

Abstract
Objective: To investigate the efficacy of the SaCo videolaryngeal mask airway (VLMA) in combination with a bronchial blocker in patients undergoing minimally invasive thoracoscopic surgery. Methods: A retrospective analysis was conducted on the clinical data of 120 patients who underwent minimally invasive thoracoscopic surgery from January 2022 to December 2023. Patients were grouped based on their treatment methods: 68 patients who received the SaCo VLMA combined with a bronchial blocker intraoperatively were designated as the L group, while 52 patients who received a tracheal tube combined with a bronchial blocker intraoperatively were designated as the E group. Heart rate (HR) and mean arterial pressure (MAP) were compared between the two groups at several time points: prior to anesthesia induction (P1), immediately after anesthesia induction (P2), 1 minute after the insertion of the tracheal tube or placement of the laryngeal mask airway (P3), and 1 minute after the removal of the tracheal tube or laryngeal mask airway (P4). Additionally, the following parameters were recorded and compared: peak airway pressure (Ppeak), airway plateau pressure (Pplat), and pulse oxygen saturation (SpO2) at various time points: 5 minutes after the insertion of the tracheal tube or placement of the laryngeal mask airway (T1), 3 minutes after two-lung ventilation (T2), 5 minutes after one-lung ventilation (T3), and 1 hour after one-lung ventilation (T4). Other observations included the degree of lung collapse during surgery, awakening quality, time to extubation or removal of the laryngeal mask airway, overall recovery quality, and incidence of complications. Results: Compared to the E group, the L group exhibited significantly higher HR and MAP at time points P2, P3, and P4 (P < 0.05). The L group also demonstrated lower Ppeak and Pplat levels from T1 to T4 compared to the E group (P < 0.05). There was no significant difference in SpO2 levels between the two groups from T1 to T4 (P > 0.05). The time to removal of the tracheal tube or laryngeal mask airway was significantly shorter in the L group than in the E group (P < 0.05). The utilization rate of vasoactive drugs was lower in the L group compared to the E group (P < 0.05). The modified Aldrete recovery scores at 30 minutes and 2 hours postoperatively were significantly higher in the L group than in the E group (P < 0.05). The Quality of Recovery Scale (QoR-15) score at 24 hours postoperatively was also higher in the L group compared to the E group (P < 0.05). Furthermore, the incidence of complications was significantly lower in the L group than in the E group (P < 0.05). Conclusion: The use of the SaCo videolaryngeal mask airway combined with a bronchial blocker in minimally invasive thoracoscopic surgery, compared to tracheal tube placement, can effectively reduce the requirement for vasoactive drugs, improve ventilation outcomes, stabilize hemodynamics, accelerate postoperative awakening, reduce the incidence of postoperative complications, and enhance the quality of postoperative awakening. These findings highlight the potential of this approach as a valuable reference for clinical practice.
Keywords: Minimally invasive thoracoscopic surgery, SaCo videolaryngeal mask airway, bronchial blocker, quality of recovery, medication usage, complications
Introduction
One-lung ventilation (OLV) is a lung isolation technique employed by anesthesiologists for patients undergoing minimally invasive thoracoscopic surgery. This technique facilitatess the collapse of the lung in the surgical field, enabling clear delineation of the lesion and providing the surgeon with a clear and stable operative field. Additionally, it reduces mechanical injury to the non-resected lung and protects the healthy lung from infection [1,2]. Studies have indicated that effective lung isolation is crucial for the successful execution of minimally invasive thoracoscopic surgery [3]. In recent years, OLV is typically achieved through the use of tracheal tubes combined with bronchial blockers or double-lumen bronchial catheters. However, despite the widespread use of endotracheal tubes in OLV, several limitations persist. Firstly, tracheal intubation is a highly invasive procedure that can trigger a stress response in patients, resulting in hemodynamic instability during surgery [4]. Secondly, the insertion of tracheal tubes may increase the risk of mechanical injury to the respiratory tract, which can adversely affect ventilation efficacy. Moreover, postoperative recovery may be hampered by discomfort and airway irritation associated with tracheal tubes, potentially delaying awakening and recovery quality. This concern is particularly relevant for elderly patients or those with chronic respiratory conditions, as tracheal tube usage often correlates with an increased incidence of postoperative complications and a negative impact on rehabilitation. Therefore, there is a pressing need for more efficient OLV tools in clinical practice.
The SaCo visual laryngeal mask airway represents the latest advancement in laryngeal mask technology. As a novel airway management tool, it is anticipated to serve as a viable alternative to endotracheal tubes due to its non-invasive nature, visual guidance capabilities, and stable ventilation performance, thereby enhancing respiratory management in minimally invasive thoracoscopic surgery. This method offers multiple functions, including esophageal drainage and tracheal intubation, along with visual guidance. Numerous studies have reported that the SaCo visual laryngeal mask airway can achieve stable ventilation during surgical procedures, demonstrating its efficacy in various traumatic operations [5]. In this study, we applied the SaCo visual laryngeal mask airway in combination with a bronchial blocker for the first time in minimally invasive thoracoscopic surgery, and systematically evaluated its clinical value in terms of anesthesia management, ventilation quality, hemodynamic stability, and postoperative recovery. Through a multi-dimensional evaluation, indicators such as heart rate, blood pressure, airway pressure, and pulse oxygen saturation, the advantages of this technology in improving intraoperative ventilation, reducing postoperative complications, accelerating awakening and enhancing recovery quality were comprehensively discussed. The findings are presented below.
Materials and methods
General data
A retrospective analysis was conducted on the clinical data of 120 patients who underwent minimally invasive thoracoscopic surgery from January 2022 to December 2023. Based on the different treatment methods, the patients were divided into two groups: the L group (68 patients, using the SaCo videolaryngeal mask airway combined with a bronchial blocker) and the E group (52 patients, using a tracheal tube combined with a bronchial blocker). This study has been approved by the Ethics Committee of Xidian Group Hospital. The sample size for each group was determined using a sample size calculation formula. We hypothesized that the SaCo videolaryngeal mask airway combined with a bronchial blocker would result in significant improvements in hemodynamic stability, ventilation quality, and postoperative recovery compared to the tracheal tube with a bronchial blocker. Based on effect sizes reported in previous literature, we set a significance level (α) of 0.05 and a test power of 0.80. A bilateral t-test indicated that a minimum sample size of approximately 50 cases was required in each group. To account for potential loss to follow-up or data loss, we included a slightly larger number of patients in each group: 68 in the L group and 52 in the E group.
Inclusion criteria and exclusion criteria
Inclusion criteria
Patients were included in the study based on the following criteria: (1) Individuals scheduled for elective, non-emergency unilateral minimally invasive thoracoscopic surgery [6]. (2) Classified as Grade I to II by the American Society of Anesthesiologists (ASA). (3) Demonstrating normal cognitive function and audiovisual abilities, allowing for effective communication. (4) Exhibiting stable vital signs. (5) Having complete clinical data.
Exclusion criteria
Patients were excluded from the study if they met any of the following criteria: (1) Presence of severe cardiovascular, cerebrovascular, or pulmonary diseases, or liver or renal insufficiency. (2) Chest CT findings indicating a distance of less than 2 cm from the opening of the right upper lung to the carina. (3) Mouth opening of less than two fingerbreadths or a history of difficult intubation. (4) Circulatory system diseases or a history of airway allergies. (5) Undergoing conversion to open thoracotomy. (6) Contraindications to the use of a laryngeal mask airway or tracheal tube, including abnormal neck and throat anatomy, limited neck mobility, or a difficult airway. (7) Presence of uncontrolled infectious or contagious diseases.
Methods
Both groups underwent a comprehensive preoperative assessment, including medical history collection and physical examination, to exclude any surgical contraindications. Patients were instructed to fast for 8 hours and to abstain from oral intake for 4 hours before surgery. Upon entering the operating room, an indwelling cannula was placed in a peripheral vein of the upper limb, and radial artery catheterization was performed under local anesthesia. A multifunctional monitor was employed to closely monitor vital parameters, including pulse oxygen saturation (SpO2), electrocardiogram (ECG), mean arterial pressure (MAP), heart rate (HR), and bispectral index (BIS). An intravenous pre-infusion of approximately 500 ml of Compound Sodium Chloride Injection (CR Double-Crane Pharmaceuticals Co., Ltd., 230414) was administered. Anesthesia induction was achieved with intravenous injections of midazolam (Jiangsu Nhwa Pharmaceutical Co., Ltd., 0.04 mg/kg, TMZ23L09), sufentanil (Yichang Humanwell Pharmaceutical Co., Ltd., 0.4 μg/kg, 21A07011), etomidate (Jiangsu Nhwa Pharmaceutical Co., Ltd., 0.2 mg/kg, TYT23A39), and rocuronium bromide (Hainan Star Pharmaceutical Co., Ltd., 0.9 mg/kg, 2312060A).
Anesthesia maintenance: Anesthesia maintenance was achieved using a target-controlled infusion of Propofol Injectable Emulsion (Jiabo Pharmaceutical, 2A230422) to attain a plasma concentration of 2-3 ng/ml, alongside remifentanil hydrochloride (Yichang Humanwell Pharmaceutical Co., Ltd., 20A04231) infused to achieve a plasma concentration of 2-4 ng/ml. Rocuronium bromide was administered at a dose of 0.1 mg/kg every 40 minutes to maintain muscle relaxation, aiming to keep the BIS value between 40 and 60 [7]. Following satisfactory muscle relaxation and an adequate depth of anesthesia (BIS < 60), either tracheal intubation or insertion of the laryngeal mask airway was performed [8]. For the L group, the SaCo videolaryngeal mask airway (VLMA) was initially inserted. After thoroughly clearing the patient’s oral secretions, the head was positioned in the midline, and the operator assisted the patient in opening their mouth. The prepared SaCo VLMA was then introduced into the oral cavity, with the back of the patient’s neck elevated to extend the head backward. The mask’s cuff was advanced along the palate to the arytenoid cartilage and posterior commissure, ensuring it was positioned behind the arytenoid cartilage and toward the glottic structures, perpendicular to the patient’s chest. The laryngeal mask airway (LMA) was connected to the anesthesia machine. If glottic structures were clearly visible and ventilation was effective, the LMA was considered successfully placed, and the bronchial blocker was inserted under visual guidance. In the E group, tracheal intubation was performed with the assistance of a video laryngoscope. Once the correct position of the tracheal tube was confirmed, it was secured, and the bronchial blocker was inserted blindly. In both groups, after 3 minutes of pure oxygen ventilation to both lungs, the bronchus was blocked for OLV. Mechanical ventilation was then initiated in volume-controlled ventilation (VCV) mode. Throughout the procedure, the patient’s lung collapse, peak airway pressure (Ppeak), and airway plateau pressure (Pplat) were closely monitored to ensure adequate ventilation. If necessary, a fiberoptic bronchoscope was used to verify the position of the bronchial blocker. Following the completion of OLV, the bronchial blocker was removed. At the end of the surgery, all intravenous anesthetic agents were discontinued, and anesthesia was terminated. The collapsed lung was re-expanded using a continuous lung inflation method. The patient was then transferred to the post-anesthesia care unit (PACU). Once the patient’s vital signs stabilized and no anesthesia-related complications were noted, the patient was returned to the general ward.
Observation indicators
Intraoperative indicators
The following intraoperative indicators were recorded and compared between the two groups: surgery duration, intraoperative OLV duration, and anesthesia maintenance time.
Hemodynamic indicators
Heart rate (HR) and mean arterial pressure (MAP) were recorded and compared at the following time points: prior to anesthesia induction (P1), immediately after anesthesia induction (P2), 1 minute after the insertion of the tracheal tube or placement of the laryngeal mask airway (P3), and 1 minute after the removal of the laryngeal mask airway or tracheal tube (P4).
Ventilation indicators
Pplat, Ppeak, and pulse oxygen saturation (SpO2) were recorded and compared at the following time points: 5 minutes after the insertion of the tracheal tube or placement of the laryngeal mask airway (T1), 3 minutes after two-lung ventilation (T2), 5 minutes after one-lung ventilation (T3), and 1 hour after one-lung ventilation (T4).
Lung collapse condition and time to remove tracheal tube or laryngeal mask airway
Following OLV, the degree of lung collapse was assessed using the Verbal Rating Scale, which ranges from 0 to 10 [9]. Higher scores indicate more effective lung collapse and optimal surgical operating space. Additionally, the time from the cessation of intravenous drug infusion to the removal of the tracheal tube or laryngeal mask airway was recorded and compared between the two groups.
Vasoactive drug usage
The number of patients requiring vasoactive drugs after the placement and removal of the tracheal tube or laryngeal mask airway was recorded.
Awakening quality
The modified Aldrete recovery score was used to evaluate the quality of awakening at 30 minutes and 2 hours postoperatively [10]. This scale includes seven items, each scored from 0 to 2 points, yielding a total score ranging from 0 to 14 points. Higher scores indicate better awakening quality.
Quality of recovery
The quality of recovery was assessed using the Quality of Recovery-15 (QoR-15) scale at 24 hours before and after surgery [8]. This scale includes 15 items, each scored from 0 to 10 points, with a total score ranging from 0 to 150 points. Higher scores reflect better early recovery quality.
Incidence of complications
The incidence of complications was recorded and compared between the two groups, including pharyngeal bleeding, hoarseness, coughing, sore throat, and bronchospasm.
Statistical methods
SPSS 22.0 software was used for statistical analysis. Complications were expressed as n (%) and analyzed using the χ2 test. Intraoperative indicators, hemodynamic indicators, ventilation indicators, lung collapse condition, time to remove the tracheal tube or laryngeal mask airway, and scores for awakening and recovery quality were presented as mean ± standard deviation (x̅±S) and analyzed using the t-test. A P-value of less than 0.05 was considered statistically significant.
Results
Comparison of baseline data between the two groups
The baseline data of the two groups were well balanced, with no significant differences (P > 0.05), indicating comparability (Table 1).
Table 1.
Comparison of baseline data between the two groups
| Group | Gender (Male/Female) | Average age (years) | Body Mass index (kg/m2) | ASA I/II |
|---|---|---|---|---|
| L group (n=68) | 37/31 | 40.84±3.26 | 21.56±1.45 | 46/22 |
| E group (n=52) | 29/23 | 40.57±2.78 | 22.03±1.47 | 39/13 |
| t | 0.022 | 0.656 | 1.759 | 0.771 |
| P | 0.882 | 0.513 | 0.081 | 0.380 |
ASA, American Society of Anesthesiologists.
Intraoperative indicators
There were no significant differences between the two groups in terms of surgery duration, intraoperative OLV duration, or anesthesia maintenance time (P > 0.05) (Figure 1).
Figure 1.
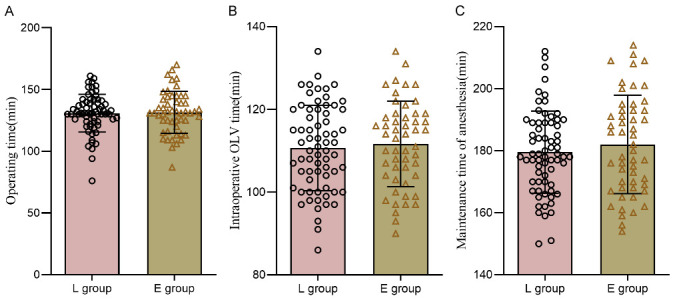
Comparison of intraoperative indexes between the two groups. A: Operation time; B: Intraoperative OLV time; C: Duration of anesthesia maintenance. OLV: One-lung ventilation.
Hemodynamic indicators
There were no significant differences in HR or MAP between the two groups at P1 (P > 0.05). However, the L group had significantly higher HR and MAP compared to the E group at P2, P3, and P4 (P < 0.05) (Table 2).
Table 2.
Comparison of hemodynamic indexes between the two groups (x̅±S)
| Indicators | Time | L group (n=68) | E group (n=52) | t | P |
|---|---|---|---|---|---|
| HR (times/min) | P1 | 92.27±9.40 | 91.86±10.74 | 0.223 | 0.824 |
| P2 | 87.46±8.64a | 85.73±8.84a | 1.076 | 0.284 | |
| P3 | 82.28±8.36a,b | 79.41±6.72a,b | 2.025 | 0.045 | |
| P4 | 75.24±6.56a,b,c | 70.94±8.47a,b,c | 3.080 | 0.003 | |
| MAP (mmHg) | P1 | 99.14±10.25 | 98.82±9.52 | 0.175 | 0.862 |
| P2 | 95.42±9.63a | 90.24±9.58a | 2.927 | 0.004 | |
| P3 | 90.26±8.71a,b | 84.75±8.26a,b | 3.511 | 0.001 | |
| P4 | 85.05±6.57a | 80.45±6.24a,b,c | 3.884 | < 0.001 |
Note: Compared with P1 in this group;
P < 0.05.
Compared with P2 in this group;
P < 0.05.
Compared with P3 in this group;
P < 0.05.
HR, Heart rate; MAP, mean arterial pressure; P1, prior to anesthesia induction; P2, immediately after anesthesia induction; P3, 1 minute after the insertion of the tracheal tube or placement of the laryngeal mask airway; P4, 1 minute after the removal of the tracheal tube or laryngeal mask airway.
Ventilation indicators
The L group exhibited significantly lower Ppeak and Pplat compared to the E group from T1 to T4 (P < 0.05). No significant differences were observed in SpO2 levels between the two groups during these time points (P > 0.05) (Table 3).
Table 3.
Comparison of ventilation indexes between the two groups (x̅±S)
| Indicators | Time | L group (n=68) | E group (n=52) | t | P |
|---|---|---|---|---|---|
| Ppeak (cmH2O) | T1 | 16.26±1.45 | 19.25±1.74 | 10.260 | < 0.001 |
| T2 | 18.46±1.54a | 22.73±1.84a | 13.828 | < 0.001 | |
| T3 | 19.28±1.36a,b | 23.41±1.22a,b | 17.228 | < 0.001 | |
| T4 | 20.24±1.56a,b,c | 23.94±1.47a,b,c | 13.198 | < 0.001 | |
| Pplat (cmH2O) | T1 | 12.14±1.20 | 15.20±1.26 | 13.545 | < 0.001 |
| T2 | 14.42±1.13a | 17.24±1.18a | 13.290 | < 0.001 | |
| T3 | 15.26±1.21a,b | 18.75±1.26a,b | 15.379 | < 0.001 | |
| T4 | 16.05±1.17a,b,c | 19.45±1.24a,b,c | 15.371 | < 0.001 | |
| SpO2 (%) | T1 | 99.24±0.24 | 99.28±0.39 | 0.692 | 0.490 |
| T2 | 99.05±0.24 | 99.04±0.24 | 0.226 | 0.822 | |
| T3 | 98.35±0.48 | 98.18±0.57 | 1.772 | 0.079 | |
| T4 | 95.82±0.37 | 95.95±0.65 | 1.383 | 0.169 |
Note: Compared with T1 in this group;
P < 0.05.
Compared with T2 in this group;
P < 0.05.
Compared with T3 in this group;
P < 0.05.
Ppeak, peak airway pressure; Pplat, airway plateau pressure; SpO2, pulse oxygen saturation; T1, 5 minutes after the insertion of the tracheal tube or placement of the laryngeal mask airway; T2, 3 minutes after two-lung ventilation; T3, 5 minutes after one-lung ventilation; T4, 1 hour after one-lung ventilation.
Lung collapse condition and time to remove tracheal tube or laryngeal mask airway
There were no significant differences in lung collapse conditions between the two groups (P > 0.05). However, the time to remove the tracheal tube or laryngeal mask airway was significantly shorter in the L group compared to the E group (P < 0.05) (Figure 2).
Figure 2.
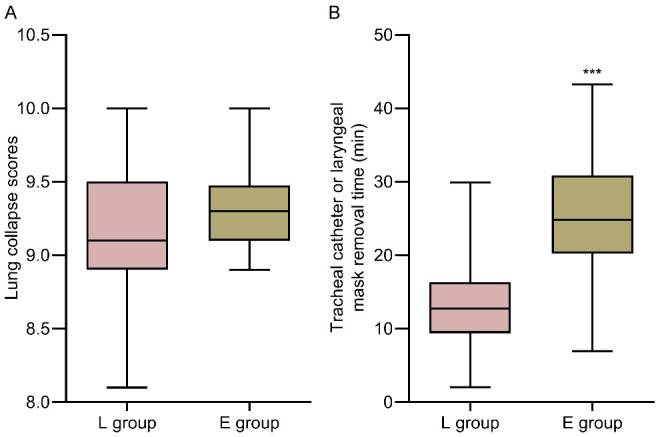
Comparison of lung collapse and time of tracheal catheter or laryngeal mask removal between the two groups. A: Collapsed lung; B: Time to remove tracheal catheter or laryngeal mask. Compared with L group, ***P < 0.001.
Vasoactive drug usage
The incidence of vasoactive drug usage was significantly lower in the L group at 1.47% (1/68) compared to 13.46% (7/52) in the E group (χ2=5.018, P=0.025).
Awakening quality
The modified Aldrete recovery scores at 30 minutes and 2 hours postoperatively were significantly higher in the L group compared to the E group (P < 0.05) (Table 4).
Table 4.
Comparison of awakening quality between the two groups (x̅±S, score)
| Group | 30 min after operation | 2 hours after operation | t | P |
|---|---|---|---|---|
| L group (n=68) | 9.15±0.49 | 12.35±0.73 | 30.013 | < 0.001 |
| E group (n=52) | 8.17±0.52 | 10.55±0.62 | 21.209 | < 0.001 |
| t | 10.572 | 14.272 | ||
| P | < 0.001 | < 0.001 |
Recovery quality
There were no significant differences in QoR-15 scores between the two groups 24 hours before surgery (P > 0.05). However, the QoR-15 scores at 24 hours postoperatively were significantly higher in the L group compared to the E group (P < 0.05) (Table 5).
Table 5.
Comparison of recovery quality between the two groups (x̅±S, score)
| Group | 30 min after operation | 2 hours after operation | t | P |
|---|---|---|---|---|
| L group (n=68) | 141.18±10.45 | 102.37±7.70 | 24.655 | < 0.001 |
| E group (n=52) | 140.19±10.55 | 90.55±6.59 | 28.777 | < 0.001 |
| t | 0.512 | 8.861 | ||
| P | 0.610 | < 0.001 |
Incidence of complications
The incidence of complications was significantly lower in the L group compared to the E group (P < 0.05) (Table 6).
Table 6.
Comparison of complication rates between the two groups n (%)
| Group | Throat hemorrhage | Hoarse | Choking | Sore throat | Bronchospasm | Total |
|---|---|---|---|---|---|---|
| L group (n=68) | 0 (0.00) | 0 (0.00) | 1 (1.47) | 0 (0.00) | 0 (0.00) | 1 (1.47) |
| E group (n=52) | 1 (1.92) | 2 (3.85) | 2 (3.85) | 2 (3.85) | 1 (1.92) | 8 (15.38) |
| χ2 | 6.340 | |||||
| P | 0.012 |
Discussion
Minimally invasive thoracoscopic surgery offers several advantages over traditional open thoracotomy, including less trauma, more controllable and reduced bleeding, enhanced clarity of the surgical field, lower postoperative pain, minimal impact on lung and immune function, and fewer postoperative complications. In recent years, this approach has gained increased recognition, and its clinical application has steadily risen. The effectiveness of OLV is crucial for the success of minimally invasive thoracoscopic surgery.
Currently, the most commonly used tools for OLV in minimally invasive thoracoscopic surgery are tracheal tubes and bronchial blockers. Tracheal tubes facilitate lung isolation, allowing for independent anesthesia and ventilation of each lung, as well as the selective removal of secretions from both lungs. When used in conjunction with bronchial blockers, they optimize lung isolation effectiveness [11,12]. However, some studies indicate that successful tracheal tube insertion necessitates glottic exposure via laryngoscopy. The placement or removal of the tracheal tube can stimulate receptors in the epiglottis, tongue base, and pharyngeal tissues, triggering activation of the sympathoadrenal medullary system and inducing a stress response. This may result in significant hemodynamic fluctuations during surgery and adversely affect ventilation quality, thereby increasing the risk of both intraoperative and postoperative complications, which is detrimental to early recovery [13].
Studies have indicated that, compared to tracheal tubes, the insertion of a bronchial blocker using the SaCo videolaryngeal mask airway (VLMA) is simpler, has a higher success rate, and is safer [14]. The results of this study showed that HR and MAP were significantly higher in the L group compared to the E group at P2, P3, and P4. Additionally, the incidence of vasoactive drug usage was lower in the L group than in the E group. These findings suggest that the combined application of the SaCo VLMA and bronchial blocker in minimally invasive thoracoscopic surgery can effectively stabilize hemodynamic parameters while reducing the reliance on vasoactive drugs. Research by Wang Ruiling et al. demonstrates that the use of a tracheal blocker can enhance surgical field visibility in thoracoscopic procedures while resulting in minimal hemodynamic changes; however, HR and MAP significantly increase during intubation and extubation [15]. This observation aligns with the outcomes noted in patients of the E group in our study. Conversely, patients in the L group, who received the SaCo VLMA, exhibited more stable hemodynamics following anesthesia induction, alongside a significant reduction in the use of vasoactive drugs. The reasons for these findings are analyzed as follows: (1) Tracheal intubation requires the use of a laryngoscope, which may lead to prolonged placement of a tracheal tube to continuously stimulate the airway mucosa. The removal of the tracheal tube also stimulates and potentially injures the glottis and airway mucosa, triggering a stress response that results in catecholamine release and subsequent hemodynamic fluctuations [16]. In contrast, the SaCo VLMA does not require tracheal insertion and can be positioned accurately using its visual guidance feature without lifting the epiglottis or irritating the glottis. This reduces damage to the pharyngeal tissues and airway mucosa, thereby minimizing hemodynamic changes during surgery [17]. (2) The design of the SaCo VLMA, characterized by its sloped front end and 70° rigidity, facilitates quicker and more convenient placement of the bronchial blocker, thereby reducing the stress response associated with its insertion and helping to stabilize intraoperative hemodynamic parameters [18]. (3) With hemodynamic parameters maintained within a stable range throughout the procedure, the need for vasoactive drugs is significantly reduced, resulting in less frequent drug administration of these medications.
A foreign study indicated that a Pplat greater than 35 cm H2O is likely to cause alveolar overdistension and associated lesions [19]. In clinical practice, maintaining end-tidal CO2 concentration or partial pressure within acceptable limits requires continuous adjustment of ventilator parameters to ensure that the Pplat remains within normal ranges. Generally, during minimally invasive thoracoscopic surgery, where only one lung is ventilated to achieve effective lung isolation, there is a risk of decreased lung compliance, reduced functional residual capacity, and insufficient ventilation, all of which can contribute to increased ventilation parameters such as Ppeak and Pplat [20]. However, the results of this study showed that the L group had significantly lower Ppeak and Pplat levels compared to the E group from T1 to T4. These findings indicate that the combined use of the SaCo VLMA and bronchial blocker in minimally invasive thoracoscopic surgery can effectively reduce ventilation pressures and improve intraoperative ventilation outcomes. Several factors may contribute to these results: (1) The SaCo VLMA allows for real-time observation and management of secretions at the mask’s front end during surgery. This capability helps ensure airtightness and smooth ventilation, effectively controlling increases in Ppeak and Pplat levels and thereby maintaining optimal ventilation quality [21]. (2) Unlike tracheal tubes, which require insertion into the airway and occupy airway space, the laryngeal mask airway does not obstruct the ventilation pathway. This results in lower airway resistance and higher tidal volume during ventilation, which facilitates more efficient gas exchange and oxygenation while promoting the rapid expulsion of CO2. Consequently, the SaCo VLMA aids in controlling Ppeak and Pplat levels, enhances lung compliance, and improves ventilation conditions [22].
The results of this study showed that the time to remove the tracheal tube or laryngeal mask airway in the L group was significantly shorter than in the E group. Additionally, the modified Aldrete recovery scores at 30 minutes and 2 hours postoperatively were higher in the L group compared to the E group. These findings suggest that the combined use of the SaCo VLMA and bronchial blocker in minimally invasive thoracoscopic surgery not only facilitates shorter removal times for airway devices but also enhances awakening quality. Several factors may explain these findings: the placement of the SaCo VLMA is simpler and safer, resulting in a reduced requirement for anesthetic agents during surgery. Consequently, patients experience a smoother, awakening process, which contributes to a higher quality of awakening and shorter time to remove the tracheal tube or laryngeal mask airway. Furthermore, the QoR-15 scale, a comprehensive evaluation tool for assessing the psychological state, pain levels, and physiological adaptation of patients undergoing traumatic surgeries, revealed that the QoR-15 scores at 24 hours postoperatively were higher in the L group compared to the E group. Moreover, the incidence of complications in the L group was significantly lower than in the E group. These findings further corroborate that the combined approach results in better postoperative recovery quality and a lower incidence of complications. Possible explanations for these results include the nature of tracheal intubation, which involves the insertion of a relatively rigid tube without direct visualization of the pharynx and larynx. Even minor misplacements can stimulate or injure the oropharyngeal area, significantly increasing the risk of complications such as pharyngeal bleeding, hoarseness, coughing during awakening period, sore throat, and bronchospasm. In contrast, the SaCo VLMA is made of softer material, which reduces irritation to the soft tissues and mucosa of the mouth and throat during insertion. As a supraglottic airway device, the VLMA does not impact the vocal cords or airway mucosa, resulting in a significantly lower incidence of coughing, sore throat, and hoarseness during the awakening period [23]. The lower complication rates observed in patients using the SaCo VLMA contribute to a shorter hospital stay and promote rapid recovery, ultimately leading to a better postoperative recovery quality.
There are some limitations to this study. First, the sample size was small, and the results of single-center retrospective analysis were limited in generalization and statistical efficacy. Our results can be verified by multi-center studies with larger sample sizes in the future. Second, this study only observed the quality of recovery and complications within 24 hours after surgery, and did not conduct long-term follow-up, and thus is lacking assessment of long-term complications and lung function recovery. In addition, the study did not analyze the impact of individual differences such as age, body mass index, and underlying medical conditions on the results, which may have influenced the anesthetic effect and postoperative recovery to some extent. Finally, this study only compared the effect of SaCo visual laryngeal mask with traditional tracheal catheter, and did not include a comparison of other ventilation management methods, which may limit the universality of the results. Therefore, future large-scale, multi-center prospective studies are needed to more comprehensively evaluate the efficacy and safety of SaCo visual laryngeal mask in minimally invasive thoracoscopic surgery.
In conclusion, the combined use of the SaCo VLMA and bronchial blocker in minimally invasive thoracoscopic surgery can effectively reduce the requirement for vasoactive drugs, improve ventilation outcomes, stabilize hemodynamic parameters, accelerate postoperative awakening, reduce the incidence of complications, and enhance the quality of postoperative recovery. This approach provides valuable insights for clinical practice.
Disclosure of conflict of interest
None.
References
- 1.Leonardi B, Forte S, Natale G, Messina G, Rainone A, Opromolla G, Puca MA, Grande M, Martone M, Leone F, Fiorito R, Molino F, Liguori G, Russo F, Ferraro F, Pace MC, Molino A, Ferrante L, Forte M, Vicidomini G, Fiorelli A. One-lung ventilation in obese patients undergoing thoracoscopic lobectomy for lung cancer. Thorac Cancer. 2023;14:281–288. doi: 10.1111/1759-7714.14747. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Peacher D, Campos JH. Is there a role for continuous positive airway pressure application during one-lung ventilation for video-assisted thoracoscopic surgery in the supine position? J Cardiothorac Vasc Anesth. 2020;34:2937–2939. doi: 10.1053/j.jvca.2020.06.034. [DOI] [PubMed] [Google Scholar]
- 3.Yoon S, Kim BR, Min SH, Lee J, Bahk JH, Seo JH. Repeated intermittent hypoxic stimuli to operative lung reduce hypoxemia during subsequent one-lung ventilation for thoracoscopic surgery: a randomized controlled trial. PLoS One. 2021;16:e0249880. doi: 10.1371/journal.pone.0249880. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Xin J, Fan XJ. Effect of visual endotracheal tube combined with bronchial occluder on pulmonary ventilation and arterial blood gas in patients undergoing thoracic surgery. Front Surg. 2023;9:1040224. doi: 10.3389/fsurg.2022.1040224. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Borkowf C, Johnson L, Albert P. Power and sample size calculations. 2012. pp. 271–283. [Google Scholar]
- 6.Zieliński M. Definitions and standard indications of minimally-invasive techniques in thymic surgery. J Vis Surg. 2017;3:99. doi: 10.21037/jovs.2017.06.04. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Yang YN, Tian XL, Ma FQ, Ma Q, Ma HJ, Chen XX. Effect of different doses of rocuronium on monitoring of recurrent laryngeal nerve during endoscopic thyroidectomy. J Clin Anesthesiol. 2024;40:597–600. [Google Scholar]
- 8.Zhi J, Yang D, Zhang YM, Wei LX, Deng XM. Clinical application of visual laryngeal masks. J Clin Anesthesiol. 2023;39:760–763. [Google Scholar]
- 9.Yoshimura T, Ueda K, Kakinuma A, Sawai J, Nakata Y. Bronchial blocker lung collapse technique: nitrous oxide for facilitating lung collapse during one-lung ventilation with a bronchial blocker. Anesth Analg. 2014;118:666–670. doi: 10.1213/ANE.0000000000000106. [DOI] [PubMed] [Google Scholar]
- 10.Moharana S, Jain D, Bhardwaj N, Gandhi K, Yaddanapudi S, Parikh B. Pressure support ventilation-pro decreases propofol consumption and improves postoperative oxygenation index compared with pressure-controlled ventilation in children undergoing ambulatory surgery: a randomized controlled trial. Can J Anaesth. 2020;67:445–451. doi: 10.1007/s12630-019-01556-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Selvi O, Azizoğlu M, Temel G, Tulgar S, Chitneni A, Çınar EN, Özer Z, Gürkan Y. Translation and validation of the turkish version of the quality of postoperative recovery score QoR-15: a multi-centred cohort study. Turk J Anaesthesiol Reanim. 2022;50:443–448. doi: 10.5152/TJAR.2022.21417. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Granell M, Petrini G, Kot P, Murcia M, Morales J, Guijarro R, de Andrés JA. Intubation with vivasight double-lumen tube versus conventional double-lumen tube in adult patients undergoing lung resection: a retrospective analysis. Ann Card Anaesth. 2022;25:279–285. doi: 10.4103/aca.aca_43_21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Li Y, Liu HQ, Zhang YS, Li J. One-lung ventilation for patients with laryngo-tracheal stenosis: a case report and literature review. Altern Ther Health Med. 2024;30:278–281. [PubMed] [Google Scholar]
- 14.Boussarsar M, Thierry G, Jaber S, Roudot-Thoraval F, Lemaire F, Brochard L. Relationship between ventilatory settings and barotrauma in the acute respiratory distress syndrome. Intensive Care Med. 2002;28:406–413. doi: 10.1007/s00134-001-1178-1. [DOI] [PubMed] [Google Scholar]
- 15.Wang RL. Comparison of clinical effect of video-assisted thoracoscopic surgery assisted by catheter or bronchial occluder. J Clin Pulm Med. 2017;22:3. [Google Scholar]
- 16.Zhang RX, Li Y, Liu XB, Lu XH, Sun HB, Wang ZF, Liu SL, Zheng Y, Liu XF, Wu XX. Is laryngeal mask airway general anesthesia feasible for minimally invasive esophagectomy? J Thorac Dis. 2018;10:E210–E213. doi: 10.21037/jtd.2018.03.102. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Fuehner T, Wiesner O, DeWall C, Dierich M, Simon AR, Hadem J, Ivanyi P, Welte T, Gottlieb J. Self-expanding metallic stent placement with laryngeal mask in lung transplant recipients. Transplant Proc. 2010;42:4595–4599. doi: 10.1016/j.transproceed.2010.10.016. [DOI] [PubMed] [Google Scholar]
- 18.Pratt T, Bromilow J. Laryngeal mask airway for airway control during percutaneous dilatational tracheostomy. Anaesth Intensive Care. 2011;39:1009–1013. doi: 10.1177/0310057X1103900605. [DOI] [PubMed] [Google Scholar]
- 19.Radhika KS, Sripriya R, Ravishankar M, Hemanth Kumar VR, Jaya V, Parthasarathy S. Assessment of suitability of i-gel and laryngeal mask airway-supreme for controlled ventilation in anesthetized paralyzed patients: a prospective randomized trial. Anesth Essays Res. 2016;10:88–93. doi: 10.4103/0259-1162.167849. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Li XL, He XB, Wan L, Liu CQ, Cui Y. Comparison of tracheal intubation with controlled ventilation and laryngeal mask airway with spontaneous ventilation for thoracoscopic bullectomy. Medicine (Baltimore) 2020;99:e19704. doi: 10.1097/MD.0000000000019704. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Huang HM, Chen RX, Zhu LM, Zhao WS, Ye XJ, Luo JW, Lu FD, Zhang L, Yang XY, Yuan Y, Cao J. Combined use of transversus abdominis plane block and laryngeal mask airway during implementing ERAS programs for patients with primary liver cancer: a randomized controlled trial. Sci Rep. 2020;10:14892. doi: 10.1038/s41598-020-71477-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Li XL, He XB, Wan L, Liu CQ, Cui Y. Comparison of tracheal intubation with controlled ventilation and laryngeal mask airway with spontaneous ventilation for thoracoscopic bullectomy. Medicine (Baltimore) 2020;99:e19704. doi: 10.1097/MD.0000000000019704. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Yan CL, Zhang YQ, Chen Y, Qv ZY, Zuo MZ. Comparison of SaCoVLM™ video laryngeal mask-guided intubation and i-gel combined with flexible bronchoscopy-guided intubation in airway management during general anesthesia: a non-inferiority study. BMC Anesthesiol. 2022;22:302. doi: 10.1186/s12871-022-01843-x. [DOI] [PMC free article] [PubMed] [Google Scholar]