

ABSTRACT
In the United States, while meningococcal vaccines are available and recommended for adolescents and young adults, coverage remains low and disparities persist. We evaluated meningococcal serogroups A, C, W, Y (MenACWY) and B (MenB) vaccine uptake, completion, and compliance using a cross-sectional analysis of National Immunization Survey-Teen (NIS-Teen) data (2015–2021) and a cohort analysis of commercial claims data (2010–2021). Regression models were used to identify factors associated with vaccine uptake. Included in the NIS-Teen MenACWY and MenB analyses were 138,952 and 177,077 patients, respectively. Included in the claims MenACWY and MenB analyses were 953,905 and 818,424 patients, respectively. In 2021, MenACWY uptake was 86.4% (95% confidence interval [CI]: 83.6–88.8%) among ≤13-year-olds (NIS-Teen) and 63.2% (62.8–63.5%) among 11–12-year-olds (claims). MenB was 33.7% (30.5–37.1%) among ≤17-year-olds (NIS-Teen), 41.6% (41.2–42.0%) among 16–18-year-olds (claims), and 15.0% (14.7–15.4%) among 19–23-year-olds (claims). The states with the lowest and highest MenB uptake by ≤17-year-olds in 2021 (NIS-Teen) were Minnesota (10.1% [3.9–23.6%]) and North Dakota (69.9% [52.1–83.2%]). Factors associated with MenACWY uptake included living in a state with a vaccine mandate, Black or Hispanic race (versus White), and well-child visit attendance. Factors associated with MenB uptake included having Medicaid (versus private insurance) and Hispanic race (versus White). The findings suggest that meningococcal vaccination coverage disparities persist across vaccines, age, geography, and race and ethnicity. Higher MenACWY (versus MenB) coverage suggests the benefit of routine recommendations. Annual well-child visits and simplified vaccination schedules could reduce vaccination access barriers.
KEYWORDS: Neisseria meningitidis; meningococcal vaccines; vaccination disparities; prevention, claims analyses; adolescent
Introduction
Invasive meningococcal disease (IMD), caused by Neisseria meningitidis, has low incidence (0.09 cases per 100,000 people in 2022), but even with appropriate treatment, 10–15% of IMD cases result in death and up to 40% of survivors may experience sequelae including hearing loss, amputations, and cognitive deficits.1–5 Since 2010, the United States (US) Advisory Committee on Immunization Practices (ACIP) routinely recommends vaccination against meningococcal serogroups A, C, W, and Y (MenACWY) for 11–12-year-olds (primary dose) and 16-year-olds (booster dose).6,7 Since 2015, the ACIP recommends vaccination against meningococcal serogroup B (MenB) for 16–23-year-olds (although 16–18-years-old is the preferred age for vaccination due to increased MenB risk at college entry) using shared clinical decision-making (SCDM) between healthcare providers (HCPs; most commonly pediatricians)8 and patients or their caregivers.6,7 The ACIP also recommends vaccination against meningococcal serogroups A, B, C, W, and Y (MenABCWY) when both MenACWY and MenB vaccines are indicated in the same visit,7 such as when a MenACWY vaccine booster dose and a dose of MenB vaccine are both indicated for a 16-year-old.
However, MenB vaccination coverage remains low compared with coverage for the MenACWY booster dose. Based on the National Immunization Survey-Teen (NIS-Teen) 2022 report, only 29.4% of 17-year-olds had received ≥1 MenB vaccination dose, versus 60.8% of 17-year-olds who had received their MenACWY booster dose.9 MenACWY vaccine uptake among younger adolescents (87.2% for 13-year-olds in 2022) was also higher than the MenACWY booster dose and MenB vaccine series.9
Prior studies have investigated potential factors associated with meningococcal vaccination, and identified barriers including limited awareness of IMD and limited understanding of why both MenACWY and MenB vaccines are needed for protection against IMD;10,11 however, population-level evaluations of real-world coverage disparities remain limited. As an example, prior research provides limited information on coverage disparities across US geographies12,13 and racial and ethnic groups. A previous US study identified the lowest MenB vaccine coverage in the South (14.6% for ≥1 dose) and the highest in the Northeast (18.3% for ≥1 dose), and reported the lowest coverage among non-Hispanic white patients (13.5% for ≥ 1 dose) and highest coverage among Hispanic patients (20.8% for ≥ 1 dose).13 Elucidating these disparities may inform targeted vaccination strategies across the US. This study used US data from the NIS-Teen survey and a commercial claims database to estimate coverage disparities for MenACWY and MenB vaccines across geographical regions and race and ethnicity in healthy adolescents and young adults.
Methods
Study design, period, population, and data sources
This retrospective, observational study used secondary data from the Centers for Disease Control and Prevention (CDC) NIS-Teen survey,14 and a claims database (OptumⓇ ClinformaticsⓇ Data Mart-Socioeconomic Status database; [CDM-SES]),15 to address the study objectives using representative and comprehensive data sources covering all 50 US states.
NIS-Teen
NIS-Teen contains survey responses and vaccination coverage information for one adolescent per household (provided by parents/guardians and vaccination providers, respectively) for both uninsured and insured 13–17-year-olds. Race and ethnicity are self-reported; ages are exact. All 13–17-year-old NIS-Teen respondents were eligible and selected for this analysis.
In the NIS-Teen analysis, a cross-sectional design was implemented using MenACWY data from 2015–2021 and MenB data from 2016–2021. The MenB analysis period differed from the MenACWY analysis period due to the introduction of the ACIP MenB vaccine recommendation in the 2016 CDC immunization schedules, which went into effect January 1, 2016.16
Claims database
The claims database captures data from patients enrolled in UnitedHealthcare commercial and Medicare Advantage insurance plans. Race and ethnicity were imputed using the claims database. The claims database contains year of birth but lacks month and day. July 1 was assigned as the missing date, which allowed a six-month margin of error.
In the claims analysis, a cohort design was implemented using MenACWY data from 2010–2021 and MenB data from 2015–2021. Both study periods ended on March 31, 2022. However, claims analyses results were reported up to the last full year of data (MenACWY analysis: 2010–2021; MenB analysis 2015–2021), allowing for coverage comparisons with NIS-Teen data. The claims analysis MenACWY study period began in 2010 to allow for more follow-up to capture both primary and booster doses.
Patients had to be 10.5-years-old by January 1, 2012 to be included in the MenACWY (11–16-years-old) cohort, 15.5–18-years-old to be in the MenB adolescent (16–18-years-old) cohort, and 18.5–23-years-old to be in the MenB young adult (19–23-years-old) cohort. Patients had to have been enrolled in their healthcare insurance plans for ≥12 months prior to their index dates. Patients who received a MenACWY vaccination before the date they turned 10.5-years-old were excluded from the MenACWY cohort. Patients at increased risk for IMD (i.e., with asplenia, complement deficiencies, sickle-cell disease, and/or HIV, and/or those using eculizumab)6 were excluded.
Study definitions
Definitions of patient demographic and clinical characteristics, including geographical regions, are included in Table S1. Full coverage metrics for each database are defined in Table S2.
NIS-Teen
For MenACWY, uptake was defined as at least one dose by ≤13-years-old; completion was defined as receipt of both a primary dose and a booster dose, and compliance as receipt of a primary dose between 11–12-years-old followed by a booster at 16–18-years-old. For MenB, uptake was defined as at least one dose by ≤17-years-old; completion was defined as receipt of the first and second vaccine dose within 12 or 15 months of each other.
Claims database
For MenACWY, uptake was defined as a first dose at 11–12-years-old; completion was defined as a second dose at 16-years-old, and compliance as receipt of at least one dose at 11–12-years-old and a second dose at 16-years-old. For MenB, uptake was defined as at least one dose at 16–18-years-old or at 19–23-years-old, and completion was defined as receipt of the first and second dose at 16–18-years-old or at 19–23-years-old, respectively.
For the claims data, specifically, index dates and follow-up periods were defined for MenACWY vaccine uptake (date patient turned 10.5-years-old; follow-up until 12-years-old or first vaccination), MenACWY vaccine completion (primary dose between 10.5–15-years-old, booster dose between 15.5–18-years-old; follow-up until 18-years-old), MenB vaccine uptake at 16–18-years-old or 19–23-years-old (latter of January 1, 2015 or when patient turns 15.5 or 18.5-years-old, respectively; follow-up until earliest date of end of enrollment, death, end of study period, or when patient turns 18 or 23-years-old, respectively). Each patient’s vaccine-specific baseline period was defined as the first 12 months preceding relevant index dates (excluding those dates).
Analyses
Analyses were age-specific (Table S2). Adjusted associations between individual (e.g., likelihood of meningococcal vaccination uptake) and contextual (e.g., healthcare expenditures) characteristics were assessed using generalized linear and Poisson regression models. Log-binomial, Poisson, and Cox regression analyses were performed using data from NIS-Teen and the claims database separately to identify key factors associated with likelihood of vaccine uptake.
NIS-Teen analysis
Pooled data from the NIS-Teen surveys were used to assess coverage metrics among 13–17-year-olds (MenACWY analysis: 2015–2021; MenB analysis: 2016–2021). Data for each calendar year were analyzed separately.
Claims analysis
Using the claims database, separate analyses were performed for MenACWY (study start January 1, 2010) and MenB (study start January 1, 2015). Schematics for the MenACWY claims analysis and the MenB claims analysis are presented in Appendix A.
Ethical considerations
This study complied with all US patient confidentiality requirements, including the 1996 Health Insurance Portability and Accountability Act (HIPAA) regulations. Approval of this study was provided by the GSK Protocol Review Committee, which reviewed the protocol (protocol identifier: VEO-000434b). All data analyzed in this study were retrospective, anonymized, public-use data; no direct subject contact or primary collection of individual human subject data occurred. Therefore, this study was considered non-human subjects research and did not require informed consent, ethics committee, or Institutional Review Board review per the 45 CFR 46 Category 4 Common Rule.17
Results
Demographic and clinical characteristics
NIS-Teen analysis
A total of 138,952 and 177,077 patients were included in the NIS-Teen MenACWY and MenB analyses, respectively. Patients were 13–17-years-old and distributed across age and gender in approximately equal proportions. Approximately half (51.3%) of patients were White, 24.4% were Hispanic, and 13.6% were Black. Overall, 10.8% of patients were of another race (defined in this study as non-Hispanic patients who were not Black or White) or multiple races.
The most common US Census divisions18 of residency were the South Atlantic (19.2%), Pacific (16.1%), East North Central (14.5%), West South Central (13.6%), and Middle Atlantic (11.9%). Most (80.3%) patients had a well-child-exam at 11–12-years-old. Half (53.3%) had private insurance and 36.1% had Medicaid. At the time of survey, 34.7% of patients had attended 2–3 HCP visits in the past 12 months; the average age at last healthcare checkup was 14.2-years-old.
Claims analysis
After applying the claims analysis exclusion criteria, a total of 10,712,496 unique patients eligible for vaccination against MenACWY and/or MenB were identified from the claims database from January 2010–March 2022. After applying the study eligibility criteria, 953,905 patients comprised the MenACWY cohort, 818,424 patients comprised the MenB 16–18-year-old cohort, and 525,487 patients comprised the MenB 19–23-year-old cohort. In each cohort, lack of continuous enrollment in a healthcare insurance plan for at least 12 months contributed to the largest number of patients excluded; 4,934,253 patients, 7,010,964 patients, and 5,499,892 patients were excluded from the MenACWY, MenB 16–18-year-old, and MenB 19–23-year-old cohorts, respectively. Across all three cohorts, there was an approximately equal balance of male and female patients; patients were White (63.4%, 64.3%, 64.4%, respectively), Hispanic (12.5%, 12.9%, 13.1%, respectively), of unknown race (10.8%, 10.1%, 10.1%, respectively), Black (7.2%, 7.5%, 7.7%, respectively), or Asian (6.1%, 5.2%, 4.7%, respectively). Across all cohorts, patients resided in the South Atlantic (20.6%, 20.4%, 20.9%, respectively), West South Central (15.9%, 15.9%, 15.4%, respectively), and East North Central (15.0%, 15.6%, 15.7%, respectively) Census divisions, among others.
Half (48.6%) of patients eligible for MenACWY resided in a state with a MenACWY vaccination mandate. Across all three cohorts, the median number of pediatrician/primary care provider (PCP) visits was 1 and close to a quarter of patients in each cohort had 2–3 office visits, respectively.
Full characteristics from both databases are described in Appendix B.
Overall vaccination coverage rates
NIS-Teen analysis
NIS-Teen national MenACWY vaccine uptake (≥1 dose by ≤13-years-old) and completion (primary dose at 11–15, second at 16–18-years-old) steadily increased over 2015–2021 (Figure 1a). In 2021, MenACWY vaccine uptake among 13–17-year-olds was 89.8% (95% confidence interval [CI], 88.7–90.8%), similar to uptake in the 13-year-old subpopulation (86.4% [95% CI, 83.6–88.8%]). The 2021 MenACWY vaccine completion rate in the ≥16-years-old subpopulation was 48.2% (95% CI, 45.7–50.7%). In 2021, MenB vaccine uptake by ≤17-years-old was 33.7% (95% CI, 30.5–37.1%; Figure 1b). MenB vaccine series completion (two doses) within 15 months in 2021 in the 17-year-old subpopulation was 14.4% (95% CI, 12.1–17.1%).
Figure 1a.
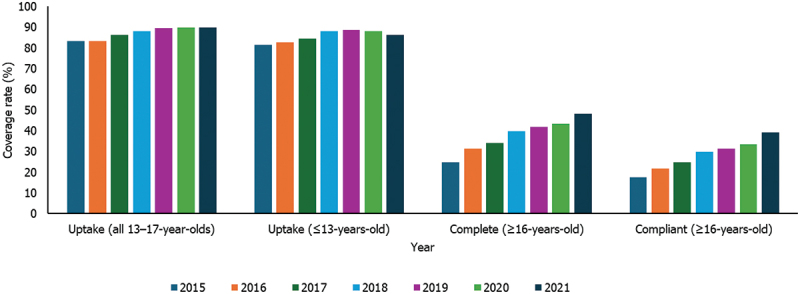
Annual crude MenACWY vaccination coverage rates among United States 13–17-year-olds; National Immunization Survey-Teen full population (2015–2021).
Figure 1b.
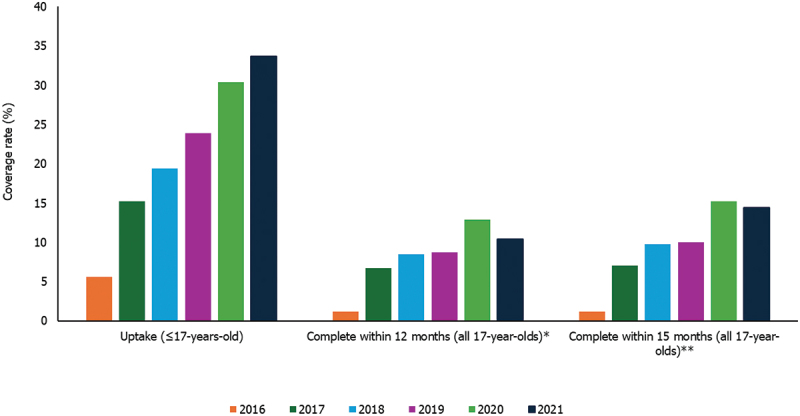
Annual crude MenB vaccination coverage rates among United States 13–17-year-olds; National Immunization Survey-Teen full population (2016–2021).
*Defined as receipt of the second dose within 12 months of the first dose. **Defined as receipt of the second dose within 15 months of the first dose.
Claims analysis
In 2021, 63.2% (95% CI, 62.8–63.5%) of patients received their MenACWY vaccine primary dose at 11–12-years-old and 65.0% (95% CI, 64.4–65.6%) received their booster dose at 16-years-old (Table S3). In 2021, 41.6% (95% CI, 41.2–42.0%) of patients in the MenB 16–18-year-old cohort received their first MenB vaccine series dose; 77.1% (95% CI, 76.8–77.5%) completed the series within 15 months. Among the MenB 19–23-year-old cohort, 15.0% (95% CI, 14.7–15.4%) received their first MenB vaccine series dose; 47.1% (95% CI, 46.1–48.0%) completed the series within 15 months (Table S4).
Coverage rates by US geography
NIS-Teen analysis
In 2021, MenACWY vaccine uptake by Census division across 13–17-year-olds ranged from 87.1% (95% CI, 81.7–91.1%) in the Pacific to 93.9% (95% CI, 92.0–95.3%) in the Middle Atlantic. Uptake of ≥ 1 MenACWY dose by ≤13-years-old ranged from 81.1% (95% CI, 74.0–86.6%) in the East South Central division to 91.0% (95% CI, 82.8–95.5%) in New England. Uptake by ≤13-years-old in this population was lowest in Alaska (58.7% [95% CI, 42.6–73.2%]) and highest in South Dakota (99.3% [95% CI, 97.2–99.9%]; Figure 2a).
Figure 2a.
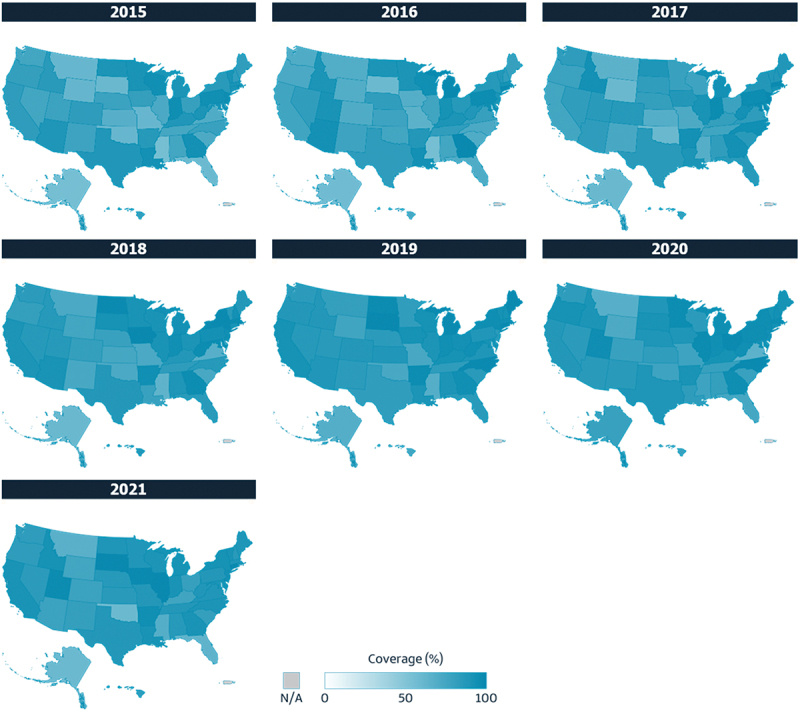
Coverage of ≥ 1 MenACWY vaccine dose by United States census state; National Immunization Survey-Teen full population (13–17-year-olds; 2015–2021).
2021 MenACWY vaccine completion rates for ≥16-year-olds ranged from 34.3% (95% CI, 28.9–40.1%) in the East South Central division to 60.8% (95% CI, 55.5–65.9%) in the Middle Atlantic. Completion was lowest in Mississippi (10.2% [95% CI, 5.8–17.4%]) and highest in North Dakota (83.4% [95% CI, 71.7–90.9%]).
In 2021, MenB vaccine uptake by ≤17-years-old ranged from 20.9% (95% CI, 15.3–27.9%) in the East South Central division to 45.2% (95% CI, 37.4–53.2%) in the South Atlantic. Minnesota and North Dakota were the lowest- and highest-performing states in 2021, respectively, ranging from 10.1% (95% CI, 3.9–23.6%) to 69.9% (95% CI, 52.1–83.2%; Figure 2b). MenB vaccine series completion within 15 months for 17-year-olds ranged from 9.8% (95% CI, 3.4–25.3%) in the Pacific to 21.9% (95% CI, 15.5–29.9%) in the South Atlantic in 2021. Series completion within 15 months was lowest in Nevada (1.4% [95% CI, 0.2–7.7%]) and highest in North Dakota (41.5% [95% CI, 25.9–59.1%]).
Figure 2b.
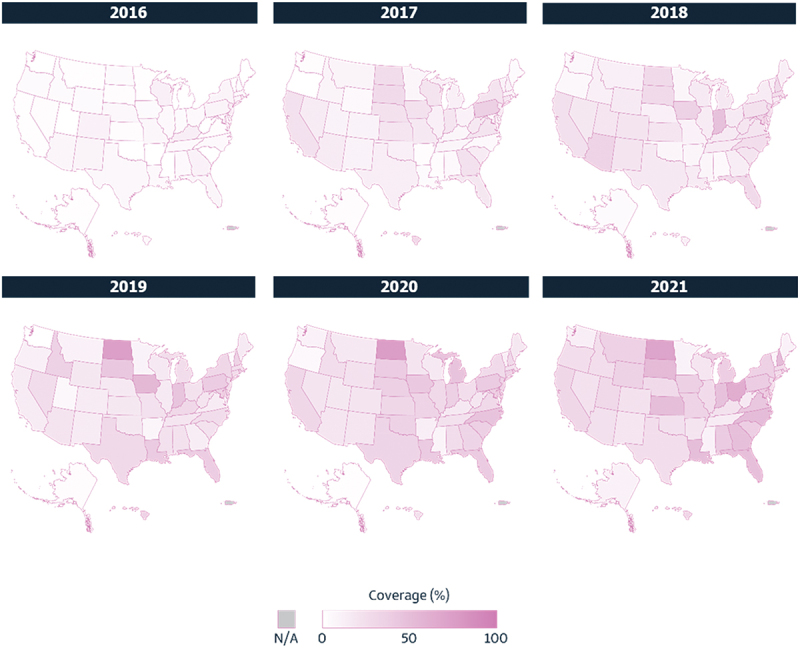
Coverage of ≥ 1 MenB vaccine dose by United States Census state; National Immunization Survey-Teen 17-year-old subpopulation (2016–2021).
Claims analysis
In 2021, among commercially-insured patients, MenACWY vaccine coverage was highest in the Middle Atlantic, where 76.1% (95% CI, 74.9–77.3%) of patients received the primary dose at 11–12-years-old and 80.1% (95% CI, 78.1–82.0%) received a booster dose by age 16. MenACWY vaccine uptake and completion was lowest in New England in 2021, where 24.9% (95% CI, 22.8–27.1%) received the primary dose at 11–12-years-old and 27.3% (95% CI, 23.5–31.3%) received a booster dose by age 16 (Table 1). In 2021, uptake was lowest in Idaho (5.7% [95% CI, 2.6–10.5%]) and highest in New Jersey (84.1% [95% CI, 82.2–85.9%]), while completion was lowest in New Mexico (6.5% [95% CI, 1.8–15.7%]) and highest in New York (84.0% [95% CI, 81.2–86.5%]).
Table 1.
MenACWY vaccine crude coverage rates by United States Census division; claims database (2021).
| N | Uptake (≥1 dose at age 11–12) | Complete (booster at age 16) | ACIP compliant (≥1 dose at age 11–12 and booster at age 16) | |
|---|---|---|---|---|
| %* (95% CI) | %* (95% CI) | %* (95% CI) | ||
| Overall | 71837 | 63.2 (62.8–63.5) | 65.0 (64.4–65.6) | 26.2 (25.7–26.6) |
| Census division | ||||
| New England | 1639 | 24.9 (22.8–27.1) | 27.3 (23.5–31.3) | 8.0 (6.4–9.8) |
| Middle Atlantic | 4755 | 76.1 (74.9–77.3) | 80.1 (78.1–82.0) | 45.5 (43.2–47.7) |
| East North Central | 10477 | 70.9 (70.0–71.8) | 71.8 (70.3–73.3) | 30.0 (28.7–31.3) |
| West North Central | 9448 | 59.8 (58.8–60.8) | 72.2 (70.8–73.6) | 25.5 (24.2–26.7) |
| South Atlantic | 14831 | 65.3 (64.5–66.1) | 66.1 (64.8–67.3) | 27.6 (26.6–28.6) |
| East South Central | 2438 | 55.9 (54.0–57.9) | 52.5 (48.6–56.4) | 18.9 (16.6–21.4) |
| West South Central | 10872 | 67.1 (66.2–67.9) | 61.7 (60.0–63.4) | 24.6 (23.4–25.9) |
| Mountain | 7914 | 65.9 (64.9–67.0) | 55.6 (53.5–57.6) | 22.8 (21.4–24.3) |
| Pacific | 7785 | 60.3 (59.2–61.4) | 57.8 (55.8–59.8) | 22.3 (21.0–23.7) |
| Unknown | 1678 | 1.5 (1.0–2.2) | 8.5 (2.8–18.7) | 0.8 (0.02–4.2) |
*Point estimate.
Abbreviations: ACIP, Advisory Committee on Immunization Practices; CI, confidence interval; MenACWY, meningococcal serogroups A, C, W, and Y.
Highest rates of receiving ≥ 1 MenB dose and completing the series within 15 months among 16–18-year-olds in 2021 were identified in the Middle Atlantic at 54.3% (95% CI, 52.6–55.9%) and 85.8% (95% CI, 84.9–86.7%), respectively (Table 2). During 2021, MenB vaccine uptake was lowest among 16–18-year-olds living in Idaho (4.2% [95% CI, 1.6–9.0%]), while completion within 15 months was lowest among 16–18-year-olds living in Alaska (20.0% [95% CI, 0.5–71.6%]). Highest uptake was found among 16–18-year-olds living in North Dakota (76.7% [95% CI, 70.9–81.9%]) and highest completion within 15 months was found in Hawaii (93.5% [95% CI, 78.6–99.2%]).
Table 2.
MenB vaccine crude coverage rates by United States census division; claims database (2021).
| MenB patients 16–18-years-old |
MenB patients 19–23-years-old |
|||||
|---|---|---|---|---|---|---|
| Uptake (≥1 dose at age 16–18) | Complete within 15 months | Uptake (≥1 dose at age 19–23) | Complete within 15 months | |||
| N | %* (95% CI) | %* (95% CI) | N | %* (95% CI) | %* (95% CI) | |
| Overall | 58034 | 41.6 (41.2–42.0) | 77.1 (76.8–77.5) | 34628 | 15.0 (14.7–15.4) | 47.1 (46.1–48.0) |
| Census division | ||||||
| New England | 1442 | 33.4 (31.0–35.9) | 85.4 (83.6–87.2) | 857 | 32.6 (29.4–35.8) | 53.7 (49.0–58.4) |
| Middle Atlantic | 3586 | 54.3 (52.6–55.9) | 85.8 (84.9–86.7) | 1788 | 29.4 (27.3–31.6) | 53.0 (49.7–56.2) |
| East North Central | 8556 | 42.5 (41.5–43.6) | 78.0 (77.2–78.9) | 5232 | 15.6 (14.6–16.6) | 52.4 (50.0–54.8) |
| West North Central | 7718 | 40.5 (39.4–41.6) | 74.7 (73.7–75.7) | 4605 | 13.5 (12.5–14.5) | 47.6 (44.9–50.3) |
| South Atlantic | 13399 | 50.7 (49.9–51.6) | 78.3 (77.7–78.9) | 7762 | 15.6 (14.8–16.4) | 45.1 (43.2–47.0) |
| East South Central | 1917 | 34.3 (32.1–36.4) | 73.0 (70.7–75.2) | 1323 | 11.5 (9.8–13.3) | 45.8 (40.1–51.7) |
| West South Central | 8477 | 38.4 (37.3–39.4) | 71.3 (70.3–72.4) | 5024 | 10.9 (10.1–11.8) | 37.4 (34.5–40.4) |
| Mountain | 6004 | 32.8 (31.6–34.0) | 70.1 (68.8–71.4) | 3589 | 11.2 (10.2–12.2) | 40.3 (37.0–43.7) |
| Pacific | 6020 | 37.9 (36.6–39.1) | 79.5 (78.4–80.5) | 3734 | 17.5 (16.3–18.8) | 50.8 (47.6–53.9) |
| Unknown | 915 | 1.7 (1.0–2.8) | 59.1 (36.4–79.3) | 714 | 0.1 (0.004–0.8) | |
*Point estimate.
Abbreviations: CI, confidence interval; MenB, meningococcal serogroup B.
Among 19–23-year-olds in 2021, patients in New England had the highest MenB vaccine uptake by 23-years-old (32.6% [95% CI, 29.4–35.8%]) and completion within 15 months (53.7% [95% CI, 49.0–58.4%]) (Table 2). In 2021, MenB vaccine uptake was lowest in New Mexico (0.7% [95% CI, 0.02–3.8%]) and highest in Massachusetts (37.7% [95% CI, 33.0–42.5%]); completion within 15 months was lowest in Idaho (20.0% [95% CI, 2.5–55.6%]) and highest in New Mexico (66.7% [95% CI, 22.3–95.7%]).
Appendix C lists full coverage rates by state per database.
Coverage rates by race and ethnicity
NIS-Teen analysis
Among 13–17-year-olds, MenACWY vaccine uptake in 2021 ranged from 87.7% (95% CI, 84.1–90.5%) in Hispanic patients to 92.4% (95% CI, 90.4–94.0%) in patients of another race or multiple races. Among 13-year-olds in 2021, uptake ranged from 85.3% (95% CI, 76.7–91.0%) in Black patients to 91.2% (95% CI, 85.6–94.8%) in patients of another race or multiple races (Figure 3a). Among patients ≥16-years-old in 2021, completion rates ranged from 44.7% (95% CI, 38.1–51.4%) in Hispanic patients to 53.4% (95% CI, 45.8–60.8%) in patients of another race or multiple races.
Figure 3a.
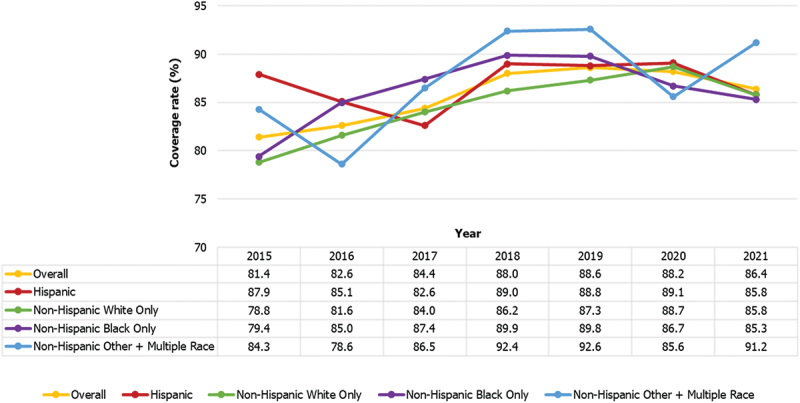
Trends in coverage of ≥1 MenACWY vaccine dose (uptake) by race and ethnicity in the United States; National Immunization Survey-Teen 13-year-old subpopulation (2015–2021).
Among 17-year-olds, MenB vaccine uptake ranged from 27.1% (95% CI, 19.5–36.3%) in patients of another race or multiple races to 42.3% (95% CI, 32.8–52.5%) in Black patients in 2021 (Figure 3b). Completion within 15 months ranged from 9.9% (95% CI, 6.1–15.8%) in patients of another and multiple races to 17.7% (95% CI, 10.9–27.4%) in Black patients (Figure 3c).
Figure 3b.
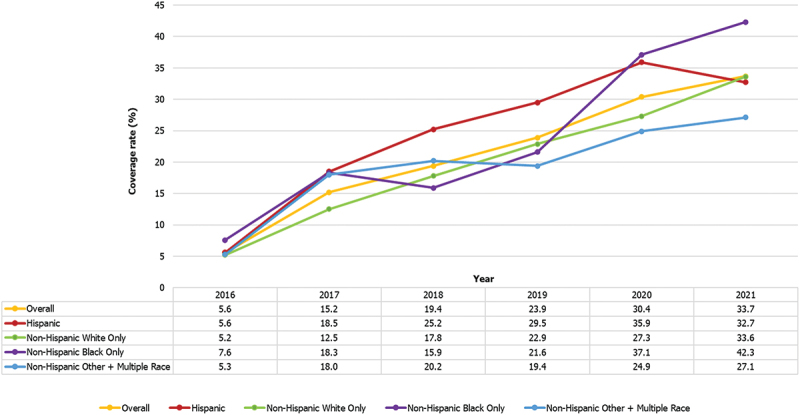
Trends in coverage of ≥ 1 MenB vaccine dose (uptake) by race and ethnicity in the United States; National Immunization Survey-Teen 17-year-old subpopulation (2016–2021).
Figure 3c.
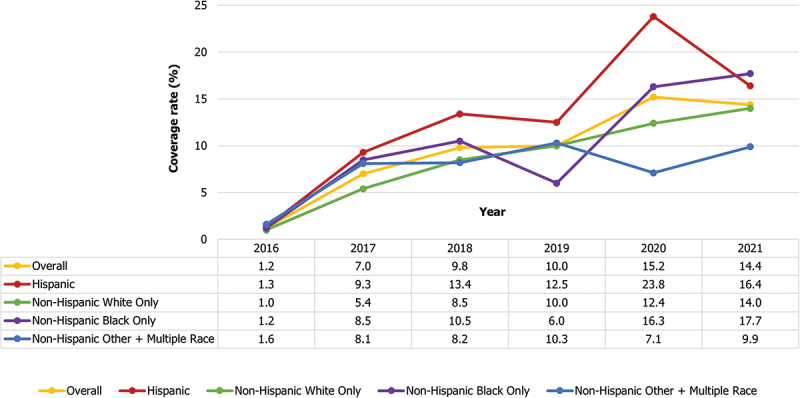
Trends in coverage of MenB vaccine series completion within 15 months by race and ethnicity in the United States; National Immunization Survey-Teen 17-year-old subpopulation (2016–2021).
Claims analysis
Among commercially-insured patients, coverage disparities across race and ethnicity were more pronounced among patients vaccinated against MenB than MenACWY (Table S5). Among 16–18-year-olds in 2021, 57.2% (95% CI, 55.9–58.6%) of patients of another race received ≥ 1 MenB vaccine dose versus 36.7% (95% CI, 35.6–37.8%) of Hispanic patients who received ≥ 1 MenB vaccine dose. Among Asian patients 16–18-years-old, 82.4% (95% CI, 81.1–83.6%) completed the MenB vaccine series within 15 months, compared to 71.5% (95% CI, 70.1–72.9%) of Black patients.
In 2021, among 19–23-year-olds of another race, 32.3% (95% CI, 30.2–34.5%) received their first MenB dose and 47.2% (95% CI, 43.2–51.2%) completed the MenB vaccine series within 15 months, versus 8.9% (95% CI, 8.1–9.7%) of Hispanic patients in this age group who received their first dose and 38.3% (95% CI, 35.1–41.6%) who completed the series within 15 months.
Predictors of vaccination uptake
Patients living in a state with a MenACWY vaccination mandate were 3.0% or 10.7% more likely to have received ≥ 1 MenACWY vaccine according to the NIS-Teen and claims analyses, respectively. Other NIS-Teen significant factors associated with increased likelihood of MenACWY uptake included residence in the East North Central Division (versus East South Central), Black or Hispanic race (versus White), and well-child visit attendance. Factors associated with increased likelihood of MenB vaccine uptake under SCDM included having Medicaid (versus private insurance), Hispanic race (versus White), and residence in the West North Central Division (versus East North Central; Appendix D).
Discussion
This retrospective study using cross-sectional NIS-Teen survey 2015–2021 data and complementary cohort claims data for the period 2010–2022 generated evidence to better understand trends in vaccination against MenACWY and MenB and the disparities in vaccination coverage among adolescents and young adults in the US. The findings of this study build upon the existing literature by providing a detailed, population-level evaluation of real-world coverage disparities.
In this study, similar proportions by gender as well as distributions by race and ethnicity and geographical region were found between the NIS-Teen analysis population and the claims analysis population. While the claims analysis was limited to private insurance, the NIS-Teen analysis found that half (53.3%) had private insurance.
In 2021, MenACWY vaccine uptake rates for ≤13-year-olds in the NIS-Teen database and claims data (at 11–12-years-old) were 86.4% and 63.2%, respectively. Lower MenB uptake rates were observed in NIS-Teen ≤17-year-olds (33.7%), the claims analysis MenB adolescent cohort (41.6%), and the claims analysis MenB young adult cohort (15.0%). These findings are consistent with the results of two US studies finding suboptimal MenB vaccine uptake and series completion rates among commercially- or Medicaid-insured young adults, perhaps due to the similar distributions of insurance coverage type across the three studies, with the majority of young adults being commercially-insured.8,19 These prior US studies reported 33% and 20% MenB vaccine series initiation among commercial- and Medicaid-insured 16–18-year-olds during 2017–2020, respectively,8 and 56.7% and 44.7% series completion in commercial- and Medicaid-insured populations, respectively.19 The consistency of these findings further highlights the need for interventions targeted toward improving MenB vaccine uptake and series completion.
Our results indicate that vaccination coverage disparities increase among age groups with less-established vaccination platforms (e.g., older adolescents).20 The meningococcal vaccination platform for 11–12-year-olds in the US is well-established and supported by the ACIP, American Academy of Pediatrics, American Academy of Family Physicians, American Medical Association, and many MenACWY vaccine state mandates, which have likely played a role in improving coverage rates in this age group.20–23 Meanwhile, there are fewer routinely recommended vaccinations for older adolescents, and these are spread over a larger age range (12–18 years old).20 Additionally, there are fewer MenACWY vaccine state requirements for colleges and universities compared with secondary school, and no current MenB vaccine state requirements.22,23 Furthermore, a recent 2023 study identified a high perceived importance of MenB vaccination as a preventative measure for the disease among parents of older adolescents and among young adults,24 highlighting a key area of opportunity for age-specific platforms. In fact, increasing the proportion of adults ≥ 19-years-old who receive recommended age-appropriate vaccines is a developmental objective of the Healthy People 2030 program,25 in line with IMD-specific goals of the American Society for Meningitis Prevention.26 Strengthening vaccination platforms that target older adolescents and young adults may improve coverage rates in these populations, reducing vaccination coverage disparities.
Vaccination disparities were also higher for MenB vaccination compared with MenACWY vaccination. Prior studies have found more prominent knowledge gaps and varying interpretations among HCPs about current ACIP guidelines for MenB vaccination under SCDM, compared with the routine MenACWY booster recommendation.11,27 A 2023 study found that strongly recommending the MenB vaccine was the top-suggested approach for improving MenB vaccination rates for 77% of HCPs (specifically physicians),11 while another 2024 study concluded that vaccination preferences of adolescents and young adults are influenced by public health authority recommendations,28 indicating that strong recommendations help facilitate increased vaccine uptake and access. This suggests the potential to improve MenB vaccination coverage among adolescents, such as via targeted education of HCPs focused on best practical implementations of vaccine recommendations utilizing HCP resources provided by the CDC, Immunize.org, and the American Society for Meningitis Prevention,29–31 or accredited continuing medical education courses.32
Our findings also demonstrate that disparities persist across geographic regions. Based on the NIS-Teen data, MenACWY vaccine uptake and completion rates were highest in states in the East North Central and Middle Atlantic Census divisions. MenACWY coverage was also found to be highest in the Middle Atlantic in the claims analysis. The majority of states in these regions hold state-wide MenACWY vaccination mandates for secondary schools and colleges,22,23 suggesting the potential benefit of vaccination mandates as a strategy to improve coverage. While MenB vaccination is recommended under SCDM, findings from both databases indicate that improved coverage is possible, as demonstrated by top-performing states such as North Dakota (~70% MenB coverage versus ~31% nationally per 2021 NIS-Teen analyses).33 Reducing barriers to meningococcal vaccination via strategies such as simplified vaccination schedules and vaccine mandates (among others warranting further investigation) may help achieve the improved coverage observed in these states.
While some differences in vaccination coverage due to race and ethnicity have decreased over time, these disparities persist among patients eligible for the MenB vaccine in particular. Among the NIS-Teen sample, patients of another race or multiple races had the lowest MenB vaccine series uptake, while Black patients had the highest MenB vaccine series uptake. This may be partially explained by the disproportionate share of Medicaid enrollees who are Black compared with other races;34 in this study, uptake was higher in patients covered by Medicaid versus private insurance. These findings highlight progress for a historically underserved population often presenting lower rates of uptake and access to other preventative care measures.35 Progress is also being made through programs such as Vaccines for Children (VFC), a CDC-funded program that covers the cost of recommended vaccines for children in the US who are Medicaid-eligible, uninsured, underinsured, and/or American Indian or Alaska Native.36 A 2014 study evaluating VFC’s effectiveness found that the program had reduced racial, ethnic, and socioeconomic disparities in child vaccination rates.37 Vaccine uptake in vulnerable and socioeconomically disadvantaged populations may be bolstered by participation in federal programs such as VFC and access to public funds that reduce financial barriers (e.g., co-payments). However, there is still a need for focused efforts toward investigating and reducing barriers to meningococcal vaccination access for patients of all racial groups.
Limitations
This study examined disparities using a sample of nationally representative individuals (representing multiple insurance types) as well as a sample limited to commercially-insured individuals. The OptumⓇ claims databases are limited to individuals under commercial and Medicare Advantage health insurance plans. Consequently, results of these studies may not be generalizable to uninsured populations or those covered by other insurance plans. Future research should investigate IMD in larger samples of patients covered by other insurance plans (e.g., Medicaid) to explore how the burden of IMD differs based on insurance type. Notably, even among individuals covered by a single insurance type, important factors contributing to vaccination disparities were identified. Another limitation of the claims database included the lack of information needed to assess the impact of specific living arrangements (e.g., dormitories), which is important for assessing the risk of IMD among older adolescents and young adults. Race and ethnicity and age were imputed. Imputation of age allowed a six-month margin of error for birthdates. However, this error was unlikely to be correlated with any outcomes or patient/geographic characteristics.
Many of the claims-related limitations were mitigated by the NIS-Teen data, which recruited patients from a nationally representative pool and contained exact age, self-reported race and ethnicity, and ages at which patients received their meningococcal vaccinations. Clinical characteristics, information on comorbidities, and patient sample age ranges are beyond the scope of data collected by NIS-Teen; vaccination coverage of 18–23-year-olds who received MenB vaccination using SCDM could not be captured. Finally, estimates by geographic region and state should be interpreted with caution given smaller sample sizes in some cases, and generally wider confidence intervals.
Conclusions
While meningococcal vaccination coverage has steadily increased in the last decade, coverage disparities persist across vaccines, age, geography, and race and ethnicity. Overall, MenB vaccine uptake and completion were lower than MenACWY vaccine uptake and completion. The lowest MenB uptake was by 19–23-year-olds in the claims analysis. In the NIS-Teen analysis, lower uptake was associated with being uninsured, residing in the New England Census region, and reporting race and ethnicity as another race or multiple races. Coverage disparities across the routinely recommended MenACWY vaccine versus the MenB vaccine (recommended under SCDM) call for interventions such as targeted education of HCPs focused on implementation of vaccine recommendations. Coverage rates in top-performing states suggest that better coverage is possible and indicate the need to reduce barriers to vaccination access through efforts including promoting annual preventive care visits and simplified vaccination schedules. Further research into vaccination disparities may help to inform strategies to improve meningococcal vaccination coverage rates among adolescents and young adults in the US.
Supplementary Material
Acknowledgments
The authors thank Costello Medical for editorial assistance and publication coordination, on behalf of GSK, and acknowledge Sarah Kyereme, Costello Medical, Boston, USA for medical writing and editorial assistance based on authors’ input and direction.
Biographies
Oscar Herrera-Restrepo is a Director in the US Health Economics & Outcomes Research division at GSK. He holds a PhD in Industrial and Systems Engineering (Management Systems) from Virginia Tech and an MSc in Industrial Engineering (Management Systems) from Universidad de Puerto Rico, Mayaguez.
Marta Kwiatkowska is a Senior Data Analyst at the NHS – DEBRA UK partnership and a former Research Associate II in the Data & Analytics division at Evidera. She holds an MSc in Health Data Analytics and Machine Learning from Imperial College London.
Samuel Huse is a Senior Data Analyst in the Data & Analytics division at Evidera. He holds a BA in Mathematics from Boston University.
Nelson Ndegwa is a Data Analyst in the Real-World Evidence division at Evidera. He was a doctoral student in Epidemiology and Biostatistics at the Karolinska Institute and holds an MSc in Bioinformatics from the University of Manchester.
Zeki Kocaata is a Global Value Evidence Lead in the Value Evidence and Outcomes division at GSK. He holds a PhD and MSc in Economics from the University of Bonn.
Michael L. Ganz is a Senior Research Scientist in the Real-World Evidence division at Evidera. He holds a PhD in Sociomedical Sciences (Health Economics) and an MS in Biostatistics from Columbia University.
Funding Statement
This work was supported by GSK (Study identifier eTrack VEO-000434b). Support for third-party writing assistance for this article, provided was funded by GSK in accordance with Good Publication Practice (GPP 2022) guidelines (https://www.ismpp.org/gpp-2022).
Disclosure statement
OHR and ZK are employed by GSK and hold financial equities in GSK. MK was an employee of Evidera (part of Thermo Fisher Scientific) at the time of this study, which was paid by GSK to conduct this study. SH and NN are employees of Evidera; MLG is an employee of Evidera and a shareholder of Thermo Fisher Scientific.
Authors’ contributions
Substantial contributions to study conception and design: OHR, MK, MLG; substantial contributions to analysis and interpretation of the data: OHR, MK, SH, NN, ZK, MLG; drafting the article or revising it critically for important intellectual content: OHR, MK, SH, NN, ZK, MLG; final approval of the version of the article to be published: OHR, MK, SH, NN, ZK, MLG.
Data sharing statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Supplementary material
Supplemental data for this article can be accessed online at https://doi.org/10.1080/21645515.2025.2479338
References
- 1.Schillie S. Revising the adolescent meningococcal vaccine schedule: term of reference and considerations. 2024. https://stacks.cdc.gov/view/cdc/148680.
- 2.Shen J, Begum N, Ruiz-Garcia Y, Martinon-Torres F, Bekkat-Berkani R, Meszaros K. Range of invasive meningococcal disease sequelae and health economic application – a systematic and clinical review. BMC Public Health. 2022;22(1):1078. doi: 10.1186/s12889-022-13342-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Harrison LH, Pelton SI, Wilder-Smith A, Holst J, Safadi MA, Vazquez JA, Taha M-K, LaForce FM, von Gottberg A, Borrow R, et al. The global meningococcal initiative: recommendations for reducing the global burden of meningococcal disease. Vaccine. 2011;29(18):3363–12. doi: 10.1016/j.vaccine.2011.02.058. [DOI] [PubMed] [Google Scholar]
- 4.Centers for Disease Control and Prevention . Meningococcal disease diagnosis, treatment, and complications. https://www.cdc.gov/meningococcal/about/diagnosis-treatment.html.
- 5.Centers for Disease Control and Prevention . Enhanced meningococcal disease surveillance report, 2022. 2022. https://www.cdc.gov/meningococcal/downloads/NCIRD-EMS-Report-2022-508.pdf.
- 6.Mbaeyi SA, Bozio CH, Duffy J, Rubin LG, Hariri S, Stephens DS, MacNeil JR. Meningococcal vaccination: recommendations of the advisory committee on immunization practices, United States, 2020. MMWR Recomm Rep. 2020;69(9):1–41. doi: 10.15585/mmwr.rr6909a1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Centers for Disease Control and Prevention . Meningococcal vaccine recommendations. https://www.cdc.gov/meningococcal/hcp/vaccine-recommendations/index.html/0.
- 8.Packnett ER, Zimmerman NM, Novy P, Morgan LC, Chime N, Ghaswalla P. Meningococcal serogroup B vaccination series initiation in the United States: a real-world claims data analysis. Hum Vaccin Immunother. 2023;19(1):2165382. doi: 10.1080/21645515.2023.2165382. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Pingali C, Yankey D, Elam-Evans LD, Markowitz LE, Valier MR, Fredua B, Crowe SJ, DeSisto CL, Stokley S, Singleton JA. Vaccination coverage among adolescents aged 13–17 years — National immunization survey–teen, United States, 2022. MMWR Morb Mortal Wkly Rep. 2023;72(34):912–919. doi: 10.15585/mmwr.mm7234a3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Ballalai I, Dawson R, Horn M, Smith V, Bekkat-Berkani R, Soumahoro L, Vicic N. Understanding barriers to vaccination against invasive meningococcal disease: a survey of the knowledge gap and potential solutions. Exper Rev Vaccines. 2023;22(1):457–467. doi: 10.1080/14760584.2023.2211163. [DOI] [PubMed] [Google Scholar]
- 11.Herrera-Restrepo O, Bunniran S, Mond T, Davenport E, Wang J, Sweeney C, Marshall GS. United States physicians’ knowledge, attitudes, and practices regarding meningococcal vaccination for healthy adolescents and young adults. J Adolesc Health. 2024;74(6):1131–1138. doi: 10.1016/j.jadohealth.2023.11.394. [DOI] [PubMed] [Google Scholar]
- 12.Ghaswalla PK, Garbinsky D, Poston S, Hunter S, Novy P, La EM. Correlates of and disparities in meningococcal B vaccination coverage among 17-year-olds in the United States: a pooled analysis of 2016-2018 National immunization survey-teen. Pediatrics. 2021;147(3):296–298. doi: 10.1542/peds.147.3MA3.296b. [DOI] [Google Scholar]
- 13.La EM, Garbinsky D, Hunter S, Poston S, Novy P, Ghaswalla P. Meningococcal B vaccination coverage among older adolescents in the United States. Vaccine. 2021;39(19):2660–2667. doi: 10.1016/j.vaccine.2021.03.071. [DOI] [PubMed] [Google Scholar]
- 14.Centers for Disease Control and Prevention . About the National Immunization Surveys (NIS). 2024. https://www.cdc.gov/nis/about/index.html.
- 15.Optum Inc . Optum claims data. https://www.optum.com/en/business/life-sciences/real-world-data/claims-data.html.
- 16.Centers for Disease Control and Prevention . Recommended immunization schedules for persons aged 0 through 18 years. 2016. https://www.cdc.gov/vaccines/hcp/imz-schedules/downloads/past/2016-child.pdf.
- 17.US Department of Health and Human Services Office for Human Research Protections . 45 CFR 46 exemptions (2018 requirements) subpart A. Basic HHS policy for protection of human research subjects HHS.Gov2018. https://www.hhs.gov/ohrp/regulations-and-policy/regulations/45-cfr-46/index.html.
- 18.US Census Bureau . Census regions and divisions of the United States. https://www2.census.gov/programs-surveys/sahie/reference-maps/2020/us_regdiv.pdf.
- 19.Packnett ER, Zimmerman NM, Kim G, Novy P, Morgan LC, Chime N, Ghaswalla P. A real-world claims data analysis of meningococcal serogroup B vaccine series completion and potential missed opportunities in the United States. Pediatr Infect Dis J. 2022;41(4):e158–e165. doi: 10.1097/INF.0000000000003455. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Kurosky SK, Esterberg E, Irwin DE, Trantham L, Packnett E, Novy P, Whelan J, Hogea C. Meningococcal vaccination among adolescents in the United States: a tale of two age platforms. J Adolesc Health. 2019;65(1):107–115. doi: 10.1016/j.jadohealth.2019.02.014. [DOI] [PubMed] [Google Scholar]
- 21.Committee on Infectious Diseases . Immunization of adolescents: recommendations of the advisory committee on immunization practices, the American Academy of pediatrics, the American Academy of family physicians, and the American Medical Association. Am Acad Pediatrics Comm Infect Dis Pediatrics. 1997;99(3):479–488. doi: 10.1542/peds.99.3.479. [DOI] [PubMed] [Google Scholar]
- 22.Immunize.org . Meningococcal ACWY (MenACWY) vaccine requirements for secondary school. https://www.immunize.org/official-guidance/state-policies/vaccine-requirements/menacwy-secondary/.
- 23.Immunize.org . Meningococcal ACWY (MenACWY) vaccine mandates for colleges and universities. https://www.immunize.org/official-guidance/state-policies/vaccine-requirements/menacwy-college/.
- 24.Herrera-Restrepo O, Zhou Z, Krishnan A, Conley WJ, Oladele E, Multani JK, Tuly R, Shi L, Chen C-C, Preiss S, et al. Awareness, attitudes, and practices on meningococcal serogroup B vaccination in the United States among parents of older adolescents and among young adults. Curr Med Res Opin. 2024;40(1):125–140. doi: 10.1080/03007995.2023.2285366. [DOI] [PubMed] [Google Scholar]
- 25.Office of Disease Prevention and Health Promotion . Increase the proportion of adults age 19 years or older who get recommended vaccines — IID‑D03. https://odphp.health.gov/healthypeople/objectives-and-data/browse-objectives/vaccination/increase-proportion-adults-age-19-years-or-older-who-get-recommended-vaccines-iid-d03.
- 26.American Society for Meningitis Prevention . How to help prevent meningococcal meningitis. 2024. https://meningitisprevention.org/get-vaccinated.
- 27.Huang L, Goren A, Lee LK, Li VW, Dempsey A, Srivastava A. Disparities in healthcare providers’ interpretations and implementations of ACIP’s meningococcal vaccine recommendations. Hum Vaccin Immunother. 2020;16(4):933–944. doi: 10.1080/21645515.2019.1682845. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Begum S, Sabater Cabrera E, Herrera-Restrepo O, Kuylen E, Shah H, Kocaata Z. Preferences for current and future meningococcal vaccines among adolescents and young adults 16–23-year-olds in the United States. Copenhagen, Denmark: European Society for Paediatric Infectious Diseases; 2024. [Google Scholar]
- 29.Centers for Disease Control and Prevention . Meningococcal vaccine recommendations. 2024. https://www.cdc.gov/meningococcal/hcp/vaccine-recommendations/index.html/1.
- 30.Immunize.org . Ask the experts: meningococcal B: vaccine recommendations. 2024. https://www.immunize.org/ask-experts/topic/menb/vaccine-recommendations-menb/.
- 31.American Society for Meningitis Prevention . Educational resources. https://meningitisprevention.org/resources.
- 32.myCME . Vaccine-based prevention of meningococcal B disease: tools for interpreting and implementing recommendations. 2021. https://www.mycme.com/courses/vaccine-based-prevention-of-meningococcal-b-disease-tools-for-interpreting-and-implementing-recommendations-7609.
- 33.Pingali C, Yankey D, Elam-Evans LD, Markowitz LE, Valier MR, Fredua B, Crowe SJ, Stokley S, Singleton JA. National vaccination coverage among adolescents aged 13–17 years — national immunization survey-teen, United States, 2021. MMWR Morb Mortal Wkly Rep. 2022;71(35):1101–1108. doi: 10.15585/mmwr.mm7135a1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Centers for Medicare and Medicaid Services . Race and ethnicity of the National Medicaid and CHIP population in 2020. https://www.medicaid.gov/media/157021.
- 35.Padamsee TJ, Bond RM, Dixon GN, Hovick SR, Na K, Nisbet EC, Wegener DT, Garrett RK. Changes in COVID-19 vaccine hesitancy among Black and White individuals in the US. JAMA Netw Open. 2022;5(1):e2144470. doi: 10.1001/jamanetworkopen.2021.44470. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Centers for Disease Control and Prevention . Vaccines for children program (VFC) information for parents. https://www.cdc.gov/vaccines-for-children/vfc-information-for-parents/index.html.
- 37.Walker AT, Smith PJ, Kolasa M. Reduction of racial/ethnic disparities in vaccination coverage, 1995-2011. MMWR Suppl. 2014;63(1):7–12. [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.