

Abstract
BACKGROUND
The needs of people with deafblindness remain poorly understood and addressed globally. This study is part of a larger body of work to develop Core Sets for deafblindness using the International Classification of Functioning, Disability, and Health (ICF).
AIM
To determine the perspectives on functioning of individuals with lived experience of deafblindness as they relate to the ICF.
DESIGN
Cross-sectional interview study.
SETTING
Global, representing all six regions of the World Health Organization.
POPULATION
A diverse cohort of 72 individuals living with deafblindness or as close family members, ranging across the spectrum of severity.
METHODS
Qualitative interviews and focus groups were used to explore six open-ended questions about perceived barriers and facilitators to functioning of body functions and structures, activities and participation, and environmental and personal factors. Data were synthesized using content analysis, and the resulting topics were linked to the ICF codes using established linking methodology prescribed by the World Health Organization’s ICF Research Branch. Descriptive statistics summarized all demographic data.
RESULTS
The analyses of the transcripts uncovered 2534 meaning units, leading to the identification of 492 corresponding distinct codes from the ICF framework, and spanning across 93.33% of coding categories available. Sensory (b2) and Mental Functions (b1) emerged as the most frequent Body Functions (b) codes. Most categories referred to Activities & Participation, with Mobility (d4) being the most frequently mentioned topic. Services, Systems and Policies (e5) was the most frequently used Environmental factor.
CONCLUSIONS
Over 93% of the ICF classification categories were accessed to code the data provided by participants, demonstrating the complexity of functioning with deafblindness. This study provides valuable information to shape policy and research by providing representation of lived experience towards the consensus conference for the comprehensive and abbreviated Core Sets for deafblindness.
CLINICAL REHABILITATION IMPACT
The inclusion of lived experience provides a holistic understanding of the daily challenges faced by individuals living with deafblindness. By being part of this process, they have a voice in shaping the classification system that will be used to describe their experiences, fostering a sense of ownership and empowerment.
Key words: Deafness; Blindness; International Classification of Functioning, Disability and Health; Qualitative research
Deafblindness is functionally defined by the limitations that the combined vision and hearing difficulties place on the ability to participate in society; these limitations can only be addressed through support services and strategies, adaptations to the environment, and the introduction of assistive devices and technologies.1 Definitions based on variables used in the medical field (e.g., visual acuity, visual field diameter and pure-tone audiogram thresholds) can vary widely, depending on location and context.2 Additional variability is created by using self-report measures, creating prevalence estimates ranging from as low as 0.003% at the population level,3 to as high as 58.6% among older adults.4 Many of these definitions have been criticized for underestimating the complexity of the impairment and the experience of disability because they are considering vision and hearing separately, thereby ignoring the potential interaction of the combined impairment and its unique nature.5
A key approach to advancing the definition and the recognition of deafblindness as a unique disability, and to harmonize a global terminology and comprehension of its functional effects, is the development of World Health Organization, International Classification of Functioning, Disability and Health (ICF) Core Sets.6 Using the ICF coding system, Core Sets provide a condensed, usable, and relevant approach to implementing the ICF codes for clinical assessment, research, and policy development in relation to specific health conditions. More importantly, Core Sets are mandated to be finalized based on the perspectives of all interested parties, including professional experts (e.g., in the case of deafblindness: tactile sign language interpreters or intervenors), health and social service providers, as well as the individuals with lived experience themselves.7 Work has been undertaken towards the development of Core Sets for deafblindness,8 whereby the perspectives of researchers9, 10 and expert professionals or health and social service providers in the field11 have previously been published. The next step in this process is the exploration of the viewpoint on functional aspects related to living with deafblindness.
The perspectives of individuals living with deafblindness are generally underrepresented within the research literature.12 In part, this underrepresentation is rooted in methodological difficulties that arise when working with persons that have difficulty accessing traditional research modalities, such as paper-format consent forms, or questionnaires.13, 14 However, there are several examples where such access and inclusion barriers were overcome successfully, providing insight into the concerns of individuals with deafblindness. For example, a scoping review of studies exploring reasons for device abandonment summarized qualitative and quantitative data collected with participants with deafblindness.15 A recent eBook presented a collection of studies on deafblindness that included individuals across all ages, exploring their perspectives on topics such as wellbeing and health, communication and information access, assistive technology and devices, and general methodological and support topics.16 Individuals with deafblindness have been involved in best practice development.17 Their perspectives include those of individuals ageing with congenital deafblindness18 as well as those that age into acquired deafblindness.19 Finally, and most importantly, the leadership of researchers and topic experts that live with deafblindness themselves guides the way towards equity and inclusion in the determination of priorities and the development of solutions.20-24 Given the diversity of the population of individuals with deafblindness, and that the degree of impairment prevents some individuals from sharing their experiences in a formal way, the perspectives of parents and other family members are critical. There are important examples of parents who have engaged as researchers and experienced experts themselves, on behalf of their own children living with deafblindness.25-27 Participatory action research examples include the experience of parents and siblings,28 and those of the children of parents living with deafblindness.29
Previous studies on deafblindness have considered the ICF as its framework or analysis guide; for example, when exploring activity limitations and participation barriers,19, 30 or environmental and contextual obstacles to assistive device use.15 Crowe et al.31 framed their interpretation of communication strategies used by older individuals with deafblindness within the ICF. Finally, Möller32 critically examined the ICF as an assessment tool when working with participants with deafblindness. Möller’s study laid some of the groundwork for the need to consider the development of Core Sets for deafblindness, as the author specifically points towards potential benefits (e.g., common language), shortcomings (e.g., personal factors and quality of life), and solutions (e.g., development and inclusion of more complex social variables in the coding system) of applying the ICF to deafblindness. The development of ICF Core Sets is an important step in achieving such solutions. Here, we focus on the perspectives of individuals living with deafblindness themselves in relation to functioning to contribute to this process.
Materials and methods
Ethical considerations
This multi-site study was approved by the institutional review boards of the Centre de recherche interdisciplinaire en réadaptation du Montréal métropolitain (MP-50-2023-1749), and the Université de Montréal (CERC 2023-4150) in Canada, the Instituto del Salud Carlos III (#CEI PI 44_2021-v3) in Spain, and the University of Melbourne (#2023-25708-42888-3) in Australia. The findings are presented here following the recommendations laid out in the COnsolidated criteria for REporting Qualitative research (COREQ) checklist.33
Study design
We utilized a qualitative methodology with focus groups and individual interviews as primary means of data collection as recommended by Selb et al.7 for this stage of developing Core Sets for deafblindness. More specifically, 26 interviews and 9 focus groups were conducted, online or in person, with participants from the six WHO regions. The modality depended on the context and feasibility of local circumstances for interacting with participants (e.g., the availability of interpreters/intervenors/parents, and/or assistive devices), with the goal of enhancing the participation of individuals with deafblindness across as many regions as possible. For example, individuals who required tactile communication support were recruited for individual interviews instead of participation in a focus group, given the logistics barriers for group communication among individuals living with deafblindness.
Recruitment procedure
We employed convenience sampling with a maximum variation strategy,34 which was ensured by considering factors such as age, sex, severity, and etiology of deafblindness. Recruitment procedures varied according to local context, ranging from identification through client databases of rehabilitation or health and social services centers, snowball sampling, or referral through professionals or service providers. Based on a local grant, participants recruited and/or interviewed through the Canadian sites received $50 CAD as acknowledgement of the time and effort provided by participating.
Study population
We included individuals living with deafblindness and/or informal caregivers as the target population. Individuals with deafblindness were considered eligible for participation if they 1) self-identified as deafblind, regardless of clinical confirmation; 2) were at least 18 years of age; 3) were willing to openly discuss various aspects related to functioning, disability, and contextual factors concerning their personal experience with deafblindness; and 4) demonstrated comprehension of the study’s objectives. This was determined through the recruitment process and obtaining consent to participate. Informal caregivers (e.g., parents of children with deafblindness or other family members) were included to provide a perspective on deafblindness relevant to children under 18 with deafblindness, and those with children (in some cases adult children) with congenital deafblindness who were unable to self-report. Caregivers were eligible if they 1) were at least 18 years of age; and 2) cared for an individual with deafblindness of any age. Each recruitment site was provided with instructions to approach potential participants that vary on the following criteria: age, age of onset of either impairment, sex, severity of either impairment, communication modality, and diagnostic information (if available). As recruitment was progressing, the research team monitored the distribution of participant characteristics as much as possible, and the encouraged sites where recruitment was still ongoing to identify under-represented individuals (e.g., we specifically aimed to include individuals who live with one congenital and one age-related sensory impairment, as this group is rarely represented in deafblindness research).
Materials
To conduct the interviews and focus groups, a standard interview guide was available to local moderators, which included items to collect demographic information. It was followed by a section asking six open-ended questions, aligned with various ICF components such as Body functions, Body structures, Activities & participations, Environmental factors, and Personal factors (Supplementary Digital Material 1: Supplementary Tables I-V). Each moderator also incorporated probing questions to provide clarification as needed. These questions were adapted from previous core-set projects7 and tailored to suit the specific communication needs of the children and adult participants with deafblindness.
Data collection procedure
Depending on the communication capacities or preferences, informed consent or assent was obtained verbally, through signed or tactile communication methods, or through a communication facilitator (e.g., family member), in line with previously described guidelines and recommendations.13, 35 Each focus group or interview was overseen by a local moderator with extensive training and experience in leading discussions and conducting interviews with individuals living with deafblindness. These moderators included project research assistants, interpreters/intervenors, or individuals affiliated with organizations providing deafblind-specific services. In situations where it was feasible and suitable, an assistant accompanied the moderator to facilitate the interactions. Focus group session or interviews lasted up to 3 hours, were recorded, and later transcribed verbatim. When necessary and possible, the transcripts of interactions conducted in a language other than English were translated using DeepL Translator software (Cologne, Germany), and then proofread by a bilingual native speaker.
Data linking methodology
The key research team members (AJ, SG, WW) received training from the WHO’s ICF Research Branch on developing ICF Core sets, including the linking procedure.8 Subsequently, these authors trained other team members (SD, TOO, CG). The training on the linking process involved identifying underlying concepts related to functioning in the data and linking them to ICF categories using established ICF linking rules.36, 37 The methodology for data linking in this qualitative study followed the same steps as in our previous ICF systematic literature review and the expert survey9, 11 and was conducted by the same team members (TOO, SD, CG) to benefit from their experience, ensure consistency, and reduce inter-rater variability. Drawing on the expertise of a senior author (SG), a linking template was created, guiding the process across seven sections: Meaning Unit; Meaningful Concept; Interpretation of Underlying Meaning; Linking Unit; ICF Code; ICF Description; and Final Codes.38 All the qualitative responses from the participants were coded and linked using this template. Adhering to updated rules for ICF linking,36 codes such as “other specified” [code 8] and “unspecified” [code 9] were selectively applied when the available information could not be accommodated within existing codes. Whenever relevant, personal factors were identified and coded as PF.
Results
Participant characteristics
Qualitative interviews and focus groups engaged a diverse cohort of 72 participants, strategically recruited to ensure equitable representation across the six WHO regions. The recruitment target of at least seven participants from each region was met, fostering a globally inclusive perspective. The Americas and the Western Pacific regions emerged as significant contributors, yielding 20 and 13 participants, respectively. Table I provides detailed information on the profiles of the study sample.
Table I. —Study characteristics of participants (N.=72).
| Sex % | |
| Female | 41.67 (N.=30) |
| Male | 31.94 (N.=23) |
| Unknown | 26.39 (N.=19) |
| Age: mean (SD) [range] | 41.69 (19.56) [1-83] |
| <18 | 6.94 (N.=5) |
| 18-40 | 25 (N.=18) |
| 41-60 | 22.22 (N.=16) |
| >61 | 9.72 (N.=7) |
| Unknown | 36.11 (N.=26) |
| Participant % | |
| Person living with deafblindness | 45.83 (N.=33) |
| Caregiver | 41.66 (N.=30) |
| Not specified | 12.5 (N.=9) |
| WHO Region (%) | |
| Region of the Americas | 27.78 (N.=20) |
| Canada | N.=10 |
| Mexico | N.=10 |
| Western Pacific Region | 18.06 (N.=13) |
| Australia | N.=13 |
| European Region | 13.89 (N.=10) |
| Spain | N.=7 |
| United Kingdom | N.=2 |
| France | N.=1 |
| African Region | 12.50 (N.=9) |
| Zambia | N.=9 |
| Eastern Mediterranean | 12.50 (N.=9) |
| Egypt | N.=9 |
| South-East Asia | 15.28 (N.=11) |
| India | N.=7 |
| Nepal | N.=4 |
| Deafblindness onset (%) | |
| Congenital | 47.22 (N.=34) |
| Acquired | 11.11 (N.=8) |
| Not specified | 41.67 (N.=30) |
| Deafblindness diagnosis (%) | |
| Usher Syndrome | 16.67 (N.=12) |
| Rubella | 5.56 (N.=4) |
| CHARGE syndrome | 5.56 (N.=4) |
| Complication of prematurity | 2.78 (N.=2) |
| Glaucoma, nature of hearing loss unknown | 2.78 (N.=2) |
| Glaucoma and middle ear/eardrum damage | 1.39 (N.=1) |
| CAGSSS syndrome | 1.39 (N.=1) |
| NORRIE disease | 1.39 (N.=1) |
| Chromosome 10q translocation | 1.39 (N.=1) |
| Quadriplegic Cerebral Palsy | 1.39 N.=1) |
| Cerebral Palsy, Klinefelter’s Syndrome | 1.39 (N.=1) |
| Smith-Magenis Syndrome | 1.39 (N.=1) |
| Viral infection | 1.39 (N.=1) |
| Cataracts, nature of hearing loss unknown | 1.39 (N.=1) |
| Cataracts and hearing infections | 1.39 (N.=1) |
| Coloboma, nature of hearing loss unknown | 1.39 (N.=1) |
| Congenital deafness with bilateral cataracts | 1.39 (N.=1) |
| Multiple congenital anomalies with deafblindness | 1.39 (N.=1) |
| Direct Trauma to the eye and/or ear | 1.39 (N.=1) |
| Retinal detachment and age-related hearing loss | 1.39 (N.=1) |
| Hydrocephaly | 1.39 (N.=1) |
| Maternal drug use | 1.39 (N.=1) |
| Other | 2.78 (N.=2) |
| Unknown | 38.89 (N.=28) |
Value rounded to two decimal places.
ICF categories
The analyses of the transcripts uncovered 2534 meaning units, leading to the identification of 492 distinct codes from the ICF framework. The management of this large number of codes was facilitated by systematic tracking and sorting within a central Microsoft Excel file in which codes and their associated information could be sorted and counted as needed. A proportional overview of their distribution is provided in Figure 1, and a breakdown of the identified code for each chapter of each category is provided in Table II. Of the 30 chapters comprising the ICF, 28 were included in the coding process, corresponding to 93.33% of coding categories available.
Figure 1.
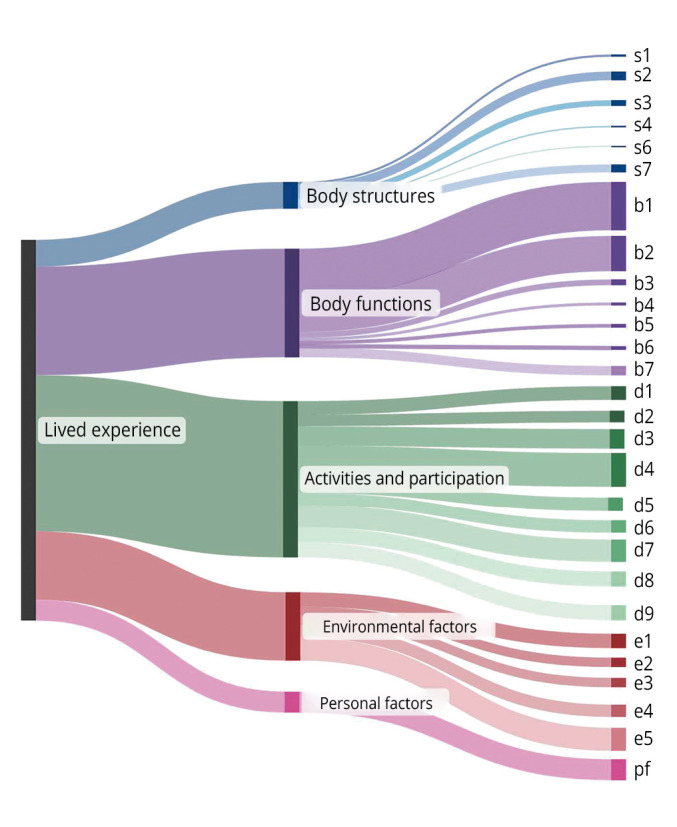
—Proportional frequency distribution of ICF chapters utilized during the linking process of responses from 72 individuals with lived experience of deafblindness. The width of each branch represents the proportional frequency use of unique ICF codes.
Table II. —Frequency of distinct codes identified within each chapter of the ICF framework categories concerning deafblindness.
| Category | Chapters | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Body structures | s1 Structures of the nervous system N.=3 |
s2 The eye, ear, and related structures N.=12 |
s3 Structures involved in voice and speech N.=8 |
s4 Structures of the cardiovascular, immunological and respiratory systems N.=2 |
s5 Structures related to the digestive, metabolic, and endocrine systems N.=0 |
s6 Structures related to the genitourinary and reproductive systems N.=1 |
s7 Structures related to movement N.=11 |
s8 Skin and related structures N.=0 |
|
| Activities and participation | d1 Learning and applying knowledge N.=19 |
d2 General tasks and demands N.=16 |
d3 Communication N.=27 |
d4 Mobility N.=47 |
d5 Self-care N.=19 |
d6 Domestic life N.=17 |
d7 Interpersonal interactions and relationship N.=31 |
d8 Major life areas N.=21 |
d9 Community, social and civic life N.=21 |
| Environmental factors | e1 Products and technology N.=20 |
e2 Natural environment and human-made changes to environment N.=13 |
e3 Support and relationships N.=13 |
e4 Attitudes N.=17 |
e5 Services, systems, and policies N.=33 |
||||
| Body functions | b1 Mental functions N.=67 |
b2 Sensory functions and pain N.=49 |
b3 Voice and speech functions N.=8 |
b4 Functions of the cardiovascular, haematological, immunological, and respiratory systems N.=4 |
b5 Functions of the digestive, metabolic and endocrine systems N.=5 |
b6 Genitourinary and reproductive functions N.=5 |
b7 Neuromusculoskeletal and movement-related functions N.=13 |
b8 Functions of the skin and related structures N.=0 |
|
Body functions (B)
A total of 707 meaning units regarding body functions were raised by participants (27.90%). Seven of the eight chapters of this category were identified as relevant to deafblindness. Of these:
44.59% belonged to Chapter 1, Mental functions;
32.43% belonged to Chapter 2, Sensory functions and pain;
8.78% belonged to Chapter 7, Neuromusculoskeletal and movement-related functions;
5.41% belonged to Chapter 3, Voice and speech functions;
3.38% belonged to Chapter 5, Functions of the digestive, metabolic and endocrine systems;
3.38% belonged to Chapter 6, Genitourinary and reproductive functions;
2.03% belonged to Chapter 4, Functions of the cardiovascular, hematological, immunological, and respiratory systems;
no meaningful concepts were identified in relation to Chapter 8, Functions of the skin and related structures.
The top five identified codes in this category, all levels combined were emotional functions (b152; N.=57), temperament and personality functions (b126; N.=43), hearing functions (b230; N.=40), seeing functions (b210; N.=39), and confidence (b1266; N.=32). The extensive list of meaning units for this ICF category is provided in Supplementary Table I.
Body structures (S)
A total of 74 meaning units in relation to body structures were raised by participants. Six of the eight chapters of this category were identified as relevant to deafblindness. Of these:
32.43% belonged to Chapter 2, The eye, ear, and related structures;
29.73% belonged to Chapter 7, Structures related to movement;
21.62% belonged to Chapter 3, Structures involved in voice and speech;
8.11% belonged to Chapter 1, Structures of the nervous system;
5.41% belonged to Chapter 4, Structures of the cardiovascular, immunological and respiratory systems;
2.70% belonged to Chapter 6, Structures related to the genitourinary and reproductive systems;
no meaningful concepts were identified in relation to Chapter 5, Structures related to the digestive, metabolic, and endocrine systems as well as Chapter 8, 8 Skin and related structures.
The top five identified codes in this category, all levels combined were eye, ear and related structures, unspecified (s299; N.=10), retina (s2203; N.=7), lens of eyeball (s2204; N.=5), structure of external ear (s240; N.=4), teeth (s3200; N.=4). The extensive list of meaning units for this ICF category is provided in Supplementary Table II.
Activities and participation (D)
This ICF category elicited the greatest number of meaning units (n=894, 35.28%). All nine of the chapters were identified as relevant to deafblindness. Of these:
21.40% belonged to Chapter 4, Mobility;
14.22% belonged to Chapter 7, Interpersonal interactions and relationships;
12.56% belonged to Chapter 3, Communication;
9.77% belonged to Chapter 9, Community, social and civic life;
8.84% belonged to Chapter 8, Major life areas;
8.84% belonged to Chapter 1, Learning and applying knowledge;
8.84% belonged to Chapter 5, Self-care;
7.91% belonged to Chapter 6, Domestic life;
7.44% belonged to Chapter 2, General tasks and demands.
The top five identified codes in this category, all levels combined were communication, unspecified (d399; N.=34), socializing (d9205; N.=31), walking around obstacles (d4503; N.=26), interpersonal interactions and relationships, unspecified (d799; N.=20), and work and employment, other specified and unspecified (d859; N.=19). The extensive list of meaning units for this ICF category is provided in Supplementary Table III.
Environmental factors (E)
Environmental factors comprised the second category to elicit a great number of meaning units (N.=785, 30.98%). All five chapters of this category were identified as relevant to deafblindness. Of these:
34.78% belonged to Chapter 5, Services, systems, and policies;
21.74% belonged to Chapter 1, Products and technology;
15.22% belonged to Chapter 4, Attitudes;
14.13% belonged to Chapter 2, Natural environment and human-made changes to environment;
14.13% belonged to Chapter 3, Support and relationships.
The top five identified codes in this category, all levels combined were societal attitudes (e460; N.=72), immediate family (e310; N.=58), personal care providers and personal assistants (e340; N.=52), assistive products and technology for communication (e1251; N.=45), and individual attitudes of immediate family members (e410; N.=36). The extensive list of meaning units for this ICF category is provided in Supplementary Table IV.
Personal factors
Meaningful concepts that could not be coded using the ICF framework were identified as nc. Twenty-nine personal factors were identified. The most prominent ones included the experience of the Covid-19 pandemic (N.=9), health status (N.=8), age (N.=5) as well as housing/living situation (N.=5). The complete list of personal factors is provided in Supplementary Table V.
Discussion
An overview of the perspectives of persons with lived experience of deafblindness reveals a remarkable 93.3% of available ICF chapters that were accessed during coding the data, emphasizing the complexity of their experiences. This proportion stands out in comparison to the 73.3% of chapters involved in the coding of the data in the deafblindness experts survey,11 60% of chapters accessed for coding the qualitative interviews conducted with individuals living with hearing loss,38 and 53.3% used when coding the vision loss systematic literature review.39 It is not surprising that the largest proportion of codes relevant to the participants referred to Activities and Participation (e.g., aspects related to communication). This finding is in line with the results of previous research9 but in comparison with the results of the expert survey11 was higher. The proportional presentation of Activities and Participation was somewhat under-represented among the responses of experts. Unlike experts, both individuals with lived experience and the systematic literature review placed proportionally less emphasis on environmental variables, such as assistive devices and human support. Somewhat unexpectedly, individuals with lived experience provided detailed information on the affected body structures, much in line with the data that emerged from the research literature.
All three data sources confirmed that among Body Functions (b) codes, Mental functions (b1) and Sensory functions (b2) were of most prominent concern, followed by Neuromusculoskeletal and movement-related functions (b7). It is likely that the importance of this last chapter indicates that deafblindness is often part of a complex health profile that includes many other impairments beyond the sensory, such as in the most common genetic cause of congenital deafblindness – CHARGE syndrome,40 or age-related comorbidities such as rheumatoid arthritis.41 The distribution of code priorities within Activities and Participation (d) as reported by individuals with lived experience highlighted Mobility (d4), Interpersonal interactions and relationships (d7) and Communication (d3). Interestingly, while d4 was also among the four most frequently expressed perspectives of experts,11 very little research focused on aspects of mobility9 – a clear gap that needs addressing. Both Interpersonal interactions and relationships (d7) and Communication (d3) were core components in all data three sources. It is of note that mobility and communication are prerequisites for interactions and relationships with others. Communication has been recognized as a key issue for this population. The development and maintenance of expressive and receptive communication abilities of individuals living with any form and severity of deafblindness is key to the development of cognition as well as literacy.42 Its importance is recognized for all aspects of activities and participation across the lifespan.43, 44 Similarly, Interpersonal interactions and relationships (d7) are agreed upon as important for individuals living with deafblindness, reflecting the role of family, friends, and members of the immediate environment as part of their interactions with their social network. The perceptions of these interactions (or lack thereof) may include the experience of how living with such a profound disability affects social relationships in general. Interpersonal interactions likely play an even larger role in low- or middle-income regions of the world where neither policies and services, nor extensive support through technology or other environmental variables are available.
Individuals with lived experience emphasized the importance (and/or absence) of Services, systems, and policies (e5) and Products and technology (e1) for achieving independence and quality of life. Interestingly, the research literature reflected this emphasis on Products and technology,9 whereas the expert survey aligned with the need for Services, systems, and policies.11 However, while research has otherwise focused on the Natural environment and human-made changes to environment (e2) in the context of accessibility adaptation, experts also emphasized Supports and Relationships (e3), neither of whom were frequently mentioned among the perspective of individuals with lived experience. As previously alluded to,11 it is possible that research topics according to published literature are influenced by funding priorities, more so than the needs of the target population. It may simply be easier to obtain technology research and development funds than find support for psycho-social research. Similarly, experts may be more concerned about services they offer and the availability of policies and services that can support their professions, given that their income and careers depend on them. Either way, it was remarkable to observe how many personal factors emerged according to the participants with lived experience. The detailed descriptions of needs, barriers and facilitators provided more refined information about the specific variables of interest to our target population than any other methodological approach (Supplementary Table V).
Research and policy implications
The comparison of ICF categories used across the preparatory studies so far has clearly indicated gaps that will become research priorities in coming years, especially now that the main concerns of individuals living with deafblindness are clearly indicated. Aside from the glaring lack of research in mobility for individuals with deafblindness, there are additional priority areas that become apparent on more detailed examination of the data. For example, factors related to self-care (d5) or domestic life (d6) are proportionally mentioned much more often by individuals with lived experience than they are acknowledged by the research literature or experts. It is possible that this observation is an indicator for individuals with deafblindness of a wish for increased independence, with a focus on self-care at home, that is not well communicated or understood by the individuals in their immediate environment. Such discrepancies can assist in determining research priorities to improve the lives of individuals with deafblindness by placing effort in line with need. Such an approach will likely increase community engagement in promoting research priorities and is an important step for forming critical mass on a global scale to bring together collaborative teams. Collaborations among the team members and their community partners have already extended into work on the Global Sustainable Development Goals in the specific context of deafblindness.45 Finalizing the Core Sets will further focus these efforts.
Limitations of the study
The limitations of this study need to be viewed within the context of conducting research with individuals living with deafblindness across the globe. It is remarkable that this international collaboration was able to facilitate recruitment and data collection across all six regions of the World Health Organization; however, not all data collection sites were equipped with comparable resources. Therefore, some of the demographic data are incomplete or were not obtainable. In addition, there is likely recruitment bias present, given the resources necessary to identify and recruit individuals with deafblindness, as they need to be known to the local partners, be reachable and have the resources to become part of the project. Even though the team took all possible steps to support participation, equal access to identify and include all potential participants across the entire spectrum of recruitment criteria may not have been realizable within the constraints of the project in all of the WHO regions.
A methodological limitation of the process when developing Core Sets is the cross-sectional approach to each of the preparatory studies, including the present qualitative interviews. This approach does not allow for an in-depth understanding of how functional abilities vary or develop over time. Therefore, future studies on the implementation and acceptance of the Core Sets, and their refinement over time will depend on longitudinal approaches to using them in research and service delivery.
The analysis and synthesis presented here provide a merged view across all regions, yet it is likely that barriers and facilitators differ as a function of financial resources and vary for different sub-populations of individuals living with deafblindness. Therefore, the next step in the analysis is to explore coding differences as a function of the WHO region and compare variations according to the income level of participants and/or the represented countries. Furthermore, we are planning to separate data that refer to children and youth, supplement these data through additional data collection, and then develop additional Core Sets specific to Children and Youth. This final step is particularly important in the context of deafblindness, given the large number of congenital and early onset diagnostic categories that cause deafblindness.3, 46
Conclusions
The present study provides a clear voice for individuals living with deafblindness and their family members and carers to contribute to the development of ICF Core Sets for deafblindness. The inclusion of their perspective allows the resulting Core Sets to reflect their level of functioning and can guide the development of content that points toward important facilitators and barriers towards participation. The representation of participants from across all six regions of the World Health Organization and across the range of ages, severities, diagnostics, and communication modalities makes this synthesis especially valuable, given that recruitment and data collection with this population was successful despite logistic and infrastructure limitations. The representation of health and social care needs from the perspective of persons with lived experience is a challenge in general but becomes an even more pressing topic when the population of interest is, by its very nature, marginalized because of communication barriers, as in the case here. The next step in the process of Core Set development is the integration and synthesis of the data from the preparatory studies to assemble the preliminary Core Sets, currently scheduled to be discussed at a consensus conference in October 2024. We anticipate the presentation and publication of the finalized version of the comprehensive and abbreviated Core Sets for deafblindness before the end of 2024, allowing us to begin the process of implementation and refinement.7
Supplementary Digital Material 1
Supplementary Table I
Identified ICF codes from the Body Functions (b) category mentioned by the participants per sub-level.
Supplementary Table II
Identified ICF codes from the Body Structures (s) category mentioned by the participants per sub-level.
Supplementary Table III
Identified ICF codes from the Activities & Participation (d) category mentioned by the participants per sub-level.
Supplementary Table IV
Identified ICF codes from the Environmental Factors (e) category mentioned by the participants per sub-level.
Supplementary Table V
Identified personal factors relevant to deafblindness and their frequency.
Acknowledgements
We would like to express our thanks to Norman Robert Boie, Daniela Anze, Sonja van de Molengraft, Frank Kat, Mirko Baur, the World Federation of the Deafblind, and the DbI European Deafblind Network, Able Australia, and Deafblind Australia for the support towards this project. A special Thank You goes to all the intervenors who supported interviews with persons with deafblindness.
Footnotes
Conflicts of interest: The authors certify that there is no conflict of interest with any financial organization regarding the material discussed in the manuscript.
Funding: This work was funded by Deafblind International, Deafblind Ontario Services Foundation, the Fonds de recherche du Québec - Santé Vision Health Research Network, and by a Global Partnerships for Research and Innovations grant from Canadian Hearing Services.
References
- 1.Centre for Welfare and Social Issues. The Nordic definition of deafblindness. 2016 [Internet]. Available from: http://www.kuurosokeat.fi/tiedosto/nordic_definition.pdf [cited 2024, Sep 25].
- 2.Bright T, Ramke J, Zhang JH, et al. Prevalence and impact of combined vision and hearing (dual sensory) impairment: A scoping review. Robinson J, ed. PLOS Global Public Health. 2023;3(5):0001905. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Dammeyer J. Prevalence and aetiology of congenitally deafblind people in Denmark. Int J Audiol 2010;49:76–82. https://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=20151880&dopt=Abstract 10.3109/14992020903311388 [DOI] [PubMed] [Google Scholar]
- 4.Rong H, Lai X, Jing R, Wang X, Fang H, Mahmoudi E. Association of Sensory Impairments With Cognitive Decline and Depression Among Older Adults in China. JAMA Netw Open 2020;3:e2014186. https://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=32990739&dopt=Abstract 10.1001/jamanetworkopen.2020.14186 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.McInnes JM. Deafblindness: A unique disability. In: McInnes JM, editor. A Guide to Planning and Support for Individuals Who Are Deafblind. Toronto: University of Toronto Press; 1999. p. 1-33. [Google Scholar]
- 6.World Health Organization. World Health Organization: International Classification of Functioning, Disability and Health (ICF) [Internet]. Available from: https://www.who.int/standards/classifications/international-classification-of-functioning-disability-and-health [cited 2022, Oct 8]. Accessed October 8, 2022.
- 7.Selb M, Escorpizo R, Kostanjsek N, Stucki G, Üstün B, Cieza A. A guide on how to develop an International Classification of Functioning, Disability and Health Core Set. Eur J Phys Rehabil Med 2015;51:105–17. https://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=24686893&dopt=Abstract [PubMed] [Google Scholar]
- 8.Paramasivam A, Jaiswal A, Minhas R, Holzhey P, Keyes K, Lopez R, et al. The development of the International Classification of Functioning, Disability and Health Core Sets for deafblindness: A study protocol. PLoS One 2021;16:e0261413. https://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=34905579&dopt=Abstract 10.1371/journal.pone.0261413 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Jaiswal A, Paramasivam A, Budhiraja S, Santhakumaran P, Gravel C, Martin J, et al. The International Classification of Functioning, Disability and Health (ICF) core sets for deafblindness, part II of the systematic review: linking data to the ICF categories. Eur J Phys Rehabil Med 2024. [Epub ahead of print]. https://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=39235255&dopt=Abstract 10.23736/S1973-9087.24.07984-X [DOI] [PMC free article] [PubMed]
- 10.Paramasivam A, Jaiswal A, Budhiraja S, Holzhey P, Santhakumaran P, Ogedengbe T, et al. The development of the International Classification of Functioning, Disability and Health Core Set for deafblindness Part I: A systematic review of outcome measures identified in deafblindness research. Eur J Phys Rehabil Med 2023;59:615–27. https://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=37458491&dopt=Abstract 10.23736/S1973-9087.23.07890-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Wittich W, Dumassais S, Jaiswal A, Paramasivam A, Budhiraja S, Lopez R, et al. Development of core sets for deafblindness: an international expert survey on functioning and disability of individuals living with deafblindness using the International Classification of Functioning, Disability, and Health. Eur J Phys Rehabil Med 2024;60:382–90. https://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=38502555&dopt=Abstract 10.23736/S1973-9087.24.08188-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Watharow A, Wayland S. Making Qualitative Research Inclusive: Methodological Insights in Disability Research. Int J Qual Methods 2022;21. 10.1177/16094069221095316 [DOI]
- 13.Wittich W, Boie NR, Jaiswal A. Methodological Approaches to Obtaining Informed Consent when Conducting Research With Individuals With Deafblindness. Int J Qual Methods 2023;22:1–11. 10.1177/16094069231205176 [DOI] [Google Scholar]
- 14.Jaiswal A, Aldersey H, Wittich W, Mirza M. Conducting Qualitative Research With Individuals Living With Deafblindness. Thousand Oaks, CA: Sage Publications Ltd; 2020. [Google Scholar]
- 15.Wittich W, Granberg S, Wahlqvist M, Pichora-Fuller MK, Mäki-Torkko E. Device abandonment in deafblindness: a scoping review of the intersection of functionality and usability through the International Classification of Functioning, Disability and Health lens. BMJ Open 2021;11:e044873. https://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=33495263&dopt=Abstract 10.1136/bmjopen-2020-044873 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Janssen MJ, Hartshorne TS, Wittich W. Editorial: Development, Wellbeing, and Lifelong Learning in Individuals With a Dual Sensory Loss. Front Psychol 2021;12:790549. https://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=34956018&dopt=Abstract 10.3389/fpsyg.2021.790549 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Roy A, McVillly KR, Crisp BR. Working with Deafblind people to develop a good practice approach. J Soc Work (Lond) 2019;21:69–87. 10.1177/1468017319860216 [DOI] [Google Scholar]
- 18.Simcock P, Manthorpe J, Tinker A. A salutogenesis approach to ageing with impairment: the managing and coping experiences of older people ageing with deafblindness. Ageing Soc 2023;43:2957–82. 10.1017/S0144686X22000083 [DOI] [Google Scholar]
- 19.Jaiswal A, Fraser S, Wittich W. Barriers and facilitators that influence social participation in older adults with dual sensory impairment. Front Educ (Lausanne) 2020;5:127. 10.3389/feduc.2020.00127 [DOI] [Google Scholar]
- 20.Watharow A. Improving the Experience of Health Care for People Living with Sensory Disability: Knowing What Is Going On. New York, NY: Lived Places Publishing; 2023. [Google Scholar]
- 21.Chahraborty I. To “The other senses”: A dialogue between visual arts and visual disability. International Research Journal Persons with Special Needs and Rehabilitation Managment. 2018;4:1–8. [Google Scholar]
- 22.Fukushima S. The deafblind and disability studies. In: Creating a Society for All: Disability and Economy. The Disability Press; 2012:70-81. [Google Scholar]
- 23.Nuccio J, Smith TB. Providing and Receiving Support Services: Comprehensive Training for Deaf-Blind Persons and Their Support Service Providers. Deafblind Service Center; 2010. [Google Scholar]
- 24.Clark JL. Where I Stand : On the Signing Community and My DeafBlind Experience. New York, NY: Handtype Press; 2014. [Google Scholar]
- 25.Brede KS, Souriau J. Let Me Join Your Tactile Attention: A Sign Language Perspective on the Communicative Togetherness with a Child who is Congenitally Deafblind. Journal of Deafblind Studies on Communication. 2016;2:4–21. [Google Scholar]
- 26.Liston LM. How to Become a Bridge, not a Barrier: Building Peer Relationships for a Young Man with Congenital Deafblindness using Multiparty Interactions in the Tactile Modality. DbI Review. 2021;65:2024. [Google Scholar]
- 27.Hartshorne TS, Schmittel MC. Social-Emotional Development in Children and Youth Who Are Deafblind. Am Ann Deaf 2016;161:444–53. https://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=27818400&dopt=Abstract 10.1353/aad.2016.0036 [DOI] [PubMed] [Google Scholar]
- 28.Wolff Heller K, Gallagher PA, Fredrick LD. Parents’ Perceptions of Siblings’ Interactions With Their Brothers and Sisters Who Are Deaf-Blind. Volume 24. Thousand Oaks, CA: Sage Publications Ltd; 1999. [Google Scholar]
- 29.Huus K, Sundqvist AS, Anderzén-Carlsson A, Wahlqvist M, Björk M. Living an ordinary life - yet not: the everyday life of children and adolescents living with a parent with deafblindness. Int J Qual Stud Health Well-being 2022;17:2064049. https://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=35437116&dopt=Abstract 10.1080/17482631.2022.2064049 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Jaiswal A, Aldersey HM, Wittich W, Mirza M, Finlayson M. Using the ICF to identify contextual factors that influence participation of persons with deafblindness. Arch Phys Med Rehabil 2019;100:2324–33. https://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=30986411&dopt=Abstract 10.1016/j.apmr.2019.03.010 [DOI] [PubMed] [Google Scholar]
- 31.Crowe K, Hovaldt HB, Dammeyer J. Communication participation in older adults with dual sensory loss. Speech Lang Hear 2020;23:232–42. 10.1080/2050571X.2019.1623457 [DOI] [Google Scholar]
- 32.Möller K. Deafblindness: a challenge for assessment—is the ICF a useful tool? Int J Audiol 2003;42(Suppl 1):S140–2. https://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=12918621&dopt=Abstract 10.3109/14992020309074635 [DOI] [PubMed] [Google Scholar]
- 33.Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care 2007;19:349–57. https://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=17872937&dopt=Abstract 10.1093/intqhc/mzm042 [DOI] [PubMed] [Google Scholar]
- 34.Patton MQ. Qualitative Research and Evaluation Methods: Theory and Practice. 4th ed. Thousand Oaks, CA: Sage Publications Ltd; 2015. [Google Scholar]
- 35.Paramasivam A, Jaiswal A, Minhas R, Wittich W, Spruyt-Rocks R. Informed Consent or Assent Strategies for Research With Individuals With Deafblindness or Dual Sensory Impairment: A Scoping Review. Arch Rehabil Res Clin Transl 2021;3:100115. https://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=34179751&dopt=Abstract 10.1016/j.arrct.2021.100115 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Cieza A, Fayed N, Bickenbach J, Prodinger B. Refinements of the ICF Linking Rules to strengthen their potential for establishing comparability of health information. Disabil Rehabil 2019;41:574–83. https://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=26984720&dopt=Abstract 10.3109/09638288.2016.1145258 [DOI] [PubMed] [Google Scholar]
- 37.Cieza A, Geyh S, Chatterji S, Kostanjsek N, Ustün B, Stucki G. ICF linking rules: an update based on lessons learned. J Rehabil Med 2005;37:212–8. https://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=16024476&dopt=Abstract 10.1080/16501970510040263 [DOI] [PubMed] [Google Scholar]
- 38.Granberg S, Pronk M, Swanepoel W, Kramer SE, Hagsten H, Hjaldahl J, et al. The ICF core sets for hearing loss project: functioning and disability from the patient perspective. Int J Audiol 2014;53:777–86. https://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=25311099&dopt=Abstract 10.3109/14992027.2014.938370 [DOI] [PubMed] [Google Scholar]
- 39.Billiet L, van Nispen RM, De Baets S, de Vries R, Van de Velde D, van der Aa HP. The first step in developing an International Classification of Functioning, Disability and Health Core Set for Vision Loss: A systematic review. Ophthalmic Physiol Opt 2024;44:413–25. https://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=38251457&dopt=Abstract 10.1111/opo.13269 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Hartshorne TS, Slavin LJ. CHARGE syndrome. In: Perfect WW, Riccio CA, Bray MA, editors. Health-Related Disorders in Children and Adolescents: A Guidebook for Educators and Service Providers. American Psychological Association; 2023. p. 453–9. [Google Scholar]
- 41.Di Matteo A, Bathon JM, Emery P. Rheumatoid arthritis. Lancet 2023;402:2019–33. https://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=38240831&dopt=Abstract 10.1016/S0140-6736(23)01525-8 [DOI] [PubMed] [Google Scholar]
- 42.Bruce SM, Nelson C, Perez A, Stutzman B, Barnhill BA. The State of Research on Communication and Literacy in Deafblindness. Am Ann Deaf 2016;161:424–43. https://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=27818399&dopt=Abstract 10.1353/aad.2016.0035 [DOI] [PubMed] [Google Scholar]
- 43.Guthrie DM, Williams N, Campos J, Mick P, Orange JB, Pichora-Fuller MK, et al. A Newly Identified Impairment in Both Vision and Hearing Increases the Risk of Deterioration in Both Communication and Cognitive Performance. Can J Aging 2022;41:363–76. https://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=35859361&dopt=Abstract 10.1017/S0714980821000313 [DOI] [PubMed] [Google Scholar]
- 44.Guthrie DM, Davidson JG, Williams N, Campos J, Hunter K, Mick P, et al. Combined impairments in vision, hearing and cognition are associated with greater levels of functional and communication difficulties than cognitive impairment alone: analysis of interRAI data for home care and long-term care recipients in Ontario. PLoS One 2018;13:e0192971. https://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=29447253&dopt=Abstract 10.1371/journal.pone.0192971 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.World Federation of the Deafblind. Deafblindness and the SDGs [Internet]. Available from: https://wfdb.eu/deafblindness-and-the-sdgs/ [cited 2024, Feb 18].
- 46.Wittich W, Simcock P. Aging and combined vision and hearing loss. In: Ravenscroft J, ed. The Routledge Handbook of Visual Impairment. London: Routledge Taylor & Francis Group; 2019. p. 438-56. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supplementary Table I
Identified ICF codes from the Body Functions (b) category mentioned by the participants per sub-level.
Supplementary Table II
Identified ICF codes from the Body Structures (s) category mentioned by the participants per sub-level.
Supplementary Table III
Identified ICF codes from the Activities & Participation (d) category mentioned by the participants per sub-level.
Supplementary Table IV
Identified ICF codes from the Environmental Factors (e) category mentioned by the participants per sub-level.
Supplementary Table V
Identified personal factors relevant to deafblindness and their frequency.