species. Biorender was used to create the figure.