

ABSTRACT
Introduction
Chronic nausea and vomiting are symptoms of a wide range of gastrointestinal and non‐gastrointestinal conditions. Diagnosis can be challenging and requires a systematic and well‐structured approach. If the initial investigation for structural, toxic and metabolic disorders is negative, digestive motility and gut‐brain interaction disorders should be assessed. United European Gastroenterology (UEG) and the European Society for Neurogastroenterology and Motility (ESNM) identified the need for an updated, evidence‐based clinical guideline for the management of chronic nausea and vomiting.
Methods
A multidisciplinary team of experts in the field, including European specialists and national societies, participated in the development of the guideline. Relevant questions were addressed through a literature review and statements were developed and voted on according to a Delphi process.
Results
Ninety‐eight statements were identified and voted following the Delphi process. Overall agreement was high, although the grade of scientific evidence was low in many areas. Disagreement was more evident for some pharmacological treatment options. A diagnostic algorithm was developed, focussing on the differentiating features between gastrointestinal motility and gut‐brain interaction disorders with predominant nausea and vomiting.
Conclusion
These guidelines provide an evidence‐based framework for the evaluation and treatment of patients with chronic nausea and vomiting.
Keywords: Delphi, guidelines, nausea, vomiting

Abbreviations
- CBT
cognitive behavioural therapy
- CHS
cannabinoid hyperemesis syndrome
- CIPO
chronic intestinal pseudo‐obstruction
- CNVS
chronic nausea and vomiting syndrome
- CT
computed tomography
- CVS
cyclic vomiting syndrome
- EGG
electrogastrography
- EMG
electromyography
- ENS
enteric nervous system
- FLIP
functional luminal imaging probe
- GERD
gastroesophageal reflux disease
- GES
gastric electrical stimulation
- GI
gastrointestinal
- HRIM
high‐resolution manometry with impedance
- HRQOL
health‐related quality of life
- IBS
irritable bowel syndrome
- ICCs
interstitial cells of Cajal
- LOS
lower oesophageal sphincter
- MRI
magnetic resonance imaging
- N&V
nausea and vomiting
- NK‐1
neurokinin‐1
- POTS
postural orthostatic tachycardia syndrome
- PPI
proton pump inhibitors
- R1
first voting round
- R2
second voting round
- SBO
small bowel obstruction
- TCA
tricyclic antidepressant
- THC
tetrahydrocannabinol
1. Introduction
Nausea and vomiting are symptoms that commonly prompt visits to the gastrointestinal (GI) specialist and general practitioner [1, 2]. They are generally transient conditions that rapidly subside; however, in a minority of patients, persist more than 4 weeks and become a chronic disorder. The differential diagnosis of chronic nausea and vomiting is broad, and can range from organic and functional GI disorders to non‐digestive aetiologies. United European Gastroenterology (UEG) and the European Society for Neurogastroenterology and Motility (ESNM) identified the need to develop an updated, comprehensive clinical guideline on chronic nausea and vomiting, motivated by recent advances in the scientific knowledge of specific causes of nausea and vomiting such as cyclic vomiting syndrome, rumination syndrome, and chronic nausea and vomiting syndrome.
This European Guideline aims to provide a well‐structured approach to harmonizing the diagnosis and management of chronic nausea and vomiting. It has been developed through the concerted effort of gastroenterologists, surgeons and primary care physicians from the ESNM and three other member societies: EAGEN (European Association for Gastroenterology, Endoscopy and Nutrition), EDS (European Digestive Surgery) and ESCPG (European Society for Primary Care Gastroenterology).
2. Methods
The UEG/ESNM began a Delphi process to develop consensus statements on chronic nausea and vomiting in collaboration with other European societies, applying the adapted RAND/UCLA modified Delphi panel method [3, 4], which is a modification of the Delphi procedure combined with the “nominal group” technique [5, 6]. This method is based on current scientific evidence and the collective judgement of a panel of experts and aims to determine a consensus for complex conditions for which evidence from controlled trials is scarce [7]. The main steps in the process were: (1) the selection of a working group of five UEG/ESNM members with expertise in nausea and vomiting disorders and the Delphi consensus process; (2) the development of 54 clinically relevant questions for our target population, that is, gastroenterology patients and healthcare providers [8]; (3) the selection of a European Working Group consisting of experts in chronic nausea and vomiting from different European countries; (4) a literature review to answer each question and drafting of statements summarizing the evidence; (5) two rounds of blinded voting of the statements and (6) grading of strength using accepted criteria. For the working group, UEG/ESNM board members nominated experts from their respective specialist and national societies for participation: EAGEN (European Association for Gastroenterology, Endoscopy and Nutrition), EDS (European Digestive Surgery), ESCPG (European Society for Primary Care Gastroenterology), the Polish National Society, the Romanian National Society, SEPD and AEG (Spanish National GI societies), and the Croatian National Society. A total of 35 experts from 13 European countries agreed to participate (Supplementary Table S1). All members had outstanding experience and expertise in general clinical practice, gastroenterology, and GI motility. All experts submitted a conflict‐of‐interest statement by November 2022. Using the PICO process, the six members of the Core Group identified 54 clinical questions (Supplementary Table S2) that were distributed among the Working Group. Each expert carried out a structured review of the literature based on specific search terms to answer each question using MEDLINE (accessed via PubMed), EMBASE, and the Cochrane Database of Systematic Reviews (Cochrane Library) until 16 November 2022. The type of studies included were systematic reviews with/without meta‐analysis, randomized/non‐randomized clinical trials, cohort studies and observational studies. Low quality of evidence documents were excluded, such as expert opinion articles, case reports or preclinical studies. Based on the evidence in the literature, each expert formulated statements related to the assigned questions, which were then reviewed and validated by the Core Group. To assess the quality of the evidence used to formulate the statements, the grading of recommendations, assessment, development, and evaluation (GRADE) methodology was applied [9] (Supplementary Table S3). The final list of 94 statements was evaluated in a first voting round by all members in March 2023, where each member indicated their level of agreement with the statement using a 5‐point Likert scale (1: totally disagree, 2: partially disagree, 3: neither agree nor disagree, 4: partially agree, 5: totally agree). The degree of agreement for each statement was measured using the following criteria [3, 4, 5, 6]. Agreement: when more than two‐thirds of the panellists voted in the same range (either lower [1‐2] or upper range [4‐5]). Disagreement: when the median was in the lower (1–2) or upper range (4–5), but one‐third or more of the panel voted in the opposite range; or if the median was 3 but one third or more of the panel voted in the lower (1‐2) or upper range (4–5). Neutral: when the median was 3 and less than one third of the panel voted in the lower (1–2) or upper range (4–5). Statements that reached agreement were considered appropriate for clinical management when the median was in the upper range (4–5) and inappropriate when the median was in the lower range (1–2). If agreement was not reached, appropriateness was considered uncertain. Participants were blinded to the votes of other participants and made suggestions to improve the clarity of the statements. After the first round of voting, the statements and recommendations were revised by the Core Group. Nine statements were subjected to a second round of blinded voting due to lack of agreement. A Delphi analysis report was then generated. Finally, a manuscript was drafted and reviewed by the Core Group for final approval.
The manuscript is divided in three sections. The first section includes statements on the most common secondary causes of chronic nausea and vomiting that should be evaluated at the beginning of diagnostic process (Table 1). The second section comprises statements on nausea and vomiting related to oesophageal, gastric, and intestinal motility disorders, while the third is dedicated to disorders of gut‐brain interaction associated with nausea and vomiting including cyclic vomiting syndrome, cannabinoid hyperemesis syndrome, chronic nausea and vomiting syndrome, and rumination syndrome (Figure 1). These motility and gut‐brain interaction disorders often involve referral and management at specialized gastroenterological centres.
TABLE 1.
Causes of secondary chronic nausea and vomiting.
| Endocrine/metabolic | Pregnancy |
| Metabolic acidosis | |
| Uraemia | |
| Hypercalcaemia | |
| Hyperthyroidism | |
| Adrenal disorders | |
| Parathyroid disorders | |
| GI inflammation | Infectious |
| Autoimmune | |
| Mucositis | |
| Dysautonomia | Postural orthostatic tachycardia syndrome (POTS) |
| Autoimmune dysautonomia | |
| Neurological disorders (Parkinson's disease, multiple system atrophy) | |
| Pharmacological | Opioids |
| GLP‐1 agonists | |
| Dopaminergics | |
| Low‐grade GI obstruction | Radiation enteritis |
| Adhesions | |
| Intestinal strictures | |
| CNS disorders | Intracranial hypertension |
| Migraine | |
| Hydrocephalus | |
| Vestibular | Labyrinthine lesions |
| Meniere's disease | |
| Vagal nerve injury | Post‐surgical |
| Psychiatric | Anxiety |
| Depression | |
| Eating disorders | |
| Malignancy‐related | Chemotherapy |
| Radiotherapy | |
| Disease‐related complications |
Abbreviations: CNS, central nervous system; GI, gastrointestinal.
FIGURE 1.
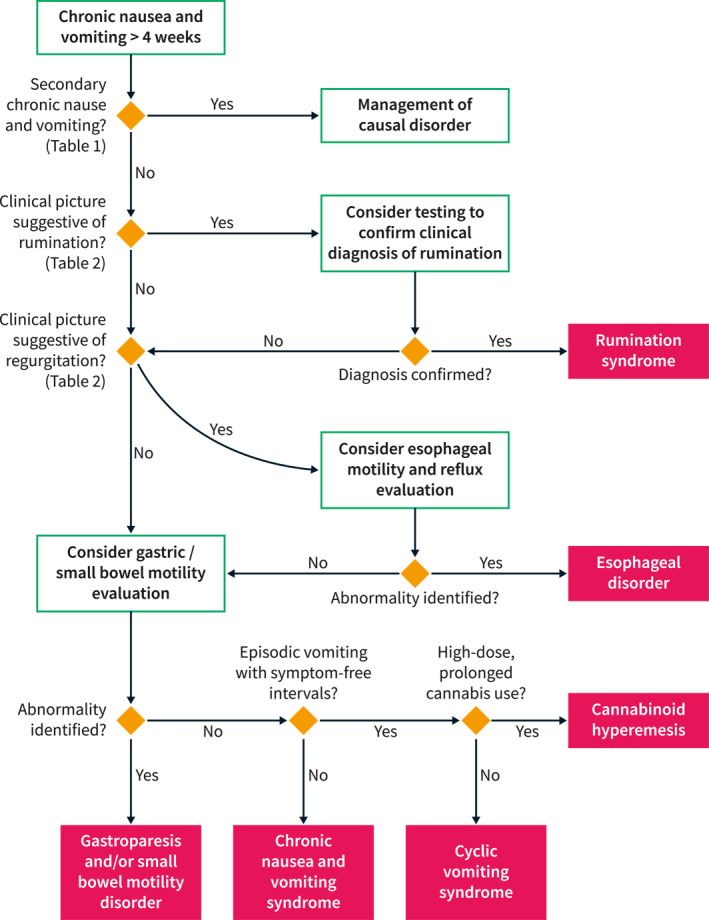
Diagnostic algorithm for chronic nausea and vomiting. Target patients are those with chronic (> 4 weeks) chronic nausea and vomiting. The consensus recommends an initial assessment of secondary forms of chronic nausea and vomiting, summarized in Table 1. If the evaluation for secondary forms is negative, a potential motility or functional digestive disorder should be considered. At this point, it is crucial to differentiate regurgitation and rumination from vomiting (Table 2). Vomiting typically involves retching, whereas regurgitation and rumination are effortless. Rumination syndrome may be diagnosed based on the characteristic features without further testing. However, confirmation, especially in less clear cases, may be obtained using oesophageal impedance manometry. If the clinical picture suggests regurgitation, objective testing for gastroesophageal reflux disease and oesophageal motility disorders is recommended. Patients with persistent unexplained nausea and vomiting, in whom rumination and regurgitation have been excluded, should be evaluated for a gastric or intestinal motility disorder. If there is no objective evidence of an underlying gastrointestinal motility disorder, the most likely diagnosis is a gut‐brain interaction disorder, either cyclic vomiting syndrome or chronic nausea and vomiting syndrome. These disorders are clinically discriminated by the vomiting pattern. When the patient presents vomiting episodes, separated by paucisymptomatic periods, the most likely diagnosis will be cyclic vomiting syndrome. If the patient with episodic vomiting is a regular cannabis user, cannabinoid hyperemesis should be considered. In patients with continuous, non‐episodic nausea and vomiting, the most likely diagnosis will be chronic nausea and vomiting syndrome.
3. Summary of Recommendations
| Level of evidence | Level of agreement* | Agreement achieved | |
|---|---|---|---|
| Section 1. Secondary chronic nausea and vomiting | |||
| Statement 1. In the evaluation of patients with chronic nausea and vomiting, endocrine and metabolic causes should be excluded. | Low | 94% | Yes |
| Statement 2. Chronic nausea and vomiting may be caused by gastrointestinal mucosal inflammation due to pharmacological toxicity, immune‐mediated disorders, or infectious diseases. | Moderate | 91% | Yes |
| Statement 3. Gastrointestinal obstruction should be excluded in patients with chronic nausea and vomiting. | Low | 85% | Yes |
| Statement 4. In patients with chronic nausea and vomiting, current medications should be reviewed to exclude pharmacological causes. | Moderate | 94% | Yes |
| Statement 5. Injuries to the vagal nerve may cause chronic nausea and vomiting following cardiac, thoracic, or abdominal interventions. | Low | 85% | Yes |
| Statement 6. Autonomic dysfunction should be considered in patients with chronic nausea and vomiting. Other symptoms that may suggest dysautonomia include orthostatic hypotension and sweating abnormalities. | Low | 79% | Yes |
| Statement 7. Vestibular disorders may be a cause of chronic nausea and vomiting. | Low | 94% | Yes |
| Statement 8. Vestibular disorders should be considered if chronic nausea and vomiting are accompanied by dizziness and/or vertigo, headache, hearing loss, tinnitus, impaired vision, focal weakness, and difficulty walking. | Low | 91% | Yes |
| Statement 9. Intracranial hypertension can cause chronic nausea and vomiting. | Low | 91% | Yes |
| Statement 10. Signs and symptoms that suggest intracranial hypertension as the cause of chronic nausea and vomiting are headache, visual disorders, vertigo, tinnitus, stiff neck, and/or focal neurologic deficits. | Low | 94% | Yes |
| Statement 11. Patients with anxiety and depression may manifest nausea and vomiting as somatic symptoms of psychological dysfunction. | Moderate | 85% | Yes |
| Statement 12. Nausea and vomiting are symptoms of eating disorders and may be self‐induced or occur as a manifestation of an associated gastrointestinal functional or motility disorder. | Moderate | 91% | Yes |
| Statement 13. In patients with advanced cancer, chronic nausea and vomiting may be caused by antineoplastic agents and radiation therapy; biochemical abnormalities; impaired gastric emptying; visceral and serosal causes of delayed gastrointestinal transit; cranial, vestibular, and cortical causes. | Very low | 91% | Yes |
| Section 2. Motility disorders | |||
| Statement 14. Chronic nausea and vomiting are not characteristic clinical features of primary oesophageal motility disorders. Regurgitation should be differentiated from vomiting. | Very low | 91% | Yes |
| Statement 15. In patients consulting for chronic nausea and vomiting, testing for oesophageal motility disorders (manometry) is recommended only if oesophageal symptoms (regurgitation, dysphagia) are present and structural disease has been ruled out. | Low | 88% | Yes |
| Statement 16. When an oesophageal motility disorder is suspected in patients with regurgitation, and/or vomiting, high‐resolution manometry should be performed after ruling out mechanical obstruction. Complementary tests, as high‐resolution impedance manometry, barium oesophagogram or endoscopic impedance planimetry FLIP may be useful in complex cases. | High | 94% | Yes |
| Statement 17. Chronic nausea and vomiting are frequent symptoms in patients with gastric motility disorders, but pain, early satiety, postprandial fullness and bloating may dominate the clinical picture in many patients. | Moderate | 85% | Yes |
| Statement 18. In patients with chronic nausea and vomiting, a gastric motility disorder may be suspected, especially when associated with diseases or medications that are associated with abnormal gastric emptying. | Moderate | 76% | Yes |
| Statement 19. A gastric emptying test is necessary to establish a diagnosis of gastroparesis in patients with unexplained chronic nausea and vomiting. | Moderate | 91% | Yes |
| Statement 20. Valid methods to measure solid gastric emptying in patients with unexplained chronic nausea and vomiting are scintigraphy and octanoic acid breath tests. | Moderate | 94% | Yes |
| Statement 21. Chronic nausea and vomiting may be characteristic clinical features of intestinal motility disorders, particularly when in presence of concomitant gastric and/or lower GI tract motility disorders. | Low | 88% | Yes |
| Statement 22. Dilated small bowel loops suggest an intestinal motor disorder in patients with chronic nausea and vomiting. | Low | 85% | Yes |
| Statement 23. Patients with confirmed intestinal motility disorders without bowel dilatation may be characterised by chronic abdominal pain. | Low | 76% | Yes |
| Statement 24. Intestinal motility tests (i.e., scintigraphy, stable isotope breath tests, wireless motility capsule, intestinal manometry, abdominal MRI) may be advised in patients with signs of intestinal dysmotility without obstructive or mucosal disorders. | Very low | 79% | Yes |
| Section 3. Disorders of gut‐brain interaction | |||
| Cyclic vomiting syndrome | |||
| Statement 25. Cyclic vomiting syndrome (CVS) refers to recurrent, regular, and stereotypical episodes of nausea and severe vomiting separated by symptom‐free intervals. CVS can be diagnosed only in the absence of other causes (organic or metabolic) that can explain the symptoms. | Moderate | 88% | Yes |
| Statement 26. CVS (defined according to Rome IV) affects about 0.1%‐2% of the adult population. | Low | 88% | Yes |
| Statement 27. Incidence and prevalence of CVS decrease with age. Accordingly, the prevalence of CVS is higher in children than in adults. Prevalence in children reaches 0.2%‐6.2% (also including studies using Rome III for definition). | Moderate | 79% | Yes |
| Statement 28. Typical characteristics suggesting CVS are the onset of episodes early in the morning, episodes lasting at least 48 h, and occurring two or fewer times per month. | Moderate | 76% | Yes |
| Statement 29. A CVS episode typically has four phases: The prodromal phase, the vomiting phase, the recovery phase, and the inter‐episodic or asymptomatic phase. | Moderate | 91% | Yes |
| Statement 30. During the prodromal phase of a CVS episode, patients often experience nausea, sweating, irritability, abdominal pain, fatigue, temperature changes, or insomnia. | Moderate | 82% | Yes |
| Statement 31. The vomiting phase of a CVS episode is characterized by intense vomiting, often bilious, and accompanied by disabling nausea and retching. Abdominal pain is often present and may be severe. Accompanying symptoms may include pallor, listlessness, anorexia, headache, photophobia, low‐grade fever, or hypothermia. | Moderate | 94% | Yes |
| Statement 32. Symptoms resolve during the recovery phase of a CVS episode. | Moderate | 88% | Yes |
| Statement 33. No vomiting is present during the inter‐episodic phase of a CVS episode, patients may be completely asymptomatic with regard to the GI system or may have milder GI symptoms. | Moderate | 91% | Yes |
| Statement 34. Symptoms can be triggered by psychological and physical stress. | Moderate | 91% | Yes |
| Statement 35. Pathogenesis of CVS is multifactorial. | High | 91% | Yes |
| Statement 36. Psychosocial factors are involved in the pathogenesis of CVS. | High | 88% | Yes |
| Statement 37. Gastric emptying is accelerated in the majority of patients with CVS, most of the other patients have normal gastric emptying. In a minority gastric emptying may be (intermittently) delayed. In these, gastroparesis is an important differential diagnosis. | Moderate | 74% | Yes |
| Statement 38. Genetic factors may be involved in CVS. | Moderate | 74% | Yes |
| Statement 39. Neurohormonal factors are involved in the pathogenesis of CVS. | Moderate | 79% | Yes |
| Statement 40. The prevalence of migraine in paediatric and adult CVS patients ranges from about 40% to 70%. About the same percentage of CVS patients have a family history of migraine. | Moderate‐low | 91% | Yes |
| Statement 41. Both, unique and potentially shared, pathophysiologic mechanisms have been observed for CVS and migraine (e.g., regarding genetic background, brain morphology, and function). Therefore, they are considered associated comorbidities but separate entities. | Moderate‐low | 88% | Yes |
| Statement 42. There is an overlap between CVS, functional dyspepsia, and irritable bowel syndrome. | Moderate‐low | 87% | Yes |
| Statement 43. Very little is known about the specific impact of CVS on adults' and children's psychosocial function. | Low | 75% | Yes |
| Statement 44. We recommend that the diagnosis of CVS is based on clinical presentation and relies on the criteria presented in statements 1 and 4‐9 of the CVS section (in analogy to Rome IV criteria). | High | 70% | Yes |
| Statement 45. We recommend that patients with CVS are treated holistically, taking into account lifestyle changes, psychological support, and avoidance of trigger factors. | Very low | 79% | Yes |
| Statement 46. Pharmacological treatment of CVS can be categorized into three groups: Abortive, supportive, and prophylactic therapy. | Moderate | 82% | Yes |
| Statement 47. We recommend that benzodiazepines and antiemetics, including ondansetron, triptans, and aprepitant are used during the prodromal phase to stop an episode of CVS and prevent vomiting. | Moderate | 91% | Yes |
| Statement 48. We recommend that during the vomiting phase energy, fluid, and electrolyte deficits are substituted intravenously. | Moderate | 82% | Yes |
| Statement 49. We recommend that antiemetics, antianxiety medications, and analgesics should be used as needed during the vomiting phase to ameliorate symptoms. | Moderate | 94% | Yes |
| Statement 50. We suggest that opioids are avoided because they may have a sensitizing effect in migraine analgesia. | Moderate | 94% | Yes |
| Statement 51. We suggest that tricyclic antidepressants are used as first‐line therapy for prophylaxis of CVS episodes. | Moderate | 85% | Yes |
| Statement 52. We suggest that as second‐line therapy for prophylaxis of CVS episodes the following substances are used: zonisamide/levetiracetam, L‐Carnitine, coenzyme Q10 and aprepitant. | Moderate | 76% | Yes |
| Statement 53. We suggest that in patients with slow recovery from CVS attacks with symptoms preventing oral food intake for several days enteral or parenteral nutrition is initiated. | Very low | 79% | Yes |
| Statement 54. Cannabinoid hyperemesis syndrome is a cyclic vomiting syndrome induced by high‐dose, prolonged cannabis use. Cannabinoid hyperemesis syndrome and cyclic vomiting syndrome are two distinct entities. | Low | 88% | Yes |
| Statement 55. We recommend that in all patients with suspected cyclic vomiting syndrome, a complete history of cannabis use is performed. | Low | 94% | Yes |
| Statement 56. Cannabinoid hyperemesis syndrome is typically characterized by severe, cyclic episodes (≥ 3/year) of nausea and vomiting with acute onset, and duration of less than a week, in patients with prolonged regular cannabis use (over 2 years). | Low | 85% | Yes |
| Statement 57. We recommend that patients with cannabinoid hyperemesis syndrome undergo withdrawal of cannabis. This is the most effective treatment. | Low | 94% | Yes |
| Statement 58. We suggest that in acute phases, patients are treated with benzodiazepines, haloperidol, and/or topical administration of capsaicin. | Low | 82% | Yes |
| Rumination syndrome | |||
| Statement 59. Rumination is a voluntary but unconscious process in which patients effortlessly bring up recently ingested food from the stomach into the mouth, where it is often then chewed again and re‐swallowed. | Moderate | 91% | Yes |
| Statement 60. The prevalence of rumination syndrome in the adult general population is likely between 0.5%‐5.8% depending on the study population. It is higher in selected populations such as therapy refractory GERD, children, and adolescents. | Moderate | 91% | Yes |
| Statement 61. Dyspeptic symptoms and minor weight loss are common in patients with rumination syndrome. | Very low | 70% | Yes |
| Statement 62. Enhanced visceral pain perception and poor postprandial accommodation of the stomach have been proposed as the mechanisms for epigastric pain and the feeling of “bloating” in patients with rumination syndrome. | Very low | 70% | Yes |
| Statement 63. The mechanism of rumination syndrome is a voluntary but unconscious process that generates a coordinated abdomino‐thoracic muscle response consisting of increased intrabdominal pressure associated to low LOS and intrathoracic pressures. | Low | 85% | Yes |
| Statement 64. The triggering of rumination events is not completely clear but they may be secondary to dyspeptic symptoms as subject seek relief through regurgitation and/or venting. | Low | 76% | Yes |
| Statement 65. Functional dyspepsia, gastroparesis, cyclic vomiting, and other disorders of gut‐brain interaction can overlap and increase the likelihood of rumination syndrome. | Low | 88% | Yes |
| Statement 66. Gastro‐oesophageal reflux disease and pathological supragastric belching can be mechanisms that provoke and/or aggravate rumination syndrome. In cases of non‐responsive gastroesophageal reflux disease, consideration should be given to rumination syndrome. | Low | 85% | Yes |
| Statement 67. Rumination syndrome is independently associated with depression and anxiety. Patients with rumination syndrome have a lower physical and mental quality of life and increased somatic symptom reporting (somatization). | Moderate | 88% | Yes |
| Statement 68. In patients with rumination syndrome, a current or previous associated eating or psychiatric disorder should be considered. | Low | 88% | Yes |
| Statement 69. Combined clinical and objective assessment using high‐resolution manometry impedance is recommended to confirm the diagnosis of rumination. | Low | 76% | Yes |
| Statement 70. Diaphragmatic breathing with or without biofeedback (visual or verbal feedback on abdominal, intercostal, or diaphragm muscle activity using either electromyography or oesophageal impedance manometry) is the first‐line therapy for rumination syndrome. | Moderate | 85% | Yes |
| Statement 71. In patients with rumination syndrome pharmacological treatment with baclofen or tricyclic antidepressants can be used if diaphragmatic breathing/biofeedback are not available or patient does not respond. | Low | 85% | Yes |
| Statement 72. In patients with secondary rumination syndrome, it is necessary to treat underlying gastroesophageal reflux with PPI. | Low | 82% | Yes |
| Statement 73. Although most patients with rumination syndrome have only modest weight loss, patient‐tailored dietetic assessment for severe cases of rumination is indicated. | Low | 85% | Yes |
| Chronic nausea and vomiting syndrome | |||
| Statement 74. Chronic unexplained nausea is defined by the presence of bothersome nausea, at least twice per week on average, in the absence of abnormalities at upper endoscopy or other disease that explains nausea, with symptoms present the last 3 months and started at least 6 months ago. | High | 88% | Yes |
| Statement 75. Chronic unexplained vomiting is diagnosed in patients who had on average at least one episode of vomiting per week, in the absence of an eating disorder, rumination, or major psychiatric disease, in absence of self‐induced induced vomiting, chronic cannabinoid use, or abnormalities in the central nervous system or metabolic diseases likely to explain the recurrent vomiting, with symptoms present the last 3 months and started at least 6 months ago. | High | 88% | Yes |
| Statement 76. Chronic nausea and vomiting syndrome, as defined according to the Rome IV criteria, has an estimated prevalence of 1%. | Low | 94% | Yes |
| Statement 77. Chronic nausea and vomiting syndrome is characterized by continuous, non‐episodic, symptoms of unexplained nausea and vomiting. | Moderate | 85% | Yes |
| Statement 78. The development and maintenance of chronic nausea and vomiting syndrome is best explained by the biopsychosocial model of disease encompassing biological, psychological, and social aspects. | Moderate | 88% | Yes |
| Statement 79. Independent factors associated with chronic nausea and vomiting syndrome are younger age, presence of IBS, and functional dyspepsia. | Moderate‐low | 91% | Yes |
| Statement 80. Psychological distress with mood disorders, anxiety disorders, somatization disorders, and catastrophizing may be associated with chronic unexplained nausea and vomiting. | Low | 91% | Yes |
| Statement 81. Chronic nausea and vomiting syndrome is diagnosed based on clinical criteria after previous exclusion of systemic, organic, or metabolic diseases by objective testing. | Low | 88% | Yes |
| Statement 82. In refractory cases of chronic nausea and vomiting syndrome, gastric electrical stimulation can be considered. | Moderate | 81% | Yes |
| Statement 83. Histamine H1 antagonists (e.g., meclizine, promethazine) are effective for the treatment of chronic nausea and vomiting. | Low | 58% | No |
| Statement 84. Muscarinic M1 antagonists (e.g., scopolamine) are effective for the treatment of chronic nausea and vomiting. | Low | 42% | No |
| Statement 85. Dopamine‐2 antagonists are effective for the treatment of chronic nausea and vomiting. | Low | 73% | Yes |
| Statement 86. 5‐HT3 antagonists are effective for the treatment of chronic nausea and vomiting. | Low | 70% | Yes |
| Statement 87. Tricyclic antidepressants are effective for the treatment of chronic nausea and vomiting. | Low | 70% | Yes |
| Statement 88. Mirtazapine is effective for the treatment of chronic nausea and vomiting. | Low | 76% | Yes |
| Statement 89. Gabapentin is effective for the treatment of chronic nausea and vomiting. | Low | 35% | No |
| Statement 90. Olanzapine is effective for the treatment of chronic nausea and vomiting. | Low | 61% | No |
| Statement 91. Cannabinoids are effective for the treatment of chronic nausea and vomiting. | Low | 29% | No |
| Statement 92. NK‐1 antagonists are effective for the treatment of chronic nausea and vomiting. | Low | 70% | Yes |
| Statement 93. In patients with chronic nausea and vomiting syndrome, attention must be given to adequate nutrition, including vitamins and minerals. | Very low | 94% | Yes |
| Statement 94. Nutritional deficits shall be corrected by dietary modifications and oral supplementation, if possible. | Very low | 91% | Yes |
*Proportion of panellists with level of agreement of 4 or 5 on the 5‐point Likert scale (1: totally disagree, 2: partially disagree, 3: neither agree nor disagree, 4: partially agree, 5: totally agree).
4. Results
4.1. Section 1. Secondary Chronic Nausea and Vomiting
4.1.1. Metabolic and Endocrine Disorders
Statement 1. In the evaluation of patients with chronic nausea and vomiting, endocrine and metabolic causes should be excluded.
Statement endorsed in R1, median panel: 5—Appropriate/agreement
Quality of evidence: low
Pregnancy is the most common endocrinologic cause of nausea and vomiting and must be considered in any woman of childbearing age. Other endocrine or metabolic aetiologies encompass diabetic ketoacidosis, uremia, hyperthyroidism, adrenal disorders, parathyroid disorders and paraneoplastic syndromes [1, 10, 11, 12]. Evaluation of endocrine/metabolic causes imply a blood test that will include thyroid assessment (TSH and T4), and other biochemical parameters: glucose, creatinine, calcium and phosphate, parathyroid hormone and blood urea nitrogen.
4.1.2. Gastrointestinal Mucosal Inflammation
Statement 2. Chronic nausea and vomiting may be caused by gastrointestinal mucosal inflammation due to pharmacological toxicity, immune‐mediated disorders, or infectious diseases.
Statement endorsed in R1, median panel: 4—Appropriate/agreement
Quality of evidence: moderate
Gastrointestinal mucosal inflammation is sometimes responsible for nausea and vomiting. Antigen presentation to the mucosa (e.g. microbial antigens) induces intestinal immune activation with low grade inflammatory changes which subsequently causes neuronal functional and structural alterations, local intestinal hypersensitivity or motor dysfunction [2]. About 9% Covid‐19 patients experience nausea or vomiting [13], sometimes in extended time. Putative direct effect of the virus on enteric nerves, inflammatory and immune activation in the intestine may cause alterations in the ENS enteroglial cells and intestinal smooth muscle [13]. Inflammation caused by the presence of the virus in the dorsal vagal complex and in the area postrema may elicit N&V [14].
Immune activation and subtle intestinal pathologies are involved in the pathogenesis of chronic N&V [15]. Many patients with gastroparesis symptoms have elevated inflammatory markers such as TNFα, IL‐6 and interstitial cells of Cajal count abnormalities [16]. N&V related to gastroparesis appears to be a multifactorial process with inflammation playing a key role in symptom development [16].
The vast majority of the literature in this area concerns the prevalence of chronic N&V in relation to mucositis caused by chemotherapy [17, 18, 19, 20], radiation therapy [17, 18, 19] and immunotherapy in oncologic patients [17]. However, it is difficult to establish a direct association of mucositis with N&V. It is a complex process potentially involving injury of the mucosa, leading to inflammatory or ulcerative lesions [17].
4.1.3. Gastrointestinal Obstruction
Statement 3. Gastrointestinal obstruction should be excluded in patients with chronic nausea and vomiting,
Statement endorsed in R1, median panel: 5—Appropriate/agreement
Quality of evidence: low
Patients with chronic N&V should be ruled out for gastrointestinal obstruction. This may be especially challenging in patients with low‐grade intestinal occlusion without proximal intestinal dilatation. Suspicion of chronic obstruction must be high in patients with inflammatory bowel disease, previous history of abdominal/pelvic surgeries, or radiation of the abdominopelvic region. In these cases, the diagnostic work‐up should be exhaustive to rule out small bowel sub‐occlusion caused by adhesions, radiation enteritis or strictures [21, 22]. In addition to chronic N&V, other clinical symptoms of obstruction include colicky abdominal pain and visible abdominal distension. Vomiting in patients with intestinal obstruction typically ceases when the patient fasts. In severe, long‐standing small bowel obstruction, vomited content may be dark and malodorous or even fecaloid [23, 24].
Objective radiological signs of obstruction such as intestinal dilatation with a visible transition point between dilated and non‐dilated bowel are not always evident, especially in patients with low‐grade chronic obstruction. It may be helpful to perform specific imaging techniques to distend the small bowel with oral contrast, such as MRI or CT enterography, to detect an intermittent or mild obstruction. However, some forms of low‐grade obstruction, particularly when caused by adhesions, are not detectable by radiology and may require an exploratory laparoscopy or laparotomy to be diagnosed. Other radiological signs that suggest intestinal obstruction include the “faeces sign” (particulate‐type material in the small bowel above the point of obstruction), the “beak sign” (a sharp narrowing of the small bowel at the point of obstruction) or anterior parietal adhesion of the small bowel in patients with intestinal adhesions [25, 26].
4.1.4. Pharmacological Agents and Toxins
Statement 4. In patients with chronic nausea and vomiting, current medications should be reviewed to exclude pharmacological causes.
Statement endorsed in R1, median panel: 5—Appropriate/agreement
Quality of evidence: moderate
Although nausea is one of the most commonly reported side effects of medications, there is a general lack of high‐quality studies investigating medication‐induced chronic N&V. Pharmacological agents produce N&V through direct and indirect mechanisms. The most important are direct stimulation of the chemoreceptor trigger zone, inhibition of gastrointestinal motility, especially delaying gastric emptying, and stimulation of the vestibular apparatus. Any given medication may have more than one mechanism associated. Common medications associated with elevated rates of chronic N&V are dopamine receptor agonists, opioids and glucagon like peptide‐1 (GLP‐1) receptor agonists.
In patients treated with dopamine receptor agonists, the mechanism of emesis seems to be centrally mediated through activation of dopaminergic D2/3 receptors [27]. Two meta‐analyses of randomized controlled trials have shown that dopamine agonists use is associated with a higher risk of N&V compared to placebo in patients with Parkinson's disease [28] and in patients with restless leg syndrome [29]. Indeed, N&V accounted for 50% of all adverse events reported with the use of ropinirole [29].
N&V are common side effects in patients that start opioid treatment, although there seems to be a tolerance phenomenon and developing chronic opioid‐induced N&V is rare [30]. Opioids have a central mechanism for inducing nausea, which is associated with delayed gastric emptying and intestinal hypomotility. Moore et al. performed a systematic review of oral opioids for chronic non‐cancer pain, which revealed that 21% of patients developed chronic nausea [31]. Laugsand et al. performed a systematic review of 50 studies evaluating the management of opioid‐induced N&V in cancer patients. Based on the analysis of the existing evidence, it has been suggested that changing the opioid type or administration route from oral to parenteral may be beneficial [32].
GLP‐1 receptor agonists are novel drugs used to treat diabetes mellitus and obesity, and their beneficial effects are mediated, at least in part, by retardation of gastric emptying [33, 34]. The main reported side effect of GLP‐1‐based agents are nausea and vomiting [35]. Bettge et al. performed a systemic analysis of gastrointestinal adverse events reported in clinical trials studying GLP‐1 receptor agonists. They found that gastrointestinal adverse effect are dose‐dependent and that long‐acting GLP‐1 receptor agonists were associated with less nausea and vomiting but more diarrhoea than short‐acting agents [36].
4.1.5. Vagal Nerve Injury
Statement 5. Injuries to the vagal nerve may cause chronic nausea and vomiting following cardiac, thoracic, or abdominal interventions.
Statement endorsed in R1, median panel: 5—Appropriate/agreement
Quality of evidence: low
A clinically relevant vagal nerve injury has been reported in patients undergoing repeated carotid endarterectomies, coronary artery bypass surgery, pneumonectomy, heart‐lung transplantation, oesophageal, gastric and bariatric surgery after fundoplication for GERD or hiatal hernia and partial gastrectomy, especially with concomitant Roux‐en‐Y anastomosis [37, 38, 39, 40, 41, 42, 43, 44, 45, 46, 47, 48, 49, 50, 51, 52, 53]. Vagal dysfunction has also been described after ablation therapy for cardiac arrhythmia [54, 55, 56, 57, 58, 59, 60].
Truncal vagotomy may result in loss of fundic and pyloric relaxation and reduced antral contractions [61]. More selective vagotomy procedures (parietal cell vagotomy or proximal gastric myotomy) may spare antral innervation and are generally associated with milder and more subtle changes in gastric function [61, 62].
Patients with vagal nerve injury after thoracic or abdominal interventions exhibit acute onset nausea, vomiting, postprandial fullness, bloating, constipation or epigastric pain, and gastric content retention [38, 43, 44, 46, 47, 48, 51, 57, 63]. The prevalence of gastric hypomotility is significantly higher in the early postoperative period and most patients recover completely with conservative treatment [44, 48, 51, 57, 63].
In thoracic surgery, symptomatic delays in gastric emptying have been reported in up to 25% of patients after single‐lung transplantation and 50% of patients after combined heart‐lung transplantation [38, 39, 40, 41, 42, 43, 44]. Gastroparesis after heart and lung transplantation may have serious implications because it predisposes to gastroesophageal reflux, microaspiration, subsequent pulmonary infection and risk of graft rejection [43, 44]. In abdominal surgery, inadvertent vagotomy has been estimated to occur in about 3%–5% of open surgeries. Specifically, the reported prevalence of unintended vagal nerve injury after anti‐reflux surgery ranges from 10% to 42% and may be more frequent with laparoscopic anti‐reflux surgery [45, 46, 47, 48, 49, 50, 51, 52].
4.1.6. Dysautonomia
Statement 6. Autonomic dysfunction should be considered in patients with chronic nausea and vomiting. Other symptoms that may suggest dysautonomia include orthostatic hypotension and sweating abnormalities.
Statement endorsed in R1, median panel: 5—Appropriate/agreement
Quality of evidence: low
GI symptoms are among the most common complaints in patients with autonomic dysfunction. Upper GI symptoms, specifically chronic N&V are among the most frequently reported. In a systemic review of gastrointestinal symptoms in patients with postural orthostatic tachycardia syndrome (POTS), Mehr S.E. et al. [64] reported a prevalence of chronic nausea between 21% and 81% and, for chronic vomiting, between 10% and 70% of patients. In patients with suspected dysautonomia diagnosed with POTS, there is evidence of abnormal gastric motility in a subgroup of patients evaluated with gastric emptying studies, either rapid gastric emptying or delayed gastric emptying [64]. Yamakawa M. et al. [65] evaluated the clinical features of 200 patients with autoimmune dysautonomia and positive ganglionic nicotinic acetylcholine receptor antibodies in Japan. In their study, chronic nausea and vomiting were common in children/adolescents and adults (60% and 21% of patients, respectively). On the other hand, there is evidence of autonomic dysfunction in patients with chronic N&V syndromes. There is an association of several autonomic features such as antecedent aura, associated headaches, photophobia, and phonophobia in patients with CVS [66]. Adrenergic autonomic dysfunction has been described in adults and children with CVS, which is similar to the autonomic dysfunction seen in patients with migraine headaches [67, 68]. GI dysmotility also plays a role in chronic nausea and vomiting in patients with dysautonomia. Nguyen et al. evaluated the autonomic function in 242 patients with chronic N&V, 72% of them had evidence of delayed gastric emptying. They found that parasympathetic dysfunction was associated with more severe symptoms and with delayed gastric empyting [69].
4.1.7. Vestibular Disorders
Statement 7. Vestibular disorders may be a cause of chronic nausea and vomiting.
Statement endorsed in R1, median panel: 5—Appropriate/agreement
Quality of evidence: low
Statement 8. Vestibular disorders should be considered if chronic nausea and vomiting are accompanied by dizziness and/or vertigo, headache, hearing loss, tinnitus, impaired vision, focal weakness, and difficulty walking.
Statement endorsed in R1, median panel: 5—Appropriate/agreement
Quality of evidence: low
N&V are common complaints in vestibular disorders, generally as an accompanying symptom of vertigo and dizziness [70, 71, 72, 73, 74, 75]. The occurrence of N&V largely depends on the type and duration of the vestibular disorder. If the vestibular disorder persists for more than 4 weeks, N&V may become chronic.
4.1.8. Intracranial Hypertension
Statement 9. Intracranial hypertension can cause chronic nausea and vomiting.
Statement endorsed in R1, median panel: 5—Appropriate/agreement
Quality of evidence: low
Statement 10. Signs and symptoms that suggest intracranial hypertension as the cause of chronic nausea and vomiting are headache, visual disorders, vertigo, tinnitus, stiff neck, and/or focal neurologic deficits.
Statement endorsed in R1, median panel: 5—Appropriate/agreement
Quality of evidence: low
Cranial hypertension can cause chronic vomiting, with or without nausea [10, 76, 77, 78, 79, 80]. Signs and symptoms that suggest cranial hypertension include non‐specific headaches, various visual abnormalities (diplopia, transient visual abnormalities, peripheral visual loss, alterations in visual acuity with blurring, loss of colour distinction, sudden visual loss), vertigo, tinnitus, stiff neck and focal neurologic deficits.
4.1.9. Psychiatric Disorders
Statement 11. Patients with anxiety and depression may manifest nausea and vomiting as somatic symptoms of psychological dysfunction.
Statement endorsed in R1, median panel: 5—Appropriate/agreement
Quality of evidence: moderate
Statement 12. Nausea and vomiting are symptoms of eating disorders and may be self‐induced or occur as a manifestation of an associated gastrointestinal functional or motility disorder.
Statement endorsed in R1, median panel: 5—Appropriate/agreement
Quality of evidence: moderate
N&V are prevalent somatic symptoms of depression and anxiety, generally in association with other somatic symptoms such as fatigue, trouble sleeping, headache and pain in arms, legs, or joints [81]. A large population study in Norway found a strong association between reporting somatic symptoms and the presence of anxiety and depression [82]. Nausea was specifically detected in 12.5% of the community and presence of anxiety disorders carried the highest risk for nausea (OR 3.42) [83].
The presence of a large number of unexplained somatic symptoms, including N&V, is associated with more severe depression and higher rates of misdiagnosis [84, 85]. A study evaluating the course of somatic symptoms of anxiety and depression, including N&V, found that these symptoms were more prevalent in females and tended to persist from childhood to adulthood [86].
GI symptoms are present in most patients with eating disorders. In a systematic literature examining the prevalence of GI symptoms in eating disorders, N&V were reported by approximately 30% of patients [87]. Therefore, eating disorders should be ruled out in patients with chronic N&V. This may be challenging, but identifying an eating disorder is imperative to correctly guide therapy [88, 89]. The aetiology of N&V in eating disorders is diverse. The main cause is self‐induced vomiting as a purgative mechanism used by patients with both bulimia nervosa and anorexia nervosa. N&V in patients with eating disorders may also be a symptom of an associated functional or motility disorder. Dyspeptic symptoms are reported by almost all patients with eating disorders [90] and delayed gastric emptying has been shown to occur in up to 40% [91, 92]. In the majority of cases, functional symptoms develop concomitantly with the eating disorder and improve with weight restoration [93].
4.1.10. Malignancy‐Related
Statement 13. In patients with advanced cancer, chronic nausea and vomiting may be caused by antineoplastic agents and radiation therapy, biochemical abnormalities, impaired gastric emptying, visceral and serosal causes of delayed gastrointestinal transit, cranial, vestibular, and cortical causes.
Statement endorsed in R1, median panel: 5—Appropriate/agreement
Quality of evidence: very low
The prevalence of N&V in patients with advanced cancer amounts to 70% [94, 95, 96, 97]. Patients may report isolated nausea, isolated vomiting (e.g., in case of increased intracranial pressure) or a combination of both symptoms [97]. Available data reflect a very complex and multifactorial nature of N&V occurring in patients with cancer [95, 96]. More than one possible aetiology is detected in around 25% of patients with malignancy [94, 97]. In general, malignancy‐related factors producing chronic N&V may be divided into those associated with cancer treatment or those associated with the disease and its complications [98, 99]. N&V secondary to antineoplastic agents and radiation therapy should be anticipated and managed according to clinical practice guidelines [100]. Other most common underlying causes of N&V in patients with cancer include chemical abnormalities (drugs, such as opioids, antidepressants, or antibiotics; toxins, derived from bowel ischemia or infection; metabolic disorders caused by renal or liver failure, hyponatremia, hypercalcemia); impaired gastric emptying (drugs, ascites, hepatomegaly, autonomic dysfunction, tumour infiltration); visceral and serosal causes of delayed gastrointestinal transit (bowel obstruction, enteritis, constipation); cranial causes (tumour or intracranial bleed, meningeal infiltration); and vestibular causes [98, 101, 102]. Given the role of anxiety and other psychological factors in patients with cancer, these causes should be also considered [95, 97]. Anticipatory N&V may occur in 25%–30% of patients by their forth chemotherapy cycle [103]. In case of N&V unrelated to antineoplastic treatment, an empirical or etiology‐based approach is recommended [95, 104].
4.2. Section 2. Motility Disorders
4.2.1. Oesophageal Motility Disorders
Statement 14. Chronic nausea and vomiting are not characteristic clinical features of primary oesophageal motility disorders. Regurgitation should be differentiated from vomiting.
Statement endorsed in R1, median panel: 5—Appropriate/agreement
Quality of evidence: very low
No specific data has been found in the literature, but based on clinical experience, nausea and vomiting are not considered as characteristic clinical features of primary oesophageal disorders such as achalasia, diffuse oesophageal spasms, or hypercontractile oesophagus, in which typical symptoms are dysphagia, regurgitation and chest pain [105]. Both patients and physicians often confuse “vomiting” and regurgitation. It is important to emphasize that an adequate clinical history should make the difference between vomiting, that is an active gastro‐duodenal process often preceded or accompanied by nausea, and regurgitation, which is passive and describes the retrograde flow of oesophageal or gastric contents into the mouth.
In patients with functional dyspepsia who often experience nausea and vomiting, nonspecific oesophageal motor disorders may be observed, mainly related to gastroesophageal reflux disease (GERD) and oesophagitis. One recent study suggests that abnormal motility of the proximal oesophagus is more often associated with symptoms of nausea and vomiting [106].
Statement 15. In patients consulting for chronic nausea and vomiting, testing for oesophageal motility disorders (manometry) is recommended only if oesophageal symptoms (regurgitation, dysphagia) are present and structural disease has been ruled out.
Statement endorsed in R1, median panel: 5—Appropriate/agreement
Quality of evidence: low
Data in the literature is scarce about the prevalence of oesophageal motility disorders in patients with nausea and vomiting. The relationship between oesophageal dysmotility and gastric disorders, such as gastroparesis and functional dyspepsia, remains unclear. In patients with functional dyspepsia who often present with nausea and vomiting as predominant symptoms, nonspecific oesophageal motor disorders may be observed, mainly related to GERD and oesophagitis [107]. We could find only one retrospective study which specifically investigated the prevalence of oesophageal motor disorders in patients with functional dyspepsia [108]. They observed a prevalence of 7%, 32% and 13% of achalasia, diffuse oesophageal spams/hypercontractile oesophagus, and esophagogastric junction outflow obstruction, respectively. Most patients had acid regurgitation and/or dysphagia though not presenting as the predominant symptom. The prevalence of achalasia and oesophageal spasms was higher in patients with delayed gastric emptying at scintigraphy. Though retrospective and probably biased, this study suggests that oesophageal motor disorder may coexist in patients with functional dyspepsia, especially when oesophageal symptoms such as acid regurgitation and dysphagia are present.
Statement 16. When an oesophageal motility disorder is suspected in patients with regurgitation, and/or vomiting, high‐resolution manometry should be performed after ruling out mechanical obstruction. Complementary tests, as high‐resolution impedance manometry, barium oesophagogram or endoscopic impedance planimetry FLIP may be useful in complex cases.
Statement endorsed in R1, median panel: 5—Appropriate/agreement
Quality of evidence: high
The analysis of suspected oesophageal motility disorder (OMD) should start with an esophagogastroduodenoscopy, to exclude benign or malignant conditions that can mimic a primary EMD. In cases with non‐conclusive endoscopic exploration and high suspicion of a structural disorder other tests like CT‐scan can be performed [109]. High‐resolution manometry (HRM) is the gold standard to assess EMD [110]. The Chicago 4.0 Classification [111] provides a classification of oesophageal motility disorders based on HRM. There are no studies evaluating the added value of high resolution impedance manometry in OMD diagnosis, only case series reporting its benefits in deciding OMD management [112], however it is recommended if rumination syndrome is suspected [113]. Chicago 4.0111 suggests that other tests can be added to the HRM to investigate OMD when equivocal results are identified using the HRM protocol or/and there is suspicion for EGJOO that do not fulfil achalasia criteria. These additional tests are timed barium esophagogram (if it is possible with a barium tablet swallow) and/or endoluminal functional lumen imaging probe (FLIP).
4.2.2. Gastric Motility Disorders
Statement 17. Chronic nausea and vomiting are frequent symptoms in patients with gastric motility disorders, but pain, early satiety, postprandial fullness and bloating may dominate the clinical picture in many patients.
Statement endorsed in R1, median panel: 4—Appropriate/agreement
Quality of evidence: moderate
The cardinal symptoms of gastric motility disorders include nausea (present in about 90%) and vomiting (present in about 75%), but patients may also complain of early satiety, postprandial fullness, bloating, belching, and upper abdominal discomfort [114, 115, 116]. Although pain was previously considered suggestive of functional dyspepsia rather than gastroparesis [117, 118], one study showed that pain occurs up to 90% of patients [115, 119, 120], and it is increasingly recognized as one of the most common symptoms of gastroparesis [121]. Evaluation of specific symptoms is complicated, since gastric motility disorders do not typically present in isolation, but may include the involvement of other organs. In diabetes, structural changes of the brain affecting the vomiting centre in the medulla, may cause nausea [122]. Pilot studies have also shown changes in brain networks in patients with gastroparesis [123, 124]. As motility disorders are not restricted to specific organs but affect several segments of the GI tract [125], symptoms may overlap between conditions. For example, many patients with gastroparesis have gastro‐oesophageal reflux, which in turn may impair oesophageal motility. In healthy subjects, in whom confounding factors such as concomitant medication and the involvement of many other organs can be controlled, the cardinal symptoms of induced gastroparesis were nausea and vomiting [126, 127, 128]. Gastrointestinal tract symptoms do, however, overlap partly due to the diffuse termination of visceral afferents in the spinal cord rendering them less specific as compared with somatic system symptoms [129, 130], and this also adds to the complexity of subjective complaints.
Statement 18. In patients with chronic nausea and vomiting, a gastric motility disorder may be suspected, especially when associated with diseases or medications that are associated with abnormal gastric emptying.
Statement endorsed in R1, median panel: 4—Appropriate/agreement
Quality of evidence: moderate
Gastric motility disorders are often associated with nausea and vomiting, but patients typically also complain of other symptoms such as early satiety, postprandial fullness, bloating and upper abdominal discomfort [114]. The clustering of such symptoms will therefore suggest a gastric motility disorder per se. Nausea and vomiting in gastroparetic patients, particularly those with diabetes, may follow a cyclical pattern, similar to cyclic vomiting syndrome [131, 132]. Suspicion that gastroparesis is the cause of nausea and vomiting should be increased in diseases associated with motility disorders, for example, diabetes and neurological disorders like Parkinson's disease. Gastroparesis should also be considered in patients with symptoms relating to previous surgery, infections, rheumatological and endocrine diseases [133]. As mentioned in statement 17, pain is frequent in patients with gastroparesis, especially in those with concomitant bowel disturbances and greater impairment in quality of life [121].
One important limitation when correlating symptoms with gastric motility is the poor association between the presence and intensity of symptoms and the degree of delayed gastric emptying [115, 134, 135]. This can be related to poor scintigraphy reporting [136], but also to the pathophysiology of gastroparesis, which encompasses several components (such as abnormal accommodation, gastric hypomotility and dysrhythmias, visceral hypersensitivity or psychological disturbances) that are not measured with standard methods such as scintigraphy [115]. However, recent data suggest that when “optimal” test methods are used, significant associations with symptoms are observed [137]. Newer techniques such as the wireless motility capsule, three‐dimensional transit or methods based on magnetic resonance imaging, where the transit time and motility of the whole GI tract are taken into consideration, may overcome these obstacles [138, 139] and offer the potential to better characterize patients with gastric motility disorders and identify their symptoms [140].
Statement 19. A gastric emptying test is necessary to establish a diagnosis of gastroparesis in patients with unexplained chronic nausea and vomiting.
Statement endorsed in R1, median panel: 5—Appropriate/agreement
Quality of evidence: moderate
Statement 20. Valid methods to measure solid gastric emptying in patients with unexplained chronic nausea and vomiting are scintigraphy and octanoic acid breath tests.
Statement endorsed in R1, median panel: 5—Appropriate/agreement
Quality of evidence: moderate
A gastric motility disorder may be considered in patients with unexplained chronic nausea and vomiting after excluding mechanical cause. The United European Gastroenterology and European Society for Neurogastroenterology and Motility consensus on gastroparesis recently acknowledged that both endoscopy and gastric emptying test were mandatory for establishing a diagnosis of gastroparesis [133]. Most studies, but not all [141, 142, 143, 144], found a correlation between nausea and vomiting severity and the delay of gastric emptying [137, 145, 146, 147, 148, 149, 150], although this correlation was weak. Most of therapeutic trials failed to demonstrate correlation between acceleration of gastric emptying and nausea and vomiting alleviation [151, 152, 153, 154]. Valid methods to measure solid gastric emptying include scintigraphy or C13 octanoic acid breath test [133, 155]. Appropriate methodology of gastric emptying studies includes an accurate 4‐h measurement and at best the absence of medications that impact on gastric motility (e.g., prokinetics or opioids) [133, 141, 155, 156]. A recent study showed that only 1/3 of patients with symptoms evocative of gastroparesis accessed to gastric emptying studies, likely due to the limited availability of tests [157]. Alternatives include wireless motility capsule test and gastric ultrasonography, but both techniques cannot be considered as first line tests. Indeed, gastric expulsion of the wireless motility capsule relies on gastric phase III activity rather than overall gastric emptying. Likewise, the main pitfall with ultrasonography is that this technique is not able to distinguish between solid and liquid emptying [133, 155]. An indirect method to assess gastric emptying relies on pressure, diameter and distensibility measurement of the pylorus using the endoFLIP system. This may represent an alternative to gastric emptying test in situations where there are no gastric emptying normal values reported (e.g., sleeve gastrectomy or esophagectomy) or in patients unable to tolerate the test meal. Pyloric pressure or distensibility alteration correlates with gastric emptying [158, 159] whereas correlation with nausea and vomiting severity remains discrepant [158, 159, 160]. EndoFLIP measurement has also been suggested to predict therapeutic response to pyloric directed therapies, including endoscopic pyloromyotomy, although this requires to be confirmed with larger trials [161, 162, 163]. Other gastric motility alterations, involving impaired fundic relaxation and/or visceral hypersensitivity poorly correlate with nausea and vomiting [164, 165, 166, 167, 168].
4.2.3. Intestinal Motility Disorders
Statement 21. Chronic nausea and vomiting may be characteristic clinical features of intestinal motility disorders, particularly when in presence of concomitant gastric and/or lower GI tract motility disorders.
Statement endorsed in R1, median panel: 4—Appropriate/agreement
Quality of evidence: low
Chronic nausea and vomiting are considered clinical features of motility disorders and, in particular, stomach and/or bowel motility disorders such as gastroparesis and chronic intestinal pseudo‐obstruction (CIPO) [169]. However, past studies evaluating the correlation between the presence of delayed gastric emptying and symptoms of nausea and/or vomiting have generally found little correlation between these symptoms and altered motility [170]. The same applies to studies evaluating small bowel motility [171].
More recent studies suggest that nausea and vomiting are less likely to correlate with the presence of a motility disturbance in a single segment of the GI tract. Nausea was reported in patients with concomitant gastroparesis and impaired small bowel motility measured by manometry in a single‐centre retrospective study [125]. A prospective single‐centre study using a wireless capsule demonstrated a moderate correlation between the presence of nausea and concomitant altered motility of the stomach, small intestine, and colon [172]. In a retrospective study conducted at a single centre, concomitant complaints of delayed colonic transit or rectal evacuation were reported in a large proportion of patients referred to a tertiary referral centre with chronic nausea and vomiting [173].
Statement 22. Dilated small bowel loops suggest an intestinal motor disorder in patients with chronic nausea and vomiting.
Statement endorsed in R1, median panel: 5—Appropriate/agreement
Quality of evidence: low
Statement 23. Patients with confirmed intestinal motility disorders without bowel dilatation may be characterised by chronic abdominal pain.
Statement endorsed in R1, median panel: 4—Appropriate/agreement
Quality of evidence: low
Very few studies have compared the clinical presentation of patients referred for suspected intestinal dysmotility with those without [174, 175]. In these studies, the number of patients with predominant nausea and/or vomiting is very small to allow a comparison [174, 175]. In the largest retrospective study in the literature, patients who underwent 24‐h small bowel manometry and were found to have normal motility had mainly unexplained abdominal pain or constipation [174]. In this study, excluding patients with previous surgery, patients presenting with symptoms/signs of sub‐occlusion were all found to have abnormal small bowel manometry [174].
In another large retrospective study, patients with chronic CIPO and severe functional disorders, mostly with abnormal small bowel manometry, were compared with IBS patients without abnormal motility. In this study, patients with CIPO were defined according to the presence of radiologically confirmed bowel dilatation compared to those with severe functional disorders. Patients with severe functional disorders presented higher epigastric pain and burning scores than those with CIPO and IBS [175]. They also had higher scores and frequency of vomiting and fullness than patients with CIPO [175]. No differences in the frequency of altered bowel habits were reported between these two groups [175].
Considering studies that only included patients with altered bowel motility, in patients diagnosed with chronic bowel dysmotility in the absence of radiological bowel dilatation, the most frequently reported symptoms were abdominal pain, abdominal distension and bloating [176, 177]. In patients with CIPO and radiologically confirmed bowel dilatation, the presence of symptoms/signs of sub‐occlusion were the main clinical presentation [178].
Statement 24. Intestinal motility tests (i.e., scintigraphy, stable isotope breath tests, wireless motility capsule, intestinal manometry, abdominal MRI) may be advised in patients with signs of intestinal dysmotility without obstructive or mucosal disorders.
Statement endorsed in R1, median panel: 4—Appropriate/agreement
Quality of evidence: very low
Plain abdominal x‐ray film has low sensitivity and specificity in detecting small bowel obstruction (SBO) [179], whereas abdominal CT scan can adequately identify patients with SBO who should be referred to surgery and determine the location of obstruction [180] with higher sensitivity than other imaging tests (i.e., plain radiography [181, 182], abdominal ultrasound [182] and small bowel follow through [183]). The current gold‐standard test to evaluate small intestinal motility is intestinal manometry. Other tests including scintigraphy and abdominal MRI are alternatives that have shown to be helpful to detect intestinal dysmotility [184, 185, 186, 187, 188, 189, 190]. Features of abnormal standard radiography and small bowel manometry may show similar findings in patients with mechanical obstruction to those with ‘functional’ obstruction (neuro‐muscular, hence CIPO) [191, 192]. Wireless capsule technology may help to evaluate small bowel dysmotility, thus aiding in recognizing possible causes of chronic nausea and vomiting [193, 194].
4.3. Section 3. Disorders of Gut‐Brain Interaction
4.3.1. Cyclic Vomiting Syndrome
4.3.1.1. Definition
Statement 25. Cyclic vomiting syndrome (CVS) refers to recurrent, regular, and stereotypical episodes of nausea and severe vomiting separated by symptom‐free intervals. CVS can be diagnosed only in the absence of other causes (organic or metabolic) that can explain the symptoms.
Statement endorsed in R1, median panel: 5—Appropriate/agreement
Quality of evidence: moderate
4.3.1.2. Epidemiology
Statement 26. CVS (defined according to Rome IV) affects about 0.1%–2% of the adult population.
Statement endorsed in R1, median panel: 5—Appropriate/agreement
Quality of evidence: low
Statement 27. Incidence and prevalence of CVS decrease with age. Accordingly, the prevalence of CVS is higher in children than in adults. Prevalence in children reaches 0.2%–6.2% (also including studies using Rome III for definition).
Statement endorsed in R1, median panel: 4—Appropriate/agreement
Quality of evidence: moderate
Cyclic vomiting syndrome (CVS) was first described in 1888 by Samuel Gee as episodes of nausea and vomiting separated by symptom‐free intervals [195, 196]. The term “cyclic” implies regularity and predictability of attacks [195, 196]. The length of symptom‐free intervals is patient specific and can last from weeks to months. Each episode can last from hours to days. CVS is a chronic entity that can persist for years [195, 196].
The syndrome was first described in children and therefore most of the criteria are based on studies and epidemiology in this population. One of the first epidemiologic studies in Aberdeen, Scotland, showed that the syndrome is not as rare as it was thought (1.9% of school‐going children) with similar prevalence in girls and boys [197, 198]. CVS is heterogeneous and the lack of definitive laboratory markers is well recognized [199]. A study in more than 200 children highlighted that, in 49% of patients diagnosed with CVS, an additional disorder can be identified that probably causes or could contribute to the vomiting [200]. For this reason, systematic diagnostic testing is recommended to look for these underlying disorders [200]; and the diagnosis of CVS is thus based upon the fulfilment of the criteria (described below) in the absence of another explanation for the symptoms [199, 201].
A larger study tried to make a distinction between cyclic nausea and chronic nausea, two frequently observed temporal patterns in children [202]. The threshold of cyclic vomiting was then defined in those patients having a high intensity (12.6 peak emeses/hour), low frequency (1.5 episodes/month) pattern, whereas the chronic group had a low intensity, high frequency, daily pattern (1.9 peak emeses/hour with 36.6 episodes/month) [203]. The cutoff of at least 4 emeses per hour and up to 2 episodes per month for the cyclic pattern was 92% sensitive and 100% specific for the final diagnosis of cyclic vomiting syndrome following negative exclusionary testing [203].
A population‐based study [204] showed an incidence of 3.15/100,000 children per year. The median age at diagnosis of CVS was 7.42 years (range 1.8–15 years). The median number of episodes of CVS per child per year was eight (range 3–52); the median duration of an episode was 24 h (range 1 h–5 days).
The Rome criteria and the task force of the international Scientific Symposium on CVS defined CVS with the following criteria [201, 205]: (1) at least 5 attacks in any interval, or a minimum of 3 attacks during a 6‐month period; (2) episodic attacks of intense nausea and vomiting lasting 1 h–10 days and occurring at least 1 week apart; (3) stereotypical pattern and symptoms in the individual patient: vomiting during attacks occurs at least 4 times/h for at least 1 h with return to baseline health between episodes; (4) Not attributed to another disorder.
However, the CVS board acknowledged the lack of evidence at the time. The criteria were defined by a combination of expert opinion, available literature, and the clinical and research experience of the task force. Some task force members recognized that atypical CVS may exist with less frequent vomiting.
CVS in adults was later recognized in 17 patients [206]. Subjects were diagnosed with CVS and considered for inclusion in the study using the following criteria: three or more discrete, stereotypic episodes of nausea and vomiting, each lasting > 12 h; > 7 days between episodes; complete resolution of nausea and vomiting between episodes; and no structural or metabolic explanation for the symptoms [206]. The results showed that an average episode of nausea and vomiting lasted 6 days (range 1–21 days), and the symptom‐free interval averaged 3.1 (0.5) months (range 0.5–6.0 months). The most uniform aspect in adult patients with CVS was the stereotypical nature of the vomiting episodes and the distinct lack of intercurrent symptoms, although it has been suggested that milder gastrointestinal symptoms may persist. In another study comparing adults and children [207], vomiting attacks occurred on average 10 times a year with a mean duration of 55.3 h in adults. In children, vomiting attacks occurred on average 25.5 times a year with a mean duration of 54.5 h [207].
4.3.2. Signs and Symptoms
Statement 28. Typical characteristics suggesting CVS are the onset of episodes early in the morning, episodes lasting at least 48 h, and occurring two or fewer times per month.
Statement endorsed in R1, median panel: 4—Appropriate/agreement
Quality of evidence: moderate
Statement 29. A CVS episode typically has four phases: the prodromal phase, the vomiting phase, the recovery phase, and the inter‐episodic or asymptomatic phase.
Statement endorsed in R1, median panel: 5—Appropriate/agreement
Quality of evidence: moderate
Statement 30. During the prodromal phase of a CVS episode, patients often experience nausea, sweating, irritability, abdominal pain, fatigue, temperature changes, or insomnia.
Statement endorsed in R1, median panel: 5—Appropriate/agreement
Quality of evidence: moderate
Statement 31. The vomiting phase of a CVS episode is characterized by intense vomiting, often bilious, and accompanied by disabling nausea and retching. Abdominal pain is often present and may be severe. Accompanying symptoms may include pallor, listlessness, anorexia, headache, photophobia, low‐grade fever, or hypothermia.
Statement endorsed in R1, median panel: 5—Appropriate/agreement
Quality of evidence: moderate
Statement 32. Symptoms resolve during the recovery phase of a CVS episode.
Statement endorsed in R1, median panel: 5—Appropriate/agreement
Quality of evidence: moderate
Statement 33. No vomiting is present during the inter‐episodic phase of a CVS episode, patients may be completely asymptomatic with regard to the GI system or may have milder GI symptoms.
Statement endorsed in R1, median panel: 5—Appropriate/agreement
Quality of evidence: moderate
Statement 34. Symptoms can be triggered by psychological and physical stress.
Statement endorsed in R1, median panel: 5—Appropriate/agreement
Quality of evidence: moderate
The duration of episodes progressively increases as infants/toddlers pass through childhood and adolescence and into adulthood [208]. The delay in diagnosis is greater in adult‐onset CVS patients than in children, and they are typically misdiagnosed for years [207, 208, 209, 210, 211]. Many other characteristics of CVS, including clinical features and response to standard therapy, are similar irrespective of age at onset, suggesting a uniform pathogenesis [208, 210]. Over time, patients usually show a gradual improvement in symptoms and complete resolution in some cases [207].
CVS typically presents in four phases: prodrome phase, vomiting phase, recovery phase and asymptomatic phase until the next episode [203, 211]. Some patients experience recognizable prodromal symptoms (e.g. nausea, sweating, irritability, abdominal pain, fatigue, temperature changes, insomnia) that provide opportunities for treatment that might provide some relief [209, 212, 213, 214]. In paediatric patients, behavioural states during episodes seem to be of three types: (1) subdued but responsive; (2) an immobile, unresponsive state referred to as “conscious coma”; and (3) writhing and moaning [212].
The vomiting is intense, accompanied by disabling nausea, and frequently bilious [201, 209]. The nausea, emesis, and retching persist even when the gastric contents consist of only mucus and bile [215]. The accompanying symptoms include pallor, listlessness, anorexia, retching, abdominal pain, headache, and photophobia, and some children have fever or diarrhoea [209, 215]. Episodes often start in the morning and are frequently triggered by psychological and physical stress, including anticipatory anxiety, infection, exercise, trauma, menstruation, and foods [206, 209, 215, 216, 217].
CVS is linked to some neurological disorders (migraine in particular) and gut‐brain interaction disorders (involving autonomic function) [197, 199, 211, 215, 216, 218]. Moreover, compared to chronic nausea and vomiting syndrome, CVS has been associated with a higher prevalence of metabolic‐endocrine disorders and genetic mitochondrial mutations and polymorphisms [215, 218, 219], the latter being more frequent in paediatric CVS compared to adult CVS [219]. In a multivariate analysis, CVS was significantly associated with comorbidities including dysautonomia, migraine, anxiety, marijuana use, irritable bowel syndrome, gastroparesis, gastroesophageal reflux disease, asthma, cigarette smoking, and hypertension [211, 220].
4.3.3. Pathophysiological Mechanisms
Statement 35. Pathogenesis of CVS is multifactorial.
Statement endorsed in R1, median panel: 5—Appropriate/agreement
Quality of evidence: high
Statement 36. Psychosocial factors are involved in the pathogenesis of CVS.
Statement endorsed in R1, median panel: 5—Appropriate/agreement
Quality of evidence: high
Statement 37. Gastric emptying is accelerated in the majority of patients with CVS, most of the other patients have normal gastric emptying. In a minority gastric emptying may be (intermittently) delayed. In these, gastroparesis is an important differential diagnosis.
Statement endorsed in R2, median panel: 4—Appropriate/agreement
Quality of evidence: moderate
Statement 38. Genetic factors may be involved in CVS.
Statement endorsed in R2, median panel: 4—Appropriate/agreement
Quality of evidence: moderate
Statement 39. Neurohormonal factors are involved in the pathogenesis of CVS.
Statement endorsed in R1, median panel: 4—Appropriate/agreement
Quality of evidence: moderate
Although several factors have been implicated in the pathogenesis of CVS, the majority of studies investigating these factors are in small series, retrospective or not replicated [221, 222, 223, 224, 225]. Psychosocial factors, such as anxiety or depression, have been reported in most patients with CVS [226]. High levels of stress have also been reported [227]. Gastric motility changes, primarily accelerated gastric emptying, have been observed [226, 228]. The presence of migraine in some patients with CVS [229] has been explained by genetical abnormalities related to mitochondrial DNA polymorphisms [219, 229]. Neurohormonal regulation has also been studied [230, 231]. Older studies identified the role of autonomic nervous dysfunction, with more frequent sympathetic abnormalities [230]. CVS patients may also have elevated levels of ghrelin and corticotrophin‐releasing factor (CRF) [231]. The gene RYR2, encoding a stress‐induced calcium channel occurring in many neurons, presents polymorphisms associated with CVS [231].
The endocannabinoid system may also play a role in CVS [232], which could explain why CVS has similar manifestations to cannabinoid hyperemesis syndrome (CHS). Furthermore, many CVS patients use cannabinoids, increasing the risk of confusion with CHS [233]. The involvement of other neurotransmitters (such as dopamine, serotonin, histamine, GABA) has not been sufficiently demonstrated [234], despite the positive effects of drugs acting on their receptors in the therapy of CVS. Other suggested factors are urea cycle disorders, hypoglycaemia, sleep disorders, or cranial hypertension. In sum, the complexity of the pathophysiology of CVS explains the comorbidities observed [218].
4.3.4. Relation With Migraine
Statement 40. The prevalence of migraine in paediatric and adult CVS patients ranges from about 40% to 70%. About the same percentage of CVS patients have a family history of migraine.
Statement endorsed in R1, median panel: 5—Appropriate/agreement
Quality of evidence: moderate‐C
Statement 41. Both, unique and potentially shared, pathophysiologic mechanisms have been observed for CVS and migraine (e.g., regarding genetic background, brain morphology, and function). Therefore, they are considered associated comorbidities but separate entities.
Statement endorsed in R1, median panel: 4—Appropriate/agreement
Quality of evidence: moderate‐C
Migraine is a frequent comorbidity in individuals with CVS, affecting both adults and children. In a systematic review by Lee et al. including both populations, 40% of patients had headaches or migraines [235]. There was a family history of headaches/migraines in 38.9%, and this association was much stronger in the adult CVS cohort compared with the paediatric cohort [235]. Li et al. reported a series of 214 children with idiopathic CVS of whom 82% had migraine‐associated CVS. This subgroup had, or subsequently developed, migraine/headaches and/or had family histories of migraine [236]. In a recent retrospective analysis of data from 57 children, 47% had a family history of migraine [237].
With respect to adults, Fleisher et al. published a retrospective analysis of 40 adult patients with CVS [213]. Of these, 28 (70%) experienced migraine headaches during or between CVS episodes. Twenty‐three (57%) of the patients had first and/or second‐degree relatives with migraine headache or its variants [213]. Partovi et al. conducted a retrospective review of patients using the clinical CVS patient registry which includes prospectively collected data of patients from 49 states in the US. Out of 455 patients with complete data, 217 (48%) also had migraine and 53% had a family history of migraine. So far, these data have been published in abstract form only [238].
The mitochondrial DNA single nucleotide polymorphisms (SNPs) 16519C_T and 3010G_A are associated with migraine and childhood cyclic vomiting syndrome [239]. Other mitochondrial DNA variants may also play a role [240]. Overall, CVS and migraine both share some form of mitochondrial dysfunction. CVS is characterized by altered insular cortex function. Migraine shows some similar alterations but also has distinct brain function characteristics [241]. Using brain MRIs, Rashid et al. demonstrated migraine‐like white matter hyperintensities in a subgroup of children with CVS and migraine, not in children with CVS who did not simultaneously suffer from migraine [242].
4.3.5. Associations
Statement 42. There is an overlap between CVS, functional dyspepsia, and irritable bowel syndrome.
Statement endorsed in R2, median panel: 4—Appropriate/agreement
Quality of evidence: moderate‐C
Patients with CVS frequently report inter‐episodic digestive symptoms. A study applying standardized Rome III questionnaires to collect GI symptoms in patients with CVS found 51% fulfiled criteria for irritable bowel syndrome and 66% for functional dyspepsia [243]. Other disorders of gut‐brain interaction, such as functional belching and functional heartburn, were also likely (39% and 38% respectively). Dyspeptic symptoms are higher in patients with migraine [213] and predict psychological distress in patients with CVS [244].
Epidemiological data from Canada, USA and UK show no difference in the prevalence of cannabis use among subjects fulfiling criteria for CVS and those with chronic nausea and vomiting syndrome, indicating an overlap between diagnoses dominated by nausea and vomiting that are included among the nausea and vomiting disorders [245].
4.3.6. Psychosocial Factors
Statement 43. Very little is known about the specific impact of CVS on adults' and children's psychosocial function.
Statement endorsed in R1, median panel: 4—Appropriate/agreement
Quality of evidence: low
There is a limited number of studies on psychosocial function/dysfunction specifically associated with CVS in adults. In a population based survey on adults, somatic symptom severity, physical and mental health‐related quality of life (HRQOL), and health care utilization was higher in the chronic nausea and vomiting disorders in general, and higher somatic symptom severity was reported to be associated specifically with CVS [245]. Almost half of CVS patients in a recent study demonstrate poor patient engagement as measured by a validated questionnaire, which was reported to be associated with poor outcomes [246]. Low patient engagement was associated with an increased number of hospitalizations and lower mental HRQOL scores.
Children with CVS reported lower HRQOL compared with those with irritable bowel syndrome (IBS), and both parents and children reported lower HRQOL compared with healthy controls [247]. This has been reported as associated with anxiety symptoms to a greater extent than the disease characteristics. Screening for anxiety symptoms and improved recognition of CVS and school support is suggested to reduce the impact of CVS on HRQOL [248].
4.3.7. Diagnosis
Statement 44. We recommend that the diagnosis of CVS is based on clinical presentation and relies on the criteria presented in statements 1 and 4‐9 of the CVS section (in analogy to Rome IV criteria).
Statement endorsed in R1, median panel: 4—Appropriate/agreement
Quality of evidence: high
The diagnosis of CVS is based on, but should not rely only on clinical presentation, at least for the first episodes of CVS. Diagnostic tests are necessary to rule out confounding conditions, assess the impact of repeating vomitus on body homeostasis, and reassure the patient or the relatives. The diagnostic work‐up is addressed to clinical presentation. Upper digestive endoscopy, small bowel X‐Ray, abdominal CT or MRI, brain imaging [249], motility studies (antroduodenal manometry, gastric emptying) [228] should be considered. In difficult cases, other rare conditions should be explored [250]. Psychological assessment should complete the work‐up [251]. In order to assess the effect of severe vomiting on the homeostasis of each patient, biochemical tests addressed to dyselectrolytemia, acid‐base balance, should be performed [250]. At present, genetic studies should be reserved for research.
4.3.8. Non‐Pharmacological Treatment Options
Statement 45. We recommend that patients with CVS are treated holistically, taking into account lifestyle changes, psychological support, and avoidance of trigger factors.
Statement endorsed in R1, median panel: 5—Appropriate/agreement
Quality of evidence: very low
Long‐term management of CVS includes education on trigger avoidance (foods such as chocolate, cheese, monosodium glutamate and red wine), regulating caffeine consumption, and fasting. Diabetes needs to be aggressively managed with a goal of blood glucose levels < 160 mg/dL [252, 253]. Episodes of hypoglycaemia must also be avoided as this may also trigger episodes. During the emetic phase, the patient's room should be kept dark, interruptions during sleep should be minimized, and the use of electronics and noise should be avoided. Moreover, avoidance of excessive emotional excitement, illness, and sleep disorders can effectively reduce the frequency of episodes in some patients. One study found that episodes of CVS fell in frequency by 70% when lifestyle changes were initiated [243]. Since chronic cannabis intake is associated with a lack of response to therapy and hyperemesis, patients should be encouraged to abstain from its use [254]. Treatment of CVS should also include strategies to address underlying psychological comorbidities, such as anxiety and depression which are common. Although data is scarce, alternative therapies such as acupressure or acupuncture could be considered for CVS prevention [254, 255].
4.3.9. Pharmacological Treatment Options
Statement 46. Pharmacological treatment of CVS can be categorized into three groups: abortive, supportive, and prophylactic therapy.
Statement endorsed in R1, median panel: 5—Appropriate/agreement
Quality of evidence: moderate
Statement 47. We recommend that benzodiazepines and antiemetics, including ondansetron, triptans, and aprepitant are used during the prodromal phase to stop an episode of CVS and prevent vomiting.
Statement endorsed in R1, median panel: 5—Appropriate/agreement
Quality of evidence: moderate
Statement 48. We recommend that during the vomiting phase energy, fluid, and electrolyte deficits are substituted intravenously.
Statement endorsed in R1, median panel: 5—Appropriate/agreement
Quality of evidence: moderate
Statement 49. We recommend that antiemetics, antianxiety medications, and analgesics should be used as needed during the vomiting phase to ameliorate symptoms.
Statement endorsed in R1, median panel: 5—Appropriate/agreement
Quality of evidence: moderate
Statement 50. We suggest that opioids are avoided because they may have a sensitizing effect in migraine analgesia.
Statement endorsed in R1, median panel: 5—Appropriate/agreement
Quality of evidence: moderate
Statement 51. We suggest that tricyclic antidepressants are used as first‐line therapy for prophylaxis of CVS episodes.
Statement endorsed in R1, median panel: 4—Appropriate/agreement
Quality of evidence: moderate
Statement 52. We suggest that as second‐line therapy for prophylaxis of CVS episodes the following substances are used: zonisamide/levetiracetam, L‐Carnitine, coenzyme Q10 and aprepitant.
Statement endorsed in R1, median panel: 4—Appropriate/agreement
Quality of evidence: moderate
Pharmacological treatment of CVS can be categorized into three groups: abortive, supportive and prophylactic therapy. The therapeutic goal of abortive (prodromal) therapy is to stop an episode of CVS and prevent vomiting. Antiemetics and benzodiazepines are routinely used. In a recent survey [256], ondansetron was the most prescribed medication during this phase. Other effective medications are triptans, for example sumatriptan, a 5‐hydroxytryptamine‐1 receptor 1B/1D agonist, as demonstrated in a study in which 83% of episodes were aborted [210]. Moreover, the NK‐1 receptor antagonist aprepitant appears to be a potent therapy (80–125 mg on the first day followed by 40–80 mg on the second and third days) [257].
During the vomiting phase, treatment consists of hydration to correct energy, fluid, and electrolyte deficits. Other rescue therapy consists of antiemetics, antianxiety medications, and analgesics. Additionally, a randomized controlled trial in a paediatric population showed that amitriptyline outperformed topiramate in reducing the severity of CVS attacks in a short‐term assessment [258].
During remission, treatment focuses on preventing further episodes. First‐line therapy for CVS prophylaxis are tricyclic antidepressants (TCAs). Amitriptyline is the preferred TCA to treat adults and is prescribed using the step‐up approach, starting with low initial doses (e.g., 10 mg at night) that are gradually increased (in some cases to 100 mg daily). At higher TCA doses (e.g. amitriptyline at 1 mg/kg/per day), 93% of patients experienced a decreased frequency and severity of attacks [226]. In addition, a randomized controlled trial conducted in Iran compared amitriptyline and cyproheptadine and revealed that both have similar positive effects on the prophylaxis of CVS [259]. Second‐line approaches include antiepileptic medications zonisamide/levetiracetam [235], L‐carnitine, and coenzyme Q10 [260, 261]. Nutritional supplements such as carnitine and coenzyme Q10 have shown some efficacy and high tolerability in small studies. The threshold for initiation of supplements should therefore be low for patients who do not achieve disease control with first‐line prophylaxis [260, 262, 263]. Aprepitant is also effective as a prophylactic treatment (40–125 mg orally twice a week) [257] (Table 3).
TABLE 3.
First‐ and second‐line pharmacological and behavioural therapeutic options for gut‐brain interaction disorders with predominant rumination/nausea/vomiting.
| 1st line | 2nd line | |
|---|---|---|
| Cyclic nausea and vomiting (prophylaxis) | Tricyclic antidepressants | Zonisamide, levetiracetam, L‐carnitine, coenzyme Q10, aprepitant |
| Cannabinoid hyperemesis | Quitting use of cannabinoids | Acute vomiting phase: Topical administration of capsaicin |
| Acute vomiting phase: Benzodiazepines, haloperidol | ||
| Rumination syndrome | Diaphragmatic breathing (+/− biofeedback) | Baclofen, tricyclic antidepressants |
| Nausea and vomiting syndrome | Tricyclic antidepressants, mirtazapine, dopamine D2 antagonists, 5‐HT3 antagonists | Gabapentin, olanzapine, NK‐1 antagonists |
4.3.10. Nutritional Support
Statement 53. We suggest that in patients with slow recovery from CVS attacks with symptoms preventing oral food intake for several days enteral or parenteral nutrition is initiated.
Statement endorsed in R1, median panel: 4—Appropriate/agreement
Quality of evidence: very low
According to expert opinion, temporary nasojejunal feedings (or exceptionally, parenteral nutrition) can hasten recovery and only should be considered if the lack of nutrition due to prolonged symptoms exceeds 5 days [264].
4.3.11. Cannabinoid Hyperemesis Syndrome
Statement 54. Cannabinoid hyperemesis syndrome is a cyclic vomiting syndrome induced by high‐dose, prolonged cannabis use. Cannabinoid hyperemesis syndrome and cyclic vomiting syndrome are two distinct entities.
Statement endorsed in R1, median panel: 5—Appropriate/agreement
Quality of evidence: low
Statement 55. We recommend that in all patients with suspected cyclic vomiting syndrome, a complete history of cannabis use is performed.
Statement endorsed in R1, median panel: 5—Appropriate/agreement
Quality of evidence: low
Statement 56. Cannabinoid hyperemesis syndrome is typically characterized by severe, cyclic episodes (≥ 3/year) of nausea and vomiting with acute onset, and duration of less than a week, in patients with prolonged regular cannabis use (over 2 years).
Statement endorsed in R1, median panel: 5—Appropriate/agreement
Quality of evidence: low
Cannabinoid hyperemesis syndrome (CHS) is cyclic vomiting secondary to prolonged high‐dose cannabis use [265, 266]. Retrospective series of patients with CHS have shown that most patients had been consuming cannabis for more than 2 years, and at high‐doses, defined as daily or nearly daily (at least 4 days a week). However, a safe threshold below which the syndrome is less likely to develop has not been defined. In 2020, 209 million individuals were using cannabis worldwide, either as a recreational drug or for treatment [267, 268]. The prevalence of CHS is unknown. One study in subjects from a drug dependent unit reported a prevalence of 18% [269].
CHS should be considered before diagnosing a patient of CVS, however differentiating these entities may be challenging since 41% of CVS patients report at least occasional cannabis use [270]. If vomiting episodes precede cannabis use, or if consumption is not high‐dose, CHS is unlikely, so CVS should be the most probable diagnosis and the aim of treatment [271]. Ultimately, the only reliable criterion to distinguish CHS from CVS is complete and persistent resolution of all symptoms of the disease following cannabis cessation [271].
The human body has two types of cannabinoid receptors, CB1 and CB2, that bind to endogenous cannabinoids [272]. CB1 receptors are in the brain, the enteric nervous system and other organs. They modulate gastric secretion, motility, inflammation, and sensation. The cannabis plant contains 3 cannabinoids: tetrahydrocannabinol (THC), cannabidiol, and cannabigerol. Exogenous cannabinoids bind to CB1 and CB2 receptors, determine psychic effects, and interestingly, some have antiemetic effects, while others at high doses cause emesis. In addition, THC accumulates in body fat and has a prolonged half‐life, leading to a large reservoir of stored THC in chronic cannabis users. These particularities might explain CHS during periods of stress [272, 273].
CHS is defined by the following characteristics: (1) severe nausea and vomiting, with a cyclic pattern (≥ 3 cycles/year), with similar onset, duration, and frequency to CVS; (2) a history of regular cannabis use for over 2 years (daily use is frequent); (3) the symptoms disappear after prolonged cannabis cessation. The third criterion is very important for the diagnosis of CHS. Patients who present ≥ 3 cycles/year, should be followed in the first year of abstinence to establish the diagnosis of CHS [266]. Similarly to CVS, CHS has 3 phases: prodromal (can last for month or years, characterized by nausea, abdominal discomfort), hyperemetic (< 1 week) and recovery phase (lasts for days‐months) [272]. Typically, patients are young (< 50 years) and use compulsive hot baths/showers to relieve symptoms, but this habit was also reported in other CVS patients. Associated symptoms are abdominal pain and weight loss [233, 274, 275, 276, 277]. Most patients start using cannabis in their teenage years, and CHS appears after prolonged, high‐dose use in the third decade of life [265]. Most patients with CHS attend the emergency department several times before diagnosis. An initial work‐up including biochemical testing, upper gastrointestinal endoscopy and CT scan are commonly performed to exclude organic causes for hyperemesis, but a complete history of cannabis use should always be performed [265].
Statement 57. We recommend that patients with cannabinoid hyperemesis syndrome undergo withdrawal of cannabis. This is the most effective treatment.
Statement endorsed in R1, median panel: 5—Appropriate/agreement
Quality of evidence: low
Statement 58. We suggest that in acute phases, patients are treated with benzodiazepines, haloperidol, and/or topical administration of capsaicin.
Statement endorsed in R1, median panel: 4—Appropriate/agreement
Quality of evidence: low
No high‐quality evidence is available on the pharmacological treatment of CHS. Several systematic reviews [265, 278] have been published on data gathered from prospective or retrospective studies, case reports and case series. Based on these reports, the only effective treatment for CHS is abstinence that achieves resolution of symptoms in 96% of cases [265]. Unfortunately, many patients are unwilling to follow this advice [270], or resume cannabis usage with the consequent relapse of CHS. It is unclear how long patients must be abstinent for their symptoms to start improving. This can vary and may take several months because of the cyclical nature of the attacks and because of the accumulation of THC in body fat.
Patients with severe dehydration and acute renal failure need fluid replacement [265]. Benzodiazepines, haloperidol [278, 279] and topical administration of capsaicin [280, 281, 282] were reported as useful in acute phases. Some reports showed that topical capsaicin decreased the total medications administered [283], while other studies did not find this association [284]. Ondansetron, the first drug used as antiemetic in the emergency department, was ineffective for CHS treatment [279]. A recent prospective observational study reported good results in patients with presumed CHS in acute phase, with intravenous ketamine and chlorpromazine [285]. Opioid analgesics should be avoided, as they can determine bowel dysfunction and emesis, and thus can worsen symptoms [265, 271]. There are limited data from case reports or small observational studies on the efficacy of prophylactic (i.e., tricyclic antidepressants, propranolol) or abortive treatments (i.e., aprepitant) in CHS [266, 278, 286, 287].
4.4. Rumination Syndrome
4.4.1. Definition
Statement 59. Rumination is a voluntary but unconscious process in which patients effortlessly bring up recently ingested food from the stomach into the mouth, where it is often then chewed again and re‐swallowed.
Statement endorsed in R1, median panel: 5—Appropriate/agreement
Quality of evidence: moderate
Rumination is characterized by an abrupt and simultaneous increase in activity of the intercostal and muscles of the anterior abdominal wall, which brings up recently ingested food. Ruminated content may be reswallowed or spat out [288]. Rumination may be accompanied by weight loss and may be easily confused with vomiting [289, 290, 291].
Rumination should be differentiated from regurgitation, as a symptom of gastroesophageal reflux and oesophageal motility disorders, which is characterized by the effortless and involuntary movement of gastric or oesophageal content to the mouth without abdominal wall contractions, not preceded by nausea, and is not accompanied by the various physical phenomena associated with vomiting [1, 288, 289] (Table 2).
TABLE 2.
Differential features of vomiting, rumination and regurgitation.
| Vomiting | Rumination | Regurgitation | ||
|---|---|---|---|---|
| General features | Source | Stomach | Stomach | Oesophagus/stomach |
| Content | Food or secretions | Food | Food or secretions | |
| Associated symptoms | Nausea | Yes | No | No |
| Retching | Yes | No | No | |
| Re‐swallowing | No | Frequent | Rare | |
| Mechanism | Relation to meals | Fasting or postprandial | Postprandial | Fasting or postprandial |
| Abdominal wall contraction | Yes, forceful | Yes, inadvertent | No | |
| Mediation | Reflex | Behavioural | Passive |
4.4.2. Epidemiology
Statement 60. The prevalence of rumination syndrome in the adult general population is likely between 0.5% and 5.8% depending on the study population. It is higher in selected populations such as therapy refractory GERD, children, and adolescents.
Statement endorsed in R1, median panel: 5—Appropriate/agreement
Quality of evidence: moderate
There are several studies among adults in the general population which have reported prevalence rates of 0.8% in Mexico [292, 293] as well as Canada [294], and 0.5%–0.9% in Australia [295, 296]. A higher prevalence rate was demonstrated in the United States of residents in Olmstead County, Minnesota, which found a 5.8% [297]. The larges study to date with 54,127 participants from 26 countries showed a prevalence of 3.1% [298]. However, studies on selected populations have reported a higher prevalence of rumination syndrome, such as patients with eating disorders (7%) or fibromyalgia (8%) [299, 300]. Several studies have also suggested that the syndrome is more common in children, adolescents (0%–7%), and patients with developmental, or psychiatric disorders [301, 302, 303, 304, 305]. The prevalence has also been suggested to be higher than the general population in patients with therapy refractory gastroesophageal reflux disease (GERD, up to 20%–46%) [306]. The prevalence of rumination syndrome also differs depending on which threshold of the frequency of rumination episodes is chosen. Patients with several episodes a day constitute a minority of the rumination syndrome population but are likely more common among patients seeking health care [298, 307].
4.4.3. Signs and Symptoms
Statement 61. Dyspeptic symptoms and minor weight loss are common in patients with rumination syndrome.
Statement endorsed in R1, median panel: 4—Appropriate/agreement
Quality of evidence: very low
Statement 62. Enhanced visceral pain perception and poor postprandial accommodation of the stomach have been proposed as the mechanisms for epigastric pain and the feeling of “bloating” in patients with rumination syndrome.
Statement endorsed in R1, median panel: 4—Appropriate/agreement
Quality of evidence: very low
Research into the association of epigastric symptoms and rumination syndrome in the medical literature is scarce. Up to 38% of patients complained of abdominal pain in a study involving children and adolescents [308].
The pathophysiology of epigastric symptoms in patients with rumination syndrome is poorly understood. Enhanced visceral pain perception and poor postprandial accommodation of the stomach have been proposed as mechanisms for epigastric pain and the feeling of “bloating” [309]. Rumination may well be an effort to reduce/relieve abdominal pain and/or bloating by “tensing the anterior abdominal wall muscles” which may then become a subconscious, maladaptive behaviour [113].
4.4.4. Pathophysiological Mechanisms
Statement 63. The mechanism of rumination syndrome is a voluntary but unconscious process that generates a coordinated abdomino‐thoracic muscle response consisting of increased intrabdominal pressure associated to low LOS and intrathoracic pressures.
Statement endorsed in R1, median panel: 5—Appropriate/agreement
Quality of evidence: low
Statement 64. The triggering of rumination events is not completely clear but they may be secondary to dyspeptic symptoms as subject seek relief through regurgitation and/or venting.
Statement endorsed in R1, median panel: 4—Appropriate/agreement
Quality of evidence: low
The proposed mechanism of rumination syndrome is an increase in intra‐abdominal pressure, due to straining of the abdominal wall muscles, usually not intentionally, and simultaneous expansion of the chest along with diaphragm relaxation, which overcomes the pressure at the lower oesophageal sphincter (LOS), leading to ascent of gastric content due to the lower intrathoracic pressure [289, 291]. The upper oesophageal sphincter also relaxes with a forward motion of the head, allowing the contents of the oesophagus to enter the mouth and be re‐masticated or spat out.
The process is usually started by the stimulus of a food bolus, and three different types of rumination have been described [310, 311]. First, a primary form of rumination with no specific cause has been identified. Second, where GERD can initiate a rumination event, and third, supragastric belching which also can initiate a rumination event. Rumination syndrome can also be misinterpreted as therapy refractory GERD, with or without associated supragastric belching [306, 312, 313].
Several diagnoses and conditions associated with rumination syndrome have been identified but no causative factor has been conclusively recognized. Studies have demonstrated an overlap with functional dyspepsia, and it has been suggested that rumination syndrome may be triggered by dyspeptic symptoms, as subjects seek relief through venting [297, 314]. Gastric accommodation and emptying in rumination syndrome is probably not of key importance, but gastric sensation may be higher, so less pressure is needed to induce LOS relaxation, which predisposes for rumination episodes [290, 309, 315]. Psychiatric comorbidities such as depression, anxiety, and eating disorders are more common in subjects with rumination syndrome [295, 298, 316].
4.4.5. Associations
Statement 65. Functional dyspepsia, gastroparesis, cyclic vomiting, and other disorders of gut‐brain interaction can overlap and increase the likelihood of rumination syndrome.
Statement endorsed in R1, median panel: 5—Appropriate/agreement
Quality of evidence: low
Statement 66. Gastro‐oesophageal reflux disease and pathological supragastric belching can be mechanisms that provoke and/or aggravate rumination syndrome. In cases of non‐responsive gastroesophageal reflux disease, consideration should be given to rumination syndrome.
Statement endorsed in R1, median panel: 5—Appropriate/agreement
Quality of evidence: low
Rumination syndrome is categorized as primary or idiopathic and secondary when associated with gastroesophageal reflux and/or supragastric belching [310, 317, 318]. Rumination syndrome is a cause of persistent, non‐responding gastroesophageal reflux disease in both adults [306, 318] and paediatrics [306]. Supragastric belching can elicit regurgitation episodes in patients with rumination syndrome and also aggravate oesophageal acid exposure [306, 319, 320]. There is emerging evidence that a subset of patients with rumination syndrome have duodenal eosinophilic inflammation [321, 322], supporting an overlap with functional dyspepsia [297]. Rumination syndrome can overlap with gastroparesis [150, 323], but patients with rumination syndrome can demonstrate either a delay or an acceleration in gastric emptying [315]. Rumination syndrome can also overlap with cyclical vomiting syndrome [298], and the presence of gut‐brain interaction disorders generally increases the likelihood of rumination syndrome [298].
4.4.6. Psychosocial Factors
Statement 67. Rumination syndrome is independently associated with depression and anxiety. Patients with rumination syndrome have a lower physical and mental quality of life and increased somatic symptom reporting (somatization).
Statement endorsed in R1, median panel: 5—Appropriate/agreement
Quality of evidence: moderate
Statement 68. In patients with rumination syndrome, a current or previous associated eating or psychiatric disorder should be considered.
Statement endorsed in R1, median panel: 5—Appropriate/agreement
Quality of evidence: low
A cross‐sectional observational study of adults in the United States found rumination syndrome to be independently associated with depression (OR 1.10, 95% CI 1.05–1.16) [297]. A large global epidemiology study of gut‐brain interaction disorders found rumination syndrome to be independently associated with anxiety (OR 1.8, 95% CI 1.6–2.1) and depression (1.5, 95% CI 1.3–1.7) [298]. Subjects fulfiling the criteria for rumination syndrome had lower physical and mental quality of life, and increased somatic symptom reporting compared with controls. Moreover, increasing frequency of rumination episodes was associated with a clear trend to lower physical and mental quality of life, and greater severity of somatization [298]. In a case‐control study of 72 patients (24 with rumination syndrome and 48 controls), those with rumination syndrome had a significantly higher prevalence of eating disorders (37.5% vs. 4.2%, OR 16.4) and psychiatric disorders (83% vs. 50%, OR 4.5) compared with controls [324]. Specifically, the risks of both anorexia nervosa (16.7% vs. 0%) and bulimia nervosa (21.1% vs. 0%) were increased in patients with rumination syndrome [324].
4.4.7. Diagnosis
Statement 69. Combined clinical and objective assessment using high‐resolution manometry impedance is recommended to confirm the diagnosis of rumination.
Statement endorsed in R1, median panel: 5—Appropriate/agreement
Quality of evidence: low
Rumination syndrome is a global clinical entity [298] and is described as a mental disorder in DSM‐5 and ICD‐11 [325], but as a functional gastrointestinal disorder called rumination syndrome in the Rome classification system [326]. Rome IV includes six diagnostic criteria for rumination syndrome in adults [326]. Although the clinical presentation of rumination syndrome shares some symptoms with other gastrointestinal disorders [113, 288, 321, 327, 328, 329, 330, 331, 332, 333], a large proportion of patients can be identified based on the clinical features of rumination [113, 321, 334]. Surprisingly, no validated screening instruments or questionnaires are available for rumination disorder. Single‐item screening for regurgitation or re‐swallowing of food are included in several questionnaires [335], for instance, the STEP [335, 336]. In terms of rumination diagnostic interviews, the EDA‐5 [337] and the PARDI [338] include questions related to rumination syndrome, but validation studies are required to determine the utility and accuracy of these tests [335].
In contrast, the objective testing of rumination has received a lot of attention in the literature during the last decade. The diagnosis of rumination has been studied using postprandial high‐resolution oesophageal manometry [312, 323, 339, 340], pH‐impedance studies [306] or high‐resolution impedance manometry [318, 341]. High‐resolution manometry (HRM), manometric findings in patients with rumination syndrome show an increase in intragastric pressure of > 30 mm Hg associated with oesophageal pressurization and a clinically recognized rumination episode [310]. There is proximal movement of the gastroesophageal junction from the intra‐abdominal cavity into the thorax due to increased intra‐abdominal pressure at the onset of rumination episodes [311, 342, 343, 344, 345]. In case of diagnostic uncertainty [323], manometric evaluation combined with pH‐impedance monitoring may confirm the diagnosis [306, 312, 346]. Whether HRM is superior to conventional manometry in the diagnostic work‐up of the rumination syndrome needs to be determined in future studies [347]. A large proportion of regurgitation episodes in patients with rumination syndrome are weakly acidic, so pH‐impedance monitoring is superior to pH‐metry for the detection of regurgitation episodes in rumination patients [306, 346, 348]. However, rumination episodes could not be distinguished from GERD on pH‐impedance studies using standard reflux metrics [349]. More “reflux” episodes are noted to extend to the proximal oesophagus in rumination [349]. Baseline impedance values are similar in rumination and GERD, and are not useful for discriminating between these conditions [350]. Combined ambulatory high‐resolution manometry and pH‐impedance had an 86% sensitivity for identification of rumination episodes in a small case series, but this technique is not universally available for clinical use [306, 312, 346]. When rumination is suspected in patients with refractory postprandial regurgitation, high‐resolution manometry with impedance (HRIM) (stationary, postprandial [351]) is indicated to distinguish rumination from GERD [312, 318, 352, 353, 354]. HRIM allows combined evaluation of oesophageal function, bolus transit and clearance [354]. When performed during postprandial periods or following test meals, HRIM can be used to diagnose rumination [354], as it allows detection of increased gastric pressure as well as retrograde bolus flow. This use of postprandial HRIM to document rumination may help indicate behavioural therapies amongst patients with ongoing symptoms despite PPI therapy [318]. This is crucial, considering that rumination can benefit more from behavioural interventions than from medical therapy or surgery [318, 354, 355].
4.4.8. Non‐Pharmacological Treatment Options
Statement 70. Diaphragmatic breathing with or without biofeedback (visual or verbal feedback on abdominal, intercostal, or diaphragm muscle activity using either electromyography or oesophageal impedance manometry) is the first‐line therapy for rumination syndrome.
Statement endorsed in R1, median panel: 5—Appropriate/agreement
Quality of evidence: moderate
Medical treatments for rumination syndrome are limited [356]. The most studied and effective therapy for rumination syndrome is diaphragmatic breathing with or without a biofeedback component. Biofeedback means that patients receive visual or verbal feedback on abdominal, intercostal or diaphragm muscle activity using either electromyography or oesophageal high‐resolution impedance manometry.
Diaphragmatic breathing without biofeedback can be taught to patients and is effective, but rumination episodes restart promptly when patients resume their normal breathing pattern [357]. This was evaluated in a study of 16 patients who were instructed in diaphragmatic breathing during a postprandial HRIM: the technique led to decreased gastric pressure and increased esophago‐gastric junction pressure [357]. The strongest evidence of benefit of diaphragmatic breathing with biofeedback comes from two single randomized trials. In the first, patients with rumination syndrome learnt the biofeedback technique based on electromyography (EMG)‐guided control of abdomino‐thoracic muscular activity. In three biofeedback sessions, patients were instructed to voluntarily reduce the activity of intercostal and anterior abdominal muscles and to increase the activity of the diaphragm and were given visual feedback on muscle activity shown on a monitor, after each biofeedback session. Patients were instructed to perform the same exercises daily at home for 5 min before and after meals. With this technique, regurgitation episodes decreased significantly from 27 ± 1 regurgitation episodes/day at baseline to 8 ± 2 episodes/day immediately after treatment [291]. Applying the same methodology in a second study, 24 patients were randomized to either diaphragmatic breathing with biofeedback or placebo. Only patients receiving biofeedback treatment reduced rumination activity [358]. In rumination syndrome psychological interventions (e.g., cognitive behavioural therapy (CBT), hypnosis) have been used but there are no randomized studies to demonstrate the objective response [359].
4.4.9. Pharmacological Treatment Options
Statement 71. In patients with rumination syndrome pharmacological treatment with baclofen or tricyclic antidepressants can be used if diaphragmatic breathing/biofeedback are not available or patient does not respond.
Statement endorsed in R1, median panel: 5—Appropriate/agreement
Quality of evidence: low
Statement 72. In patients with secondary rumination syndrome, it is necessary to treat underlying gastroesophageal reflux with PPI.
Statement endorsed in R1, median panel: 5—Appropriate/agreement
Quality of evidence: low
Baclofen has been proposed as a pharmacological agent for rumination syndrome because it increases the pressure and reduces transient relaxations of the lower oesophageal sphincter. An initial open‐label study found that baclofen decreased the number of rumination episodes by 68% [360]. A subsequent randomized, placebo‐controlled study confirmed this finding to a milder degree [356]. This later study also found that some patients taking baclofen experienced notable side effects, including sleepiness, dizziness, and acral paraesthesia, but these resolved in less than 2 days in all cases.
A single open‐label study evaluated the effect of combining diaphragmatic breathing with low‐dose tricyclic antidepressants, with the objective of reducing the associated gastric visceral hypersensitivity and anxiety, and found that 91% of patients with rumination syndrome reported an improvement in their symptoms [361] (Table 3).
4.4.10. Nutritional Support
Statement 73. Although most patients with rumination syndrome have only modest weight loss, patient‐tailored dietetic assessment for severe cases of rumination is indicated.
Statement endorsed in R1, median panel: 4—Appropriate/agreement
Quality of evidence: low
Although patients with rumination syndrome have only modest weight loss [308, 334, 362], some case reports describe severe malnutrition and need for nutritional support [363, 364, 365]. To date, no data on specific macro‐/micro‐nutrient deficiencies in patients with rumination have been reported in the literature. However, a dietetic assessment performed as part of a multidisciplinary team approach is considered appropriate for the most severe cases [364].
4.5. Chronic Nausea and Vomiting Syndrome
4.5.1. Definition
Statement 74. Chronic Unexplained Nausea is defined by the presence of bothersome nausea, at least twice per week on average, in the absence of abnormalities at upper endoscopy or other disease that explains nausea, with symptoms present the last 3 months and started at least 6 months ago.
Statement endorsed in R1, median panel: 5—Appropriate/agreement
Quality of evidence: high
Statement 75. Chronic Unexplained Vomiting is diagnosed in patients who had on average at least one episode of vomiting per week, in the absence of an eating disorder, rumination, or major psychiatric disease, in absence of self‐induced induced vomiting, chronic cannabinoid use, or abnormalities in the central nervous system or metabolic diseases likely to explain the recurrent vomiting, with symptoms present the last 3 months and started at least 6 months ago.
Statement endorsed in R1, median panel: 5—Appropriate/agreement
While the sensation of “nausea” is readily expressed by chronic nausea and vomiting syndrome (CNVS) patients, its meaning is not uniform across subjects and cultures, and to some patients it represents a generalized sense of malaise and even fatigue [366]. The Rome consensus defined nausea in the classical medical symptom sense, as a sick sensation that precedes the need or desire to vomit, and which may be felt predominantly in the epigastrium or the throat [314]. Vomiting is defined as the forceful oral expulsion of gastric contents associated with contraction of the muscles of the abdominal and chest wall.
The Rome IV consensus defined chronic nausea and vomiting syndrome based on the presence of chronic unexplained nausea and/or chronic unexplained nausea vomiting following the criteria stated above [314].
4.5.2. Epidemiology
Statement 76. Chronic nausea and vomiting syndrome, as defined according to the Rome IV criteria, has an estimated prevalence of 1%.
Statement endorsed in R1, median panel: 5—Appropriate/agreement
Quality of evidence: low
Data on the epidemiology of CNVS in the scientific community is scarce [1]. The highest quality evidence is available from the Rome Foundation Global Epidemiology Study, in which survey data from 6300 individuals across the United States, UK and Canada was collected [245]. The prevalence of chronic nausea and vomiting syndrome according to the Rome IV criteria was ∼1% (58/6300).
Jung et al. evaluated the prevalence of clinically significant chronic nausea in general population in 5096 South Korean individuals via telephone survey [367]. Cases were defined as chronic unexplained nausea after exclusion of organic causes through the meticulous medical examination and if the frequency of nausea was ‘more than one day per week'. Its prevalence was 1.6% (1.4%–1.8%) and about 90% of nausea was not accompanied by vomiting. Camilleri et al. reported on results of a telephone survey of 21,128 adults in the United States [368]. Nausea and vomiting were present in 9.5% and 2.7% of individuals at least once during the past 3 months, respectively. When considering a frequency of at least once per week (considered clinically relevant), the prevalence was 2.2% and 0.4%, respectively, for nausea and vomiting.
4.5.3. Signs and Symptoms
Statement 77. Chronic nausea and vomiting syndrome is characterized by continuous, non‐episodic symptoms of unexplained nausea and vomiting.
Statement endorsed in R1, median panel: 5—Appropriate/agreement
Quality of evidence: moderate
Unlike occasional vomiting, for example, in case of functional dyspepsia with other predominant symptoms, unexplained vomiting should occur at least once per month to be considered chronic [314, 369]. Following the Rome IV criteria, CNVS presents with vomiting episodes of ≥ 1/week, with or without nausea for the past 3 months (onset ≥ 6 months before diagnosis) [314]. Vomiting in the absence of nausea may be caused by a central nervous system disease, and other systemic, organic or metabolic diseases should be excluded before considering a diagnosis of CNVS [314]. In addition, vomiting should not be self‐induced (e.g., bulimia nervosa with binge episodes) and distinguished from regurgitation and rumination [1, 314].
4.5.4. Pathophysiological Mechanisms
Statement 78. The development and maintenance of chronic nausea and vomiting syndrome is best explained by the biopsychosocial model of disease encompassing biological, psychological, and social aspects.
Statement endorsed in R1, median panel: 5—Appropriate/agreement
Quality of evidence: moderate
Studies identified several biological, psychological and social aspects contributing to CNVS. Regarding the biological component, an overlap with migraine has been shown [196, 235, 236, 370, 371]. On a functional basis, gastric emptying may be either normal, accelerated or delayed [245, 372]. Gastric electrophysiology can be altered with abnormal frequency or uncoupling [228, 373], possibly related to histologically visible neuropathies (e.g. fewer interstitial cells of Cajal [374]) or myopathies, serum autoimmune abnormalities [373] or autonomic nerve dysfunction [67, 68, 69, 227, 230, 375]. In the brain, chronic nausea and vomiting syndrome may be related to chronic vestibular dysfunction [73].
In terms of the psychological component, an association exists between CNVS and psychological comorbidities [216, 376], symptoms, such as dizziness [377], as well as other functional disorders [229], such as IBS [196, 220] or evacuation disorders [173]. Regarding the social component, independent factors associated with CNVS include increasing somatic symptom severity and lower quality of life [245].
4.5.5. Associations
Statement 79. Independent factors associated with chronic nausea and vomiting syndrome are younger age, presence of IBS, and functional dyspepsia.
Statement endorsed in R1, median panel: 4—Appropriate/agreement
Quality of evidence: moderate‐C
As the aetiology of CNVS is diverse and not limited to the gastrointestinal tract, it is difficult to find common predisposing factors. There is limited data in the literature about this topic, most based on expert opinions derived from review articles [1, 224, 314, 378]. Consequently, the level of evidence is low. Aziz 2019 et al. reported that independent factors associated with functional nausea and vomiting disorders are younger age, presence of IBS and functional dyspepsia [245].
4.5.6. Psychosocial Factors
Statement 80. Psychological distress with mood disorders, anxiety disorders, somatization disorders, and catastrophizing may be associated with chronic unexplained nausea and vomiting.
Statement endorsed in R1, median panel: 5—Appropriate/agreement
Quality of evidence: low
CNVS adheres to a biopsychosocial model in the field of neurogastroenterology, resulting from complex and reciprocal interactions between biological, psychological, and social factors, rather than from linear monocausal etiopathogenic processes [224, 250, 314, 379]. Indeed, symptoms are conceptually generated based on a complex interaction between factors such as gut dysbiosis, altered mucosal immune function, altered gut signalling (e.g. visceral hypersensitivity), and central nervous system dysregulation of the modulation of gut signalling and motor function. The physiologic feature of gastric emptying may be either normal, accelerated or delayed [245]. A stressful life and emotional events are associated with symptom exacerbation [376, 379, 380], and early‐life adverse events, such as physical or sexual abuse, are also prevalent [379, 381]. Nausea is a common symptom in patients with pain‐associated functional gastrointestinal disorders that correlates with poor school and social functioning [382] and reduces patients' quality of life [383]. A perturbation in interoception processing is probably also involved [2, 384]. Psychological distress with mood disorders, anxiety disorders, somatization disorders, and catastrophizing may also be associated.
4.5.7. Diagnosis
Statement 81. Chronic nausea and vomiting syndrome is diagnosed based on clinical criteria after previous exclusion of systemic, organic, or metabolic diseases by objective testing.
Statement endorsed in R1, median panel: 5—Appropriate/agreement
Quality of evidence: low
Following the Rome IV criteria, possible systemic, organic or metabolic diseases should be excluded before a diagnosis of CNVS [314]. Although the endoscopic detection of food in the stomach after an overnight fast may be indicative of gastroparesis, confirmation of delayed gastric emptying with scintigraphy or breath tests is mandatory according to the recent European consensus on gastroparesis [1, 133]. Following exclusion of a mechanical obstruction, antroduodenal manometry is useful to exclude dysmotility [1, 314]. In addition, oesophageal manometry or pH‐testing is indicated when suspecting achalasia or gastro‐esophageal reflux, respectively [1, 314]. Metabolic abnormalities (less common and usually presenting with CVS in childhood) require more complex plasma (ammonia, amino acids) and urine (organic acids, amino‐levulinic acid and porphobilinogen levels) testing [205, 314].
Recordings of gastric myoelectrical activity by electrogastrography (EGG), may identify dysrhythmias in patients with chronic unexplained nausea and vomiting, although this technique is only available at highly specialized centres [385]. Recently, the technique has evolved to high‐resolution electrogastrography mapping, and shown to detect electrophysiological patterns that correlate with specific gastroduodenal symptom profiles [386].
Histological and molecular analyses of full‐thickness gastric biopsies from patients with chronic unexplained nausea and vomiting have evidenced a loss of pacemaker interstitial cells of Cajal (ICCs) and macrophage‐based immune dysregulation [374, 387]. At present, gastric full‐thickness biopsies are surgically obtained at specialized referral centres for comprehensive evaluation of patients with severe refractory unexplained nausea and vomiting [388].
4.5.8. Non‐Pharmacological Treatment Options
Statement 82. In refractory cases of chronic nausea and vomiting syndrome, gastric electrical stimulation can be considered.
Statement endorsed in R2, median panel: 4—Appropriate/agreement
Quality of evidence: moderate
Besides pharmacological treatments, as in irritable bowel syndrome, a non‐pharmacological approach to CNVS based on the dogma of gut‐brain interaction disorder is possible. However, the available data on hypnosis, cognitive behavioural therapy and others are poor or fragmented, or apply to non‐functional GI disorders. Several bioelectric therapies have been advocated for CNVS. The most well studied is gastric electrical stimulation (GES). A recent meta‐analysis including 730 patients concluded that GES improves gastroparesis symptoms and specifically reduces the frequency of weekly vomiting episodes [389]. GES is effective in the long‐term in patients with medically refractory nausea and vomiting, showing an efficacy of 50% at 5 years [390] and 10 years [391] in an intention‐to‐treat analysis. Non‐invasive vagus nerve stimulation performed for 4 weeks in patients with idiopathic gastroparesis significantly improved nausea/vomiting but there was no control group [392].
Hypnotherapy (gut‐directed hypnotherapy, 3‐month intervention period) is more effective than standard medical treatment in reducing nausea symptoms in children with functional nausea during treatment and at the 6‐month follow‐up visit, but not at the 12‐month follow‐up evaluation [393, 394]. Hypnosis is of interest in the management of anticipatory nausea and vomiting [395] and nausea and vomiting in cancer therapy [396] or pregnancy [397] and could be extrapolated to CNVS in adults. Hypnotherapy could possibly be used to treat early‐life trauma with hypno‐analysis. One study suggested that acupressure wristbands were ineffective in relieving nausea and vomiting in hospice patients [398]. Most studies of complementary and alternative therapies for nausea and vomiting have been performed in the setting of chemotherapy and anticipatory nausea and vomiting. Treatments investigated have included behavioural therapies, acupuncture, and ginger, but it is unclear if such strategies can be extrapolated to patients not undergoing chemotherapy [399]. An integrative healthcare model with heartfulness meditation and care coordination improved outcome in CVS [400] but data are lacking in CNVS.
4.5.9. Pharmacological Treatment Options
Statement 83. Histamine H1 antagonists (e.g., meclizine, promethazine) are effective for the treatment of chronic nausea and vomiting.
Statement Endorsed in R2, median panel: 4—Appropriate/neutral
Quality of evidence: low
Statement 84. Muscarinic M1 antagonists (e.g., scopolamine) are effective for the treatment of chronic nausea and vomiting.
Statement Endorsed in R2, median panel: 3—Uncertain/disagreement
Quality of evidence: low
Statement 85. Dopamine‐2 antagonists are effective for the treatment of chronic nausea and vomiting.
Statement endorsed in R1, median panel: 4—Appropriate/agreement
Quality of evidence: low
Statement 86. 5‐HT3 antagonists are effective for the treatment of chronic nausea and vomiting.
Statement endorsed in R1, median panel: 4—Appropriate/agreement
Quality of evidence: low
Statement 87. Tricyclic antidepressants are effective for the treatment of chronic nausea and vomiting.
Statement endorsed in R1, median panel: 4—Appropriate/agreement
Quality of evidence: low
Statement 88. Mirtazapine is effective for the treatment of chronic nausea and vomiting.
Statement endorsed in R1, median panel: 4—Appropriate/agreement
Quality of evidence: low
Statement 89. Gabapentin is effective for the treatment of chronic nausea and vomiting.
Statement endorsed in R2, median panel: 3—Uncertain/disagreement
Quality of evidence: low
Statement 90. Olanzapine is effective for the treatment of chronic nausea and vomiting.
Statement endorsed in R2, median panel: 4—Appropriate/neutral
Quality of evidence: low
Statement 91. Cannabinoids are effective for the treatment of chronic nausea and vomiting.
Statement endorsed in R2, median panel: 3—Uncertain/neutral
Quality of evidence: low
Statement 92. NK‐1 antagonists are effective for the treatment of chronic nausea and vomiting.
Statement endorsed in R1, median panel: 4—Appropriate/agreement
Quality of evidence: low
The pharmacological treatment of CNVS has been addressed in only a relatively small number of studies. Several classes of drugs with antiemetic capabilities have been developed, including histamine H1 antagonists (e.g. meclizine, promethazine), muscarinic M1 antagonists (e.g. scopolamine), dopamine D2 antagonists (e.g. prochlorperazine), serotonin 5‐HT3 antagonists (e.g. ondansetron, granisetron), neurokinin NK1 antagonists (e.g. aprepitant), and cannabinoids (e.g. dronabinol) [250, 401] (Table 3). A few case series of 5‐HT3 antagonists, approved in the setting of cancer chemotherapy, report efficacy in nausea and vomiting, mostly in patients with gastroparesis [402, 403, 404].
Tricyclic antidepressant agents (e.g. amitriptyline, nortriptyline, desipramine) have been reported as beneficial in uncontrolled series of patients with functional vomiting, while in one controlled trial in functional dyspepsia, amitriptyline improved nausea [405, 406]. In a retrospective report of 94 patients fulfiling Rome III criteria for chronic idiopathic nausea or functional vomiting, 72% experienced at least moderate symptomatic improvement and 22% noted symptom remission with neuromodulators—primarily tricyclic agents (66 patients), but also norepinephrine dopamine reuptake inhibitors (10 patients), selective serotonin reuptake inhibitors (5 patients), serotonin norepinephrine reuptake inhibitors (5 patients), and other agents (9 patients) [405]. An open‐label series and several case reports suggest efficacy with mirtazapine, an antidepressant that has nausea‐suppressive properties probably due to histamine‐1 receptor antagonism [407, 408]. In a controlled trial in functional dyspepsia, mirtazapine improved nausea [409].
Emerging data from other indications support potential efficacy with other neuromodulators, such as the delta ligand gabapentin, the atypical antipsychotic agent olanzapine, and cannabinoids, but evidence on these agents in the treatment of chronic nausea and vomiting syndrome remains scant [408]. While cannabinoids may have some efficacy in chemotherapy‐induced nausea and vomiting, studies in CNVS are lacking [410]. The NK1 antagonist aprepitant improved nausea and vomiting symptoms in a controlled trial in patients with symptoms suggestive of gastroparesis, but a large subset of this series had a normal gastric emptying rate [411].
The identification of serum autoantibodies again various channelopathies has led to the use of intravenous immunoglobulin in patients with severe refractory nausea and vomiting [412, 413].
4.5.10. Nutritional support
Statement 93. In patients with chronic nausea and vomiting syndrome, attention must be given to adequate nutrition, including vitamins and minerals.
Statement endorsed in R1, median panel: 5—Appropriate/agreement
Quality of evidence: very low
Statement 94. Nutritional deficits shall be corrected by dietary modifications and oral supplementation, if possible.
Statement endorsed in R1, median panel: 5—Appropriate/agreement
Quality of evidence: very low
There are no relevant scientific studies that have investigated the role of nutritional support for patients with CNVS. However, there is literature on nutritional management of gastroparesis which may have clinical implications for the treatment of patients with CNVS.
In a study on 305 patients with gastroparesis the BlockBrief 2000 food frequency questionnaire was used to estimate caloric, vitamin and mineral intake [414]. They observed that mean caloric intake was reduced to 58% of daily energy requirements and that 64% of patients reported caloric‐deficient diets, defined as less than 60% of estimated energy requirements. Deficiencies were also shown for several vitamins and minerals.
Published reviews and guidelines [12, 62, 114, 117, 133, 415] generally suggest that dietary modifications represent the first line of treatment for gastroparesis, regardless of disease severity. As patients often have early satiety, they are recommended to eat small meals and to avoid foods high in fat and indigestible fibres because they delay gastric emptying [62, 416]. When small meals are eaten, more frequent meals may be required to maintain caloric intake. Patients are advised to consume liquids as the gastric emptying of caloric liquids or homogenized solids is often preserved in patients with gastroparesis [62, 417]. A high‐fat diet with solid meals increases the severity and frequency of symptoms among patients with gastroparesis [416], whereas a small‐particle‐size diet reduces upper GI symptoms in patients with diabetic gastroparesis [418].
Conflicts of Interest
C.M. reports receipt of research support from Alfasigma. D.K. acknowledges receipt of grants and research support from UEG (guideline for faecal incontinence), MLDS (Dutch Foundation for Gastroenterology), Rome Foundation, ZonMw (Dutch governmental), and Horizon 2020 (EU). In addition, D.K. has received support from Allergan, Grunenthal, and Will Pharma. D.K. has participated in a company‐sponsored speaker’s bureau for Dr. Falk, with payments directed to the host institution. J.S. declares receiving grants and research support from Bayer and Laboratorios Salvat SA. Additionally, J.S. reports receiving advisory, honoraria, or consultant fees from Norgine and Reckitt Benckiser. J.S. has participated in company‐sponsored speaker’s bureaus for Norgine, Cassen Recordati, Bayer, and Grünenthal. M.C. discloses being a co‐investigator on a grant sponsored by Sanofi, and serving as a consultant for Sanofi, Mayoly, RB, and Arena. N.R. reports owning intellectual property in a patent family related to pressure‐flow analytics. R.D.G. reports having received grants and research support, as well as advisory, honoraria, or consultant fees from Kyowa Kirin International and Takeda. All other authors have declared no conflicts of interest in relation to this study.
Supporting information
Supporting Information S1
Supporting Information S2
Acknowledgements
Celia Miguel Blanco, Beatriz Albuixech and Anchel González Barriga, from Medical Science Consulting (Spain), provided editorial support, in the form of medical writing, assembling tables based on authors' detailed directions, collating author comments, copyediting, fact‐checking, and referencing.
The full list of members and affiliations of the Working Group is provided the Supplementary Material.
Funding: These guidelines have been funded by United European Gastroenterology.
For a complete list of the International Working Group for the European Guideline on Chronic Nausea and Vomiting, see the Acknowledgments section.
[Correction added on 10 January 2025, after first online publication: The author name ‘Luis Gerardo Alcalá‐González’ has been corrected.]
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
References
- 1. Lacy B. E., Parkman H. P., and Camilleri M., “Chronic Nausea and Vomiting: Evaluation and Treatment,” American Journal of Gastroenterology 113, no. 5 (2018): 647–659: Epub 20180315, 10.1038/s41395-018-0039-2. [DOI] [PubMed] [Google Scholar]
- 2. Heckroth M., Luckett R. T., Moser C., Parajuli D., and Abell T. L., “Nausea and Vomiting in 2021: A Comprehensive Update,” Journal of Clinical Gastroenterology 55, no. 4 (2021): 279–299, 10.1097/mcg.0000000000001485. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Fink A., Kosecoff J., Chassin M., and Brook R. H., “Consensus Methods: Characteristics and Guidelines for Use,” American Journal of Public Health 74, no. 9 (1984): 979–983, 10.2105/ajph.74.9.979. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Fitch K., Bernstein S. J., Aguilar M. D., et al., RAND/UCLA Appropriateness Method User's Manual (Santa Monica, CA: RAND corporation, 2000). [Google Scholar]
- 5. Hutchings A., Raine R., Sanderson C., and Black N., “A Comparison of Formal Consensus Methods Used for Developing Clinical Guidelines,” Journal of Health Services Research & Policy 11, no. 4 (2006): 218–224, 10.1258/135581906778476553. [DOI] [PubMed] [Google Scholar]
- 6. McMillan S. S., King M., and Tully M. P., “How to Use the Nominal Group and Delphi Techniques,” International Journal of Clinical Pharmacy 38, no. 3 (2016): 655–662: Epub 20160205, 10.1007/s11096-016-0257-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Mullen P. M., “Delphi: Myths and Reality,” Journal of Health, Organisation and Management 17, no. 1 (2003): 37–52, 10.1108/14777260310469319. [DOI] [PubMed] [Google Scholar]
- 8. Richardson W. S., Wilson M. C., Nishikawa J., and Hayward R. S., “The Well‐Built Clinical Question: A Key to Evidence‐Based Decisions,” ACP Journal Club 123, no. 3 (1995): A12–A13. [PubMed] [Google Scholar]
- 9. Guyatt G. H., Oxman A. D., Vist G. E., et al., “GRADE: An Emerging Consensus on Rating Quality of Evidence and Strength of Recommendations,” BMJ 336, no. 7650 (2008): 924–926, 10.1136/bmj.39489.470347.AD. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Scorza K., Williams A., Phillips J. D., and Shaw J., “Evaluation of Nausea and Vomiting,” American Family Physician 76, no. 1 (2007): 76–84. [PubMed] [Google Scholar]
- 11. Tome J., Kamboj A. K., and Sweetser S., “A Practical 5‐Step Approach to Nausea and Vomiting,” Mayo Clinic Proceedings 97, no. 3 (2022): 600–608, 10.1016/j.mayocp.2021.10.030. [DOI] [PubMed] [Google Scholar]
- 12. Quigley E. M., Hasler W. L., and Parkman H. P., “AGA Technical Review on Nausea and Vomiting,” Gastroenterology 120, no. 1 (2001): 263–286, 10.1053/gast.2001.20516. [DOI] [PubMed] [Google Scholar]
- 13. Marasco G., Lenti M. V., Cremon C., et al., “Implications of SARS‐CoV‐2 Infection for Neurogastroenterology,” Neuro‐Gastroenterology and Motility 33, no. 3 (2021): e14104: Epub 20210216, 10.1111/nmo.14104. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Chigr F., Merzouki M., and Najimi M., “Autonomic Brain Centers and Pathophysiology of COVID‐19,” ACS Chemical Neuroscience 11, no. 11 (2020): 1520–1522: Epub 20200519, 10.1021/acschemneuro.0c00265. [DOI] [PubMed] [Google Scholar]
- 15. Akiho H., Ihara E., Motomura Y., and Nakamura K., “Cytokine‐Induced Alterations of Gastrointestinal Motility in Gastrointestinal Disorders,” World Journal of Gastrointestinal Pathophysiology 2, no. 5 (2011): 72–81, 10.4291/wjgp.v2.i5.72. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Abell T. L., Kedar A., Stocker A., et al., “Pathophysiology of Gastroparesis Syndromes Includes Anatomic and Physiologic Abnormalities,” Digestive Diseases and Sciences 66, no. 4 (2021): 1127–1141: Epub 20200423, 10.1007/s10620-020-06259-6. [DOI] [PubMed] [Google Scholar]
- 17. Basile D., Di Nardo P., Corvaja C., et al., “Mucosal Injury During Anti‐cancer Treatment: From Pathobiology to Bedside,” Cancers 11, no. 6 (2019): 857: Epub 20190620, 10.3390/cancers11060857. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Blijlevens N. and Sonis S., “Palifermin (Recombinant Keratinocyte Growth Factor‐1): A Pleiotropic Growth Factor With Multiple Biological Activities in Preventing Chemotherapy‐ and Radiotherapy‐Induced Mucositis,” Annals of Oncology 18, no. 5 (2007): 817–826: Epub 20061009, 10.1093/annonc/mdl332. [DOI] [PubMed] [Google Scholar]
- 19. Logan R. M., Stringer A. M., Bowen J. M., et al., “The Role of Pro‐inflammatory Cytokines in Cancer Treatment‐Induced Alimentary Tract Mucositis: Pathobiology, Animal Models and Cytotoxic Drugs,” Cancer Treatment Reviews 33, no. 5 (2007): 448–460: Epub 20070515, 10.1016/j.ctrv.2007.03.001. [DOI] [PubMed] [Google Scholar]
- 20. O'Brien B. J., Rusthoven J., Rocchi A., et al., “Impact of Chemotherapy‐Associated Nausea and Vomiting on Patients' Functional Status and on Costs: Survey of Five Canadian Centres,” Canadian Medical Association Journal 149, no. 3 (1993): 296–302. [PMC free article] [PubMed] [Google Scholar]
- 21. Vanderbecq Q., Ardon R., De Reviers A., et al., “Adhesion‐Related Small Bowel Obstruction: Deep Learning for Automatic Transition‐Zone Detection by CT,” Insights Imaging 13, no. 1 (2022): 13: Epub 20220124, 10.1186/s13244-021-01150-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Ten Broek R. P. G., Krielen P., Di Saverio S., et al., “Bologna Guidelines for Diagnosis and Management of Adhesive Small Bowel Obstruction (ASBO): 2017 Update of the Evidence‐Based Guidelines From the World Society of Emergency Surgery ASBO Working Group,” World Journal of Emergency Surgery 13, no. 1 (2018): 24: Epub 20180619, 10.1186/s13017-018-0185-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Rami Reddy S. R. and Cappell M. S., “A Systematic Review of the Clinical Presentation, Diagnosis, and Treatment of Small Bowel Obstruction,” Current Gastroenterology Reports 19, no. 6 (2017): 28, 10.1007/s11894-017-0566-9. [DOI] [PubMed] [Google Scholar]
- 24. Taylor M. R. and Lalani N., “Adult Small Bowel Obstruction,” Academic Emergency Medicine 20, no. 6 (2013): 528–544, 10.1111/acem.12150. [DOI] [PubMed] [Google Scholar]
- 25. Khaled W., Millet I., Corno L., et al., “Clinical Relevance of the Feces Sign in Small‐Bowel Obstruction Due to Adhesions Depends on its Location,” American Journal of Roentgenology 210, no. 1 (2018): 78–84: Epub 20171018, 10.2214/ajr.17.18126. [DOI] [PubMed] [Google Scholar]
- 26. Ros P. R. and Huprich J. E., “ACR Appropriateness Criteria on Suspected Small‐Bowel Obstruction,” Journal of the American College of Radiology 3, no. 11 (2006): 838–841, 10.1016/j.jacr.2006.09.018. [DOI] [PubMed] [Google Scholar]
- 27. Belkacemi L. and Darmani N. A., “Dopamine Receptors in Emesis: Molecular Mechanisms and Potential Therapeutic Function,” Pharmacological Research 161 (2020): 105124: Epub 20200816, 10.1016/j.phrs.2020.105124. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Zhou C. Q., Zhang J. W., Wang M., and Peng G. G., “Meta‐analysis of the Efficacy and Safety of Long‐Acting Non‐Ergot Dopamine Agonists in Parkinson's Disease,” Journal of Clinical Neuroscience 21, no. 7 (2014): 1094–1101: Epub 20140429, 10.1016/j.jocn.2013.10.041. [DOI] [PubMed] [Google Scholar]
- 29. Kurin M., Bielefeldt K., and Levinthal D. J., “Prevalence of Nausea and Vomiting in Adults Using Ropinirole: A Systematic Review and Meta‐Analysis,” Digestive Diseases and Sciences 63, no. 3 (2018): 687–693: Epub 20180130, 10.1007/s10620-018-4937-3. [DOI] [PubMed] [Google Scholar]
- 30. Coluzzi F., Rocco A., Mandatori I., and Mattia C., “Non‐Analgesic Effects of Opioids: Opioid‐Induced Nausea and Vomiting: Mechanisms and Strategies for Their Limitation,” Current Pharmaceutical Design 18, no. 37 (2012): 6043–6052, 10.2174/138161212803582540. [DOI] [PubMed] [Google Scholar]
- 31. Moore R. A. and McQuay H. J., “Prevalence of Opioid Adverse Events in Chronic Non‐Malignant Pain: Systematic Review of Randomised Trials of Oral Opioids,” Arthritis Research and Therapy 7, no. 5 (2005): R1046–R1051: Epub 20050628, 10.1186/ar1782. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Laugsand E. A., Kaasa S., and Klepstad P., “Management of Opioid‐Induced Nausea and Vomiting in Cancer Patients: Systematic Review and Evidence‐Based Recommendations,” Palliative Medicine 25, no. 5 (2011): 442–453, 10.1177/0269216311404273. [DOI] [PubMed] [Google Scholar]
- 33. Borner T., Tinsley I. C., Doyle R. P., Hayes M. R., and De Jonghe B. C., “Glucagon‐Like Peptide‐1 in Diabetes Care: Can Glycaemic Control Be Achieved Without Nausea and Vomiting?,” British Journal of Pharmacology 179, no. 4 (2022): 542–556: Epub 20210914, 10.1111/bph.15647. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Maselli D. B. and Camilleri M., “Effects of GLP‐1 and its Analogs on Gastric Physiology in Diabetes Mellitus and Obesity,” Advances in Experimental Medicine & Biology 1307 (2021): 171–192, 10.1007/5584_2020_496. [DOI] [PubMed] [Google Scholar]
- 35. Sikirica M. V., Martin A. A., Wood R., Leith A., Piercy J., and Higgins V., “Reasons for Discontinuation of GLP1 Receptor Agonists: Data From a Real‐World Cross‐Sectional Survey of Physicians and Their Patients With Type 2 Diabetes,” Diabetes Metab Syndr Obes 10 (2017): 403–412: Epub 20170929, 10.2147/dmso.S141235. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Bettge K., Kahle M., Abd El Aziz M. S., Meier J. J., and Nauck M. A., “Occurrence of Nausea, Vomiting and Diarrhoea Reported as Adverse Events in Clinical Trials Studying Glucagon‐like Peptide‐1 Receptor Agonists: A Systematic Analysis of Published Clinical Trials,” Diabetes, Obesity and Metabolism 19, no. 3 (2017): 336–347: Epub 20161219, 10.1111/dom.12824. [DOI] [PubMed] [Google Scholar]
- 37. AbuRahma A. F. and Choueiri M. A., “Cranial and Cervical Nerve Injuries After Repeat Carotid Endarterectomy,” Journal of Vascular Surgery 32, no. 4 (2000): 649–654, 10.1067/mva.2000.109751. [DOI] [PubMed] [Google Scholar]
- 38. Suen H. C., Hendrix H., and Patterson G. A., “Physiologic Consequences of Pneumonectomy. Consequences on the Esophageal Function,” Chest Surgery Clinics of North America 9, no. 2 (1999): 475–483, xiii. [PubMed] [Google Scholar]
- 39. Au J., Hawkins T., Venables C., et al., “Upper Gastrointestinal Dysmotility in Heart‐Lung Transplant Recipients,” Ann Thorac Surg 55, no. 1 (1993): 94–97, 10.1016/0003-4975(93)90480-6. [DOI] [PubMed] [Google Scholar]
- 40. Sodhi S. S., Guo J. P., Maurer A. H., O'Brien G., Srinivasan R., and Parkman H. P., “Gastroparesis After Combined Heart and Lung Transplantation,” Journal of Clinical Gastroenterology 34, no. 1 (2002): 34–39, 10.1097/00004836-200201000-00007. [DOI] [PubMed] [Google Scholar]
- 41. Grass F., Schäfer M., Cristaudi A., et al., “Incidence and Risk Factors of Abdominal Complications After Lung Transplantation,” World Journal of Surgery 39, no. 9 (2015): 2274–2281, 10.1007/s00268-015-3098-1. [DOI] [PubMed] [Google Scholar]
- 42. Costa H. F., Malvezzi Messias P., dos Reis F. P., et al., “Abdominal Complications After Lung Transplantation in a Brazilian Single Center,” Transplantation Proceedings 49, no. 4 (2017): 878–881, 10.1016/j.transproceed.2017.03.002. [DOI] [PubMed] [Google Scholar]
- 43. Mertens V., Dupont L., and Sifrim D., “Relevance of GERD in Lung Transplant Patients,” Current Gastroenterology Reports 12, no. 3 (2010): 160–166, 10.1007/s11894-010-0106-3. [DOI] [PubMed] [Google Scholar]
- 44. Berkowitz N., Schulman L. L., McGregor C., and Markowitz D., “Gastroparesis After Lung Transplantation. Potential Role in Postoperative Respiratory Complications,” Chest 108, no. 6 (1995): 1602–1607, 10.1378/chest.108.6.1602. [DOI] [PubMed] [Google Scholar]
- 45. Shafi M. A. and Pasricha P. J., “Post‐Surgical and Obstructive Gastroparesis,” Current Gastroenterology Reports 9, no. 4 (2007): 280–285, 10.1007/s11894-007-0031-2. [DOI] [PubMed] [Google Scholar]
- 46. Yolsuriyanwong K., Marcotte E., Venu M., and Chand B., “Impact of Vagus Nerve Integrity Testing on Surgical Management in Patients With Previous Operations With Potential Risk of Vagal Injury,” Surgical Endoscopy 33, no. 8 (2019): 2620–2628: Epub 20181025, 10.1007/s00464-018-6562-9. [DOI] [PubMed] [Google Scholar]
- 47. Fich A., Neri M., Camilleri M., Kelly K. A., and Phillips S. F., “Stasis Syndromes Following Gastric Surgery: Clinical and Motility Features of 60 Symptomatic Patients,” Journal of Clinical Gastroenterology 12, no. 5 (1990): 505–512, 10.1097/00004836-199010000-00005. [DOI] [PubMed] [Google Scholar]
- 48. Salameh J. R., R. E. Schmieg, Jr. , Runnels J. M., and Abell T. L., “Refractory Gastroparesis After Roux‐En‐Y Gastric Bypass: Surgical Treatment With Implantable Pacemaker,” Journal of Gastrointestinal Surgery 11, no. 12 (2007): 1669–1672: Epub 20070929, 10.1007/s11605-007-0331-8. [DOI] [PubMed] [Google Scholar]
- 49. van Rijn S., Roebroek Y. G., Conchillo J. M., Bouvy N. D., and Masclee A. A., “Effect of Vagus Nerve Injury on the Outcome of Antireflux Surgery: An Extensive Literature Review,” Digestive Surgery 33, no. 3 (2016): 230–239: Epub 20160319, 10.1159/000444147. [DOI] [PubMed] [Google Scholar]
- 50. Frantzides C. T., Carlson M. A., Zografakis J. G., Moore R. E., Zeni T., and Madan A. K., “Postoperative Gastrointestinal Complaints After Laparoscopic Nissen Fundoplication,” Jsls 10, no. 1 (2006): 39–42. [PMC free article] [PubMed] [Google Scholar]
- 51. van der Mijle H. C., Beekhuis H., Bleichrodt R. P., and Kleibeuker J. H., “Transit Disorders of the Gastric Remnant and Roux Limb After Roux‐En‐Y Gastrojejunostomy: Relation to Symptomatology and Vagotomy,” British Journal of Surgery 80, no. 1 (1993): 60–64, 10.1002/bjs.1800800122. [DOI] [PubMed] [Google Scholar]
- 52. Kozarek R. A., Low D. E., and Raltz S. L., “Complications Associated With Laparoscopic Anti‐reflux Surgery: One Multispecialty Clinic's Experience,” Gastrointestinal Endoscopy 46, no. 6 (1997): 527–531, 10.1016/s0016-5107(97)70008-7. [DOI] [PubMed] [Google Scholar]
- 53. Bekelis K., Gottfried O. N., Wolinsky J. P., Gokaslan Z. L., and Omeis I., “Severe Dysphagia Secondary to Posterior C1‐C3 Instrumentation in a Patient With Atlantoaxial Traumatic Injury: A Case Report and Review of the Literature,” Dysphagia 25, no. 2 (2010): 156–160: Epub 20090930, 10.1007/s00455-009-9255-7. [DOI] [PubMed] [Google Scholar]
- 54. Miyazaki S., Taniguchi H., Kusa S., et al., “Factors Associated With Periesophageal Vagal Nerve Injury After Pulmonary Vein Antrum Isolation,” Journal of American Heart Association 3, no. 5 (2014): e001209: Epub 20140923, 10.1161/jaha.114.001209. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55. Park S. Y., Camilleri M., Packer D., and Monahan K., “Upper Gastrointestinal Complications Following Ablation Therapy for Atrial Fibrillation,” Neuro‐Gastroenterology and Motility 29, no. 11 (2017): Epub 20170519, 10.1111/nmo.13109. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56. Jhuo S. J., Lo L. W., Chang S. L., et al., “Periesophageal Vagal Plexus Injury Is a Favorable Outcome Predictor After Catheter Ablation of Atrial Fibrillation,” Heart Rhythm 13, no. 9 (2016): 1786–1793: Epub 20160525, 10.1016/j.hrthm.2016.05.020. [DOI] [PubMed] [Google Scholar]
- 57. Kuwahara T., Takahashi A., Takahashi Y., et al., “Clinical Characteristics and Management of Periesophageal Vagal Nerve Injury Complicating Left Atrial Ablation of Atrial Fibrillation: Lessons From Eleven Cases,” Journal of Cardiovascular Electrophysiology 24, no. 8 (2013): 847–851: Epub 20130329, 10.1111/jce.12130. [DOI] [PubMed] [Google Scholar]
- 58. Miyazaki S., Nakamura H., Taniguchi H., et al., “Gastric Hypomotility After Second‐Generation Cryoballoon Ablation‐Unrecognized Silent Nerve Injury After Cryoballoon Ablation,” Heart Rhythm 14, no. 5 (2017): 670–677, 10.1016/j.hrthm.2017.01.028. [DOI] [PubMed] [Google Scholar]
- 59. Lakkireddy D., Reddy Y. M., Atkins D., et al., “Effect of Atrial Fibrillation Ablation on Gastric Motility: The Atrial Fibrillation Gut Study,” Circ Arrhythm Electrophysiol 8, no. 3 (2015): 531–536: Epub 20150314, 10.1161/circep.114.002508. [DOI] [PubMed] [Google Scholar]
- 60. Koo J., Lam S. K., Chan P., et al., “Proximal Gastric Vagotomy, Truncal Vagotomy With Drainage, and Truncal Vagotomy With Antrectomy for Chronic Duodenal Ulcer. A Prospective, Randomized Controlled Trial,” Annals of Surgery 197, no. 3 (1983): 265–271, 10.1097/00000658-198303000-00004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61. Mistiaen W., Van Hee R., and Bortier H., “Current Status of Proximal Gastric Vagotomy, One Hundred Years After Pavlov: Is it Finally History?,” Acta Chirurgica Belgica 105, no. 2 (2005): 121–126. [PubMed] [Google Scholar]
- 62. Camilleri M., Parkman H. P., Shafi M. A., Abell T. L., and Gerson L., “Clinical Guideline: Management of Gastroparesis,” American Journal of Gastroenterology 108, no. 1 (2013): 18–37: quiz 8. Epub 20121113, 10.1038/ajg.2012.373. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63. Chaves D. M., de Moura E. G., Mestieri L. H., Artifon E. L., and Sakai P., “Endoscopic Pyloromyotomy via a Gastric Submucosal Tunnel Dissection for the Treatment of Gastroparesis After Surgical Vagal Lesion,” Gastrointestinal Endoscopy 80, no. 1 (2014): 164: Epub 20140515, 10.1016/j.gie.2014.03.045. [DOI] [PubMed] [Google Scholar]
- 64. Mehr S. E., Barbul A., and Shibao C. A., “Gastrointestinal Symptoms in Postural Tachycardia Syndrome: A Systematic Review,” Clinical Autonomic Research 28, no. 4 (2018): 411–421: Epub 20180316, 10.1007/s10286-018-0519-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65. Yamakawa M., Watari M., Torii K. I., et al., “gAChR Antibodies in Children and Adolescents With Acquired Autoimmune Dysautonomia in Japan,” Ann Clin Transl Neurol 8, no. 4 (2021): 790–799: Epub 20210223, 10.1002/acn3.51317. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66. Chelimsky G., Madan S., Alshekhlee A., Heller E., McNeeley K., and Chelimsky T., “A Comparison of Dysautonomias Comorbid With Cyclic Vomiting Syndrome and With Migraine,” Gastroenterology research and practice 2009 (2009): 701019–701026: Epub 20100106, 10.1155/2009/701019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67. Venkatesan T., Prieto T., Barboi A., et al., “Autonomic Nerve Function in Adults With Cyclic Vomiting Syndrome: A Prospective Study,” Neuro‐Gastroenterology and Motility 22, no. 12 (2010): 1303–1307, e339, 10.1111/j.1365-2982.2010.01577.x. [DOI] [PubMed] [Google Scholar]
- 68. Rashed H., Abell T. L., Familoni B. O., and Cardoso S., “Autonomic Function in Cyclic Vomiting Syndrome and Classic Migraine,” Digestive Diseases and Sciences 44, no. 8 Suppl (1999): 74S–88S. [PubMed] [Google Scholar]
- 69. Nguyen L., Wilson L. A., Miriel L., et al., “Autonomic Function in Gastroparesis and Chronic Unexplained Nausea and Vomiting: Relationship With Etiology, Gastric Emptying, and Symptom Severity,” Neuro‐Gastroenterology and Motility 32, no. 8 (2020): e13810: Epub 20200215, 10.1111/nmo.13810. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70. Dougherty J. M., Carney M., Hohman M. H., and Emmady P. D., Vestibular Dysfunction. StatPearls. Treasure Island (FL): StatPearls Publishing Copyright © 2023 (StatPearls Publishing LLC, 2023). [Google Scholar]
- 71. Bisdorff A., Von Brevern M., Lempert T., and Newman‐Toker D. E., “Classification of Vestibular Symptoms: Towards an International Classification of Vestibular Disorders,” Journal of Vestibular Research 19, no. 1‐2 (2009): 1–13, 10.3233/ves-2009-0343. [DOI] [PubMed] [Google Scholar]
- 72. Hall C. D., Herdman S. J., Whitney S. L., et al., “Vestibular Rehabilitation for Peripheral Vestibular Hypofunction: An Updated Clinical Practice Guideline From the Academy of Neurologic Physical Therapy of the American Physical Therapy Association,” Journal of Neurologic Physical Therapy 46, no. 2 (2022): 118–177, 10.1097/npt.0000000000000382. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73. Evans T. H. and Schiller L. R., “Chronic Vestibular Dysfunction as an Unappreciated Cause of Chronic Nausea and Vomiting,” SAVE Proceedings 25, no. 3 (2012): 214–217, 10.1080/08998280.2012.11928830. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74. American Gastroenterological Association Medical Position Statement: Nausea and Vomiting.” Gastroenterology 120, no. 1 (2001): 261–263. 10.1053/gast.2001.20515. [DOI] [PubMed] [Google Scholar]
- 75. National Guideline C. National Institute for Health and Care Excellence: Guidelines , Suspected Neurological Conditions: Recognition and Referral (London: National Institute for Health and Care Excellence (NICE) Copyright © NICE May 2019, 2019). [Google Scholar]
- 76. Sharma S., Hashmi M. F., Kumar A. “Intracranial Hypertension.” (2018). [PubMed]
- 77. D. L. Barnett, 2nd , Rosenbaum R. A., and Diaz J. R., “Refractory Nausea and Vomiting in the Setting of Well‐Controlled Idiopathic Intracranial Hypertension,” BMJ Case Reports 2014 (2014): bcr2014203724: Epub 20140603, 10.1136/bcr-2014-203724. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78. Bouges A., AlSaid Y., Chaudhry S., Hassan A., and Cupler E., “Idiopathic Intracranial Hypertension (IIH) Manifesting With Nausea and Vomiting in the Absence of Headache in an Adult (P4. 393),” AAN Enterprises 86, no. 16_supplement (2016), 10.1212/wnl.86.16_supplement.p4.393. [DOI] [Google Scholar]
- 79. Walker H. K., Hall W. D., Hurst J. W. “Clinical Methods: The History, Physical, and Laboratory Examinations.” (1990). [PubMed]
- 80. Raoof N. and Hoffmann J., “Diagnosis and Treatment of Idiopathic Intracranial Hypertension,” Cephalalgia 41, no. 4 (2021): 472–478: Epub 20210225, 10.1177/0333102421997093. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 81. Grover S., Kumar V., Chakrabarti S., et al., “Prevalence and Type of Functional Somatic Complaints in Patients With First‐Episode Depression,” East Asian Arch Psychiatry 22, no. 4 (2012): 146–153. [PubMed] [Google Scholar]
- 82. Haug T. T., Mykletun A., and Dahl A. A., “The Association Between Anxiety, Depression, and Somatic Symptoms in a Large Population: The HUNT‐II Study,” Psychosomatic Medicine 66, no. 6 (2004): 845–851, 10.1097/01.psy.0000145823.85658.0c. [DOI] [PubMed] [Google Scholar]
- 83. Haug T. T., Mykletun A., and Dahl A. A., “The Prevalence of Nausea in the Community: Psychological, Social and Somatic Factors,” General Hospital Psychiatry 24, no. 2 (2002): 81–86, 10.1016/s0163-8343(01)00184-0. [DOI] [PubMed] [Google Scholar]
- 84. Perugi G., Canonico P. L., Carbonato P., et al., “Unexplained Somatic Symptoms During Major Depression: Prevalence and Clinical Impact in a National Sample of Italian Psychiatric Outpatients,” Psychopathology 44, no. 2 (2011): 116–124: Epub 20110112, 10.1159/000319848. [DOI] [PubMed] [Google Scholar]
- 85. Li A., Guessoum S. B., Ibrahim N., Lefèvre H., Moro M. R., and Benoit L., “A Systematic Review of Somatic Symptoms in School Refusal,” Psychosomatic Medicine 83, no. 7 (2021): 715–723, 10.1097/psy.0000000000000956. [DOI] [PubMed] [Google Scholar]
- 86. Beutel M. E., Wiltink J., Ghaemi Kerahrodi J., et al., “Somatic Symptom Load in Men and Women From Middle to High Age in the Gutenberg Health Study ‐ Association With Psychosocial and Somatic Factors,” Scientific Reports 9, no. 1 (2019): 4610: Epub 20190314, 10.1038/s41598-019-40709-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 87. Riedlinger C., Schmidt G., Weiland A., et al., “Which Symptoms, Complaints and Complications of the Gastrointestinal Tract Occur in Patients With Eating Disorders? A Systematic Review and Quantitative Analysis,” Frontiers in Psychiatry 11 (2020): 195: Epub 20200420, 10.3389/fpsyt.2020.00195. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 88. Werlang M. E., Sim L. A., Lebow J. R., and Lacy B. E., “Assessing for Eating Disorders: A Primer for Gastroenterologists,” American Journal of Gastroenterology 116, no. 1 (2021): 68–76, 10.14309/ajg.0000000000001029. [DOI] [PubMed] [Google Scholar]
- 89. Stanculete M. F., Chiarioni G., Dumitrascu D. L., Dumitrascu D. I., and Popa S. L., “Disorders of the Brain‐Gut Interaction and Eating Disorders,” World Journal of Gastroenterology 27, no. 24 (2021): 3668–3681, 10.3748/wjg.v27.i24.3668. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 90. Santonicola A., Siniscalchi M., Capone P., Gallotta S., Ciacci C., and Iovino P., “Prevalence of Functional Dyspepsia and its Subgroups in Patients With Eating Disorders,” World Journal of Gastroenterology 18, no. 32 (2012): 4379–4385, 10.3748/wjg.v18.i32.4379. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 91. Hutson W. R. and Wald A., “Gastric Emptying in Patients With Bulimia Nervosa and Anorexia Nervosa,” American Journal of Gastroenterology 85, no. 1 (1990): 41–46. [PubMed] [Google Scholar]
- 92. Benini L., Todesco T., Dalle Grave R., Deiorio F., Salandini L., and Vantini I., “Gastric Emptying in Patients With Restricting and Binge/purging Subtypes of Anorexia Nervosa,” American Journal of Gastroenterology 99, no. 8 (2004): 1448–1454, 10.1111/j.1572-0241.2004.30246.x. [DOI] [PubMed] [Google Scholar]
- 93. Gibson D., Watters A., and Mehler P. S., “The Intersect of Gastrointestinal Symptoms and Malnutrition Associated With Anorexia Nervosa and Avoidant/restrictive Food Intake Disorder: Functional or Pathophysiologic?‐A Systematic Review,” International Journal of Eating Disorders 54, no. 6 (2021): 1019–1054: Epub 20210527, 10.1002/eat.23553. [DOI] [PubMed] [Google Scholar]
- 94. Bentley A. and Boyd K., “Use of Clinical Pictures in the Management of Nausea and Vomiting: A Prospective Audit,” Palliative Medicine 15, no. 3 (2001): 247–253, 10.1191/026921601678576239. [DOI] [PubMed] [Google Scholar]
- 95. Harris D. G., “Nausea and Vomiting in Advanced Cancer,” British Medical Bulletin 96, no. 1 (2010): 175–185: Epub 20100930, 10.1093/bmb/ldq031. [DOI] [PubMed] [Google Scholar]
- 96. Harder S., Herrstedt J., Isaksen J., et al., “The Nature of Nausea: Prevalence, Etiology, and Treatment in Patients With Advanced Cancer Not Receiving Antineoplastic Treatment,” Supportive Care in Cancer 27, no. 8 (2019): 3071–3080: Epub 20190104, 10.1007/s00520-018-4623-1. [DOI] [PubMed] [Google Scholar]
- 97. Stephenson J. and Davies A., “An Assessment of Aetiology‐Based Guidelines for the Management of Nausea and Vomiting in Patients With Advanced Cancer,” Supportive Care in Cancer 14, no. 4 (2006): 348–353: Epub 20051015, 10.1007/s00520-005-0897-1. [DOI] [PubMed] [Google Scholar]
- 98. Gordon P., LeGrand S. B., and Walsh D., “Nausea and Vomiting in Advanced Cancer,” European Journal of Pharmacology 722 (2014): 187–191: Epub 20131105, 10.1016/j.ejphar.2013.10.010. [DOI] [PubMed] [Google Scholar]
- 99. Navari R. M., “Nausea and Vomiting in Advanced Cancer,” Current Treatment Options in Oncology 21, no. 2 (2020): 14: Epub 20200205, 10.1007/s11864-020-0704-8. [DOI] [PubMed] [Google Scholar]
- 100. Razvi Y., Chan S., McFarlane T., et al., “ASCO, NCCN, MASCC/ESMO: A Comparison of Antiemetic Guidelines for the Treatment of Chemotherapy‐Induced Nausea and Vomiting in Adult Patients,” Supportive Care in Cancer 27, no. 1 (2019): 87–95: Epub 20181003, 10.1007/s00520-018-4464-y. [DOI] [PubMed] [Google Scholar]
- 101. Rhodes V. A. and McDaniel R. W., “Nausea, Vomiting, and Retching: Complex Problems in Palliative Care,” CA: A Cancer Journal for Clinicians 51, no. 4 (2001): 232–248: ; quiz 49‐52., 10.3322/canjclin.51.4.232. [DOI] [PubMed] [Google Scholar]
- 102. Webb A., “Management of Nausea and Vomiting in Patients With Advanced Cancer at the End of Life,” Nursing Standard 32, no. 10 (2017): 53–63, 10.7748/ns.2017.e10993. [DOI] [PubMed] [Google Scholar]
- 103. Roscoe J. A., Morrow G. R., Aapro M. S., Molassiotis A., and Olver I., “Anticipatory Nausea and Vomiting,” Supportive Care in Cancer 19, no. 10 (2011): 1533–1538: Epub 20100830, 10.1007/s00520-010-0980-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 104. Henson L. A., Maddocks M., Evans C., Davidson M., Hicks S., and Higginson I. J., “Palliative Care and the Management of Common Distressing Symptoms in Advanced Cancer: Pain, Breathlessness, Nausea and Vomiting, and Fatigue,” Journal of Clinical Oncology 38, no. 9 (2020): 905–914: Epub 20200205, 10.1200/jco.19.00470. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 105. Wienbeck M. and Berges W., “Esophageal Disorders in the Etiology and Pathophysiology of Dyspepsia,” Scandinavian Journal of Gastroenterology ‐ Supplement 109, no. sup109 (1985): 133–143, 10.3109/00365528509103947. [DOI] [PubMed] [Google Scholar]
- 106. Jehangir A., Tanner S., Malik Z., and Parkman H. P., “Characterizing the Proximal Esophageal Segment in Patients With Symptoms of Esophageal Dysmotility,” Neuro‐Gastroenterology and Motility 32, no. 9 (2020): e13888: Epub 20200602, 10.1111/nmo.13888. [DOI] [PubMed] [Google Scholar]
- 107. Handa M., Mine K., Yamamoto H., et al., “Esophageal Motility and Psychiatric Factors in Functional Dyspepsia Patients With or Without Pain,” Digestive Diseases and Sciences 44, no. 10 (1999): 2094–2098, 10.1023/a:1026690806330. [DOI] [PubMed] [Google Scholar]
- 108. Triadafilopoulos G., Nguyen L., and Clarke J. O., “Patients With Symptoms of Delayed Gastric Emptying Have a High Prevalence of Oesophageal Dysmotility, Irrespective of Scintigraphic Evidence of Gastroparesis,” BMJ Open Gastroenterol 4, no. 1 (2017): e000169: Epub 20170914, 10.1136/bmjgast-2017-000169. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 109. Latrache S., Melchior C., Desprez C., et al., “Is it Necessary to Perform a Morphological Assessment for an Esophageal Motility Disorder? A Retrospective Descriptive Study,” Clin Res Hepatol Gastroenterol 45, no. 6 (2021): 101633: Epub 20210301, 10.1016/j.clinre.2021.101633. [DOI] [PubMed] [Google Scholar]
- 110. Roman S., Huot L., Zerbib F., et al., “High‐Resolution Manometry Improves the Diagnosis of Esophageal Motility Disorders in Patients With Dysphagia: A Randomized Multicenter Study,” American Journal of Gastroenterology 111, no. 3 (2016): 372–380: Epub 20160202, 10.1038/ajg.2016.1. [DOI] [PubMed] [Google Scholar]
- 111. Yadlapati R., Kahrilas P. J., Fox M. R., et al., “Esophageal Motility Disorders on High‐Resolution manometry: Chicago classification Version 4.0(©),” Neuro‐Gastroenterology and Motility 33, no. 1 (2021): e14058, 10.1111/nmo.14058. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 112. Boo H. S., Chik I., Ngiu C. S., Lim S. Y., and Jarmin R., “High Resolution Impedance Manometry: A Necessity or Luxury in Esophageal Motility Disorder?,” Am J Case Rep 19 (2018): 998–1003: Epub 20180823, 10.12659/ajcr.909717. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 113. Halland M., Pandolfino J., and Barba E., “Diagnosis and Treatment of Rumination Syndrome,” Clinical Gastroenterology and Hepatology 16, no. 10 (2018): 1549–1555: Epub 20180612, 10.1016/j.cgh.2018.05.049. [DOI] [PubMed] [Google Scholar]
- 114. Camilleri M., Chedid V., Ford A. C., et al., “Gastroparesis,” Nature Reviews Disease Primers 4, no. 1 (2018): 41, 10.1038/S41572-018-0038-Z. [DOI] [PubMed] [Google Scholar]
- 115. Lacy B. E., Tack J., and Gyawali C. P., “AGA Clinical Practice Update on Management of Medically Refractory Gastroparesis: Expert Review,” Clinical Gastroenterology and Hepatology: the official clinical practice journal of the American Gastroenterological Association 20, no. 3 (2022): 491–500, 10.1016/J.CGH.2021.10.038. [DOI] [PubMed] [Google Scholar]
- 116. Parkman H. P., Yates K., Hasler W. L., et al., “Similarities and Differences Between Diabetic and Idiopathic Gastroparesis,” Clinical Gastroenterology and Hepatology: the official clinical practice journal of the American Gastroenterological Association 9, no. 12 (2011): 1056–1064, 10.1016/J.CGH.2011.08.013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 117. Parkman H. P., Hasler W. L., and Fisher R. S., “AGA Technical Review on the Diagnosis and Treatment of Gastroparesis,” Gastroenterology 127, no. 5 (2004): 1592–1622, 10.1053/j.gastro.2004.09.055. [DOI] [PubMed] [Google Scholar]
- 118. Soykan I., Sivri B., Sarosiek I., Kiernan B., and McCallum R. W., “Demography, Clinical Characteristics, Psychological and Abuse Profiles, Treatment, and Long‐Term Follow‐Up of Patients With Gastroparesis,” Digestive Diseases and Sciences 43, no. 11 (1998): 2398–2404, 10.1023/A:1026665728213. [DOI] [PubMed] [Google Scholar]
- 119. Nguyen L. A. and Snape W. J., “Clinical Presentation and Pathophysiology of Gastroparesis,” Gastroenterology Clinics of North America 44, no. 1 (2015): 21–30, 10.1016/J.GTC.2014.11.003. [DOI] [PubMed] [Google Scholar]
- 120. Parkman H. P., Wilson L. A., Hasler W. L., et al., “Abdominal Pain in Patients With Gastroparesis: Associations With Gastroparesis Symptoms, Etiology of Gastroparesis, Gastric Emptying, Somatization, and Quality of Life,” Digestive Diseases and Sciences 64, no. 8 (2019): 2242–2255, 10.1007/S10620-019-05522-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 121. Hasler W. L., Wilson L. A., Parkman H. P., et al., “Factors Related to Abdominal Pain in Gastroparesis: Contrast to Patients With Predominant Nausea and Vomiting,” Neuro‐Gastroenterology and Motility: the official journal of the European Gastrointestinal Motility Society 25, no. 5 (2013): 427, 10.1111/NMO.12091. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 122. Croosu S. S., Hansen T. M., Brock B., Mohr Drewes A., Brock C., and Frøkjær J. B., “Altered Functional Connectivity Between Brain Structures in Adults With Type 1 Diabetes and Polyneuropathy,” Brain Research 1784 (2022): 147882, 10.1016/J.BRAINRES.2022.147882. [DOI] [PubMed] [Google Scholar]
- 123. Parkman H. P. and Schwartz S. S., “Esophagitis and Gastroduodenal Disorders Associated With Diabetic Gastroparesis,” Archives of Internal Medicine 147, no. 8 (1987): 1477–1480, 10.1001/ARCHINTE.1987.00370080113021. [DOI] [PubMed] [Google Scholar]
- 124. Snodgrass P., Sandoval H., Calhoun V. D., et al., “Central Nervous System Mechanisms of Nausea in Gastroparesis: An fMRI‐Based Case‐Control Study,” Digestive Diseases and Sciences 65, no. 2 (2020): 551–556, 10.1007/S10620-019-05766-5. [DOI] [PubMed] [Google Scholar]
- 125. Cogliandro R. F., Rizzoli G., Bellacosa L., et al., “Is Gastroparesis a Gastric Disease?,” Neuro‐Gastroenterology and Motility 31, no. 5 (2019): e13562: Epub 20190217, 10.1111/nmo.13562. [DOI] [PubMed] [Google Scholar]
- 126. Mark E. B., Nedergaard R. B., Hansen T. M., et al., “Tapentadol Results in Less Deterioration of Gastrointestinal Function and Symptoms Than Standard Opioid Therapy in Healthy Male Volunteers,” Neuro‐Gastroenterology and Motility: the official journal of the European Gastrointestinal Motility Society 33, no. 11 (2021), 10.1111/NMO.14131. [DOI] [PubMed] [Google Scholar]
- 127. Olesen A. E., Gronlund D., Mark E. B., Krogh K., Frokjar J. B., and Drewes A. M., “Effects of Naloxegol on Gastrointestinal Transit and Colonic Fecal Volume in Healthy Participants Receiving Oxycodone,” Journal of neurogastroenterology and motility 25, no. 4 (2019): 602–610, 10.5056/JNM18079. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 128. Poulsen J. L., Mark E. B., Brock C., Frøkjær J. B., Krogh K., and Drewes A. M., “Colorectal Transit and Volume During Treatment With Prolonged‐Release Oxycodone/Naloxone Versus Oxycodone Plus Macrogol 3350,” Journal of neurogastroenterology and motility 24, no. 1 (2018): 119–127, 10.5056/JNM17058. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 129. Drewes A. M., Olesen A. E., Farmer A. D., Szigethy E., Rebours V., and Olesen S. S., “Gastrointestinal Pain,” Nature Reviews Disease Primers 6, no. 1 (2020): 1, 10.1038/s41572-019-0135-7. [DOI] [PubMed] [Google Scholar]
- 130. Hoogerwerf W. A., Pasricha P. J., Kalloo A. N., and Schuster M. M., “Pain: The Overlooked Symptom in Gastroparesis,” American Journal of Gastroenterology 94, no. 4 (1999): 1029–1033, 10.1111/J.1572-0241.1999.01008.X. [DOI] [PubMed] [Google Scholar]
- 131. Bills S., Shine A., Williams J. C., et al., “Difference in Cyclic versus Non‐cyclic Symptom Patterns in Patients With the Symptoms of Gastroparesis Undergoing Bioelectric Therapy,” Digestive Diseases and Sciences 69, no. 5 (2024): 1722–1730: Epub 20240409, 10.1007/s10620-024-08303-1. [DOI] [PubMed] [Google Scholar]
- 132. Christensen C. J., Johnson W. D., and Abell T. L., “Patients With Cyclic Vomiting Pattern and Diabetic Gastropathy Have More Migraines, Abnormal Electrogastrograms, and Gastric Emptying,” Scandinavian Journal of Gastroenterology 43, no. 9 (2008): 1076–1081, 10.1080/00365520802085411. [DOI] [PubMed] [Google Scholar]
- 133. Schol J., Wauters L., Dickman R., et al., “United European Gastroenterology (UEG) and European Society for Neurogastroenterology and Motility (ESNM) Consensus on Gastroparesis,” United European Gastroenterol J 9, no. 3 (2021): 287–306, 10.1002/ueg2.12060. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 134. Haans J. J. L. and Masclee A. A. M., “Review Article: The Diagnosis and Management of Gastroparesis,” Alimentary Pharmacology and Therapeutics 26, no. Suppl 2 (2007): 37–46: (SUPPL. 2), 10.1111/J.1365-2036.2007.03534.X. [DOI] [PubMed] [Google Scholar]
- 135. Keller J., Bassotti G., Clarke J., et al., “Expert Consensus Document: Advances in the Diagnosis and Classification of Gastric and Intestinal Motility Disorders,” Nature Reviews Gastroenterology & Hepatology 15, no. 5 (2018): 291–308, 10.1038/NRGASTRO.2018.7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 136. Cangemi D. J. and Lacy B. E., “Gastroparesis,” Current Opinion in Gastroenterology 37, no. 6 (2021): 596–601, 10.1097/MOG.0000000000000782. [DOI] [PubMed] [Google Scholar]
- 137. Vijayvargiya P., Jameie‐Oskooei S., Camilleri M., Chedid V., Erwin P. J., and Murad M. H., “Association Between Delayed Gastric Emptying and Upper Gastrointestinal Symptoms: A Systematic Review and Meta‐Analysis,” Gut 68, no. 5 (2019): 804–813: Epub 20180602, 10.1136/gutjnl-2018-316405. [DOI] [PubMed] [Google Scholar]
- 138. Brinck C. E., Mark E. B., Klinge M. W., et al., “Magnetic Tracking of Gastrointestinal Motility,” Physiological Measurement 41, no. 12 (2020): 12TR01, 10.1088/1361-6579/ABCD1E. [DOI] [PubMed] [Google Scholar]
- 139. Khalaf A., Hoad C. L., Menys A., et al., “MRI Assessment of the Postprandial Gastrointestinal Motility and Peptide Response in Healthy Humans,” Neuro‐Gastroenterology and Motility: the official journal of the European Gastrointestinal Motility Society 30, no. 1 (2018): e13182, 10.1111/nmo.13182. [DOI] [PubMed] [Google Scholar]
- 140. Wegeberg A. M. L., Brock C., Ejskjaer N., et al., “Gastrointestinal Symptoms and Cardiac Vagal Tone in Type 1 Diabetes Correlates With Gut Transit Times and Motility Index,” Neuro‐Gastroenterology and Motility: the official journal of the European Gastrointestinal Motility Society 33, no. 1 (2021), 10.1111/NMO.13885. [DOI] [PubMed] [Google Scholar]
- 141. Wuestenberghs F., Juge M., Melchior C., Desprez C., Leroi A. M., and Gourcerol G., “Association Between Symptoms, Quality of Life, and Gastric Emptying in Dyspeptic Patients,” J Neurogastroenterol Motil 25, no. 4 (2019): 534–543, 10.5056/jnm19060. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 142. Pasricha P. J., Colvin R., Yates K., et al., “Characteristics of Patients With Chronic Unexplained Nausea and Vomiting and Normal Gastric Emptying,” Clinical Gastroenterology and Hepatology 9, no. 7 (2011): 567–576: e1‐4. Epub 20110311, 10.1016/j.cgh.2011.03.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 143. Karamanolis G., Caenepeel P., Arts J., and Tack J., “Association of the Predominant Symptom With Clinical Characteristics and Pathophysiological Mechanisms in Functional Dyspepsia,” Gastroenterology 130, no. 2 (2006): 296–303, 10.1053/j.gastro.2005.10.019. [DOI] [PubMed] [Google Scholar]
- 144. Talley N. J., G. R. Locke, 3rd , Lahr B. D., et al., “Functional Dyspepsia, Delayed Gastric Emptying, and Impaired Quality of Life,” Gut 55, no. 7 (2006): 933–939: Epub 20051201, 10.1136/gut.2005.078634. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 145. Kindt S., Dubois D., Van Oudenhove L., et al., “Relationship Between Symptom Pattern, Assessed by the PAGI‐SYM Questionnaire, and Gastric Sensorimotor Dysfunction in Functional Dyspepsia,” Neuro‐Gastroenterology and Motility 21, no. 11 (2009): 1183: ‐e105. Epub 20090804, 10.1111/j.1365-2982.2009.01374.x. [DOI] [PubMed] [Google Scholar]
- 146. Sarnelli G., Caenepeel P., Geypens B., Janssens J., and Tack J., “Symptoms Associated With Impaired Gastric Emptying of Solids and Liquids in Functional Dyspepsia,” American Journal of Gastroenterology 98, no. 4 (2003): 783–788, 10.1111/j.1572-0241.2003.07389.x. [DOI] [PubMed] [Google Scholar]
- 147. Vanheel H., Carbone F., Valvekens L., et al., “Pathophysiological Abnormalities in Functional Dyspepsia Subgroups According to the Rome III Criteria,” American Journal of Gastroenterology 112, no. 1 (2017): 132–140: Epub 20161213, 10.1038/ajg.2016.499. [DOI] [PubMed] [Google Scholar]
- 148. Chedid V., Brandler J., Vijayvargiya P., Park S. Y., Szarka L. A., and Camilleri M., “Characterization of Upper Gastrointestinal Symptoms, Gastric Motor Functions, and Associations in Patients With Diabetes at a Referral Center,” American Journal of Gastroenterology 114, no. 1 (2019): 143–154, 10.1038/s41395-018-0234-1. [DOI] [PubMed] [Google Scholar]
- 149. Park S. Y., Acosta A., Camilleri M., et al., “Gastric Motor Dysfunction in Patients With Functional Gastroduodenal Symptoms,” American Journal of Gastroenterology 112, no. 11 (2017): 1689–1699: Epub 20170912, 10.1038/ajg.2017.264. [DOI] [PubMed] [Google Scholar]
- 150. Parkman H. P., Yates K., Hasler W. L., et al., “Clinical Features of Idiopathic Gastroparesis Vary With Sex, Body Mass, Symptom Onset, Delay in Gastric Emptying, and Gastroparesis Severity,” Gastroenterology 140, no. 1 (2011): 101–115: Epub 20101020, 10.1053/j.gastro.2010.10.015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 151. Ducrotte P., Coffin B., Bonaz B., et al., “Gastric Electrical Stimulation Reduces Refractory Vomiting in a Randomized Crossover Trial,” Gastroenterology 158, no. 3 (2020): 506–514.e2: Epub 20191021, 10.1053/j.gastro.2019.10.018. [DOI] [PubMed] [Google Scholar]
- 152. Camilleri M., McCallum R. W., Tack J., Spence S. C., Gottesdiener K., and Fiedorek F. T., “Efficacy and Safety of Relamorelin in Diabetics With Symptoms of Gastroparesis: A Randomized, Placebo‐Controlled Study,” Gastroenterology 153, no. 5 (2017): 1240–1250.e2: Epub 20170729, 10.1053/j.gastro.2017.07.035. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 153. Carbone F., Van den Houte K., Clevers E., et al., “Prucalopride in Gastroparesis: A Randomized Placebo‐Controlled Crossover Study,” American Journal of Gastroenterology 114, no. 8 (2019): 1265–1274, 10.14309/ajg.0000000000000304. [DOI] [PubMed] [Google Scholar]
- 154. Tack J., Goelen N., Carbone F., et al., “Prokinetic Effects and Symptom Relief in the Pharmacotherapy of Gastroparesis,” Gastroenterology 158, no. 6 (2020): 1841–1842: Epub 20200218, 10.1053/j.gastro.2019.06.049. [DOI] [PubMed] [Google Scholar]
- 155. Camilleri M., Kuo B., Nguyen L., et al., “ACG Clinical Guideline: Gastroparesis,” American Journal of Gastroenterology 117, no. 8 (2022): 1197–1220: Epub 20220603, 10.14309/ajg.0000000000001874. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 156. Abell T. L., Camilleri M., Donohoe K., et al., “Consensus Recommendations for Gastric Emptying Scintigraphy: A Joint Report of the American Neurogastroenterology and Motility Society and the Society of Nuclear Medicine,” American Journal of Gastroenterology 103, no. 3 (2008): 753–763: Epub 20071119, 10.1111/j.1572-0241.2007.01636.x. [DOI] [PubMed] [Google Scholar]
- 157. Ye Y., Yin Y., Huh S. Y., Almansa C., Bennett D., and Camilleri M., “Epidemiology, Etiology, and Treatment of Gastroparesis: Real‐World Evidence From a Large US National Claims Database,” Gastroenterology 162, no. 1 (2022): 109–121.e5: Epub 20211006, 10.1053/j.gastro.2021.09.064. [DOI] [PubMed] [Google Scholar]
- 158. Gourcerol G., Tissier F., Melchior C., et al., “Impaired Fasting Pyloric Compliance in Gastroparesis and the Therapeutic Response to Pyloric Dilatation,” Alimentary Pharmacology & Therapeutics 41, no. 4 (2015): 360–367: Epub 20141219, 10.1111/apt.13053. [DOI] [PubMed] [Google Scholar]
- 159. Snape W. J., Lin M. S., Agarwal N., and Shaw R. E., “Evaluation of the Pylorus With Concurrent Intraluminal Pressure and EndoFLIP in Patients With Nausea and Vomiting,” Neuro‐Gastroenterology and Motility 28, no. 5 (2016): 758–764: Epub 20160127, 10.1111/nmo.12772. [DOI] [PubMed] [Google Scholar]
- 160. Malik Z., Sankineni A., and Parkman H. P., “Assessing Pyloric Sphincter Pathophysiology Using EndoFLIP in Patients With Gastroparesis,” Neuro‐Gastroenterology and Motility 27, no. 4 (2015): 524–531: Epub 20150224, 10.1111/nmo.12522. [DOI] [PubMed] [Google Scholar]
- 161. Desprez C., Melchior C., Wuestenberghs F., et al., “Pyloric Distensibility Measurement Predicts Symptomatic Response to Intrapyloric Botulinum Toxin Injection,” Gastrointestinal Endoscopy 90, no. 5 (2019): 754–760.e1: Epub 20190425, 10.1016/j.gie.2019.04.228. [DOI] [PubMed] [Google Scholar]
- 162. Jacques J., Pagnon L., Hure F., et al., “Peroral Endoscopic Pyloromyotomy Is Efficacious and Safe for Refractory Gastroparesis: Prospective Trial With Assessment of Pyloric Function,” Endoscopy 51, no. 1 (2019): 40–49: Epub 20180612, 10.1055/a-0628-6639. [DOI] [PubMed] [Google Scholar]
- 163. Vosoughi K., Ichkhanian Y., Jacques J., et al., “Role of Endoscopic Functional Luminal Imaging Probe in Predicting the Outcome of Gastric Peroral Endoscopic Pyloromyotomy (With Video),” Gastrointestinal Endoscopy 91, no. 6 (2020): 1289–1299: Epub 20200206, 10.1016/j.gie.2020.01.044. [DOI] [PubMed] [Google Scholar]
- 164. Tack J., Piessevaux H., Coulie B., Caenepeel P., and Janssens J., “Role of Impaired Gastric Accommodation to a Meal in Functional Dyspepsia,” Gastroenterology 115, no. 6 (1998): 1346–1352, 10.1016/s0016-5085(98)70012-5. [DOI] [PubMed] [Google Scholar]
- 165. Rhee P. L., Kim Y. H., Son H. J., et al., “Evaluation of Individual Symptoms Cannot Predict Presence of Gastric Hypersensitivity in Functional Dyspepsia,” Digestive Diseases and Sciences 45, no. 8 (2000): 1680–1684, 10.1023/a:1005550019308. [DOI] [PubMed] [Google Scholar]
- 166. Castro A., Mearin F., Larish J., and Malagelada J. R., “Gastric Fundus Relaxation and Emetic Sequences Induced by Apomorphine and Intragastric Lipid Infusion in Healthy Humans,” American Journal of Gastroenterology 95, no. 12 (2000): 3404–3411, 10.1111/j.1572-0241.2000.03352.x. [DOI] [PubMed] [Google Scholar]
- 167. Schaub N., Ng K., Kuo P., Aziz Q., and Sifrim D., “Gastric and Lower Esophageal Sphincter Pressures During Nausea: A Study Using Visual Motion‐Induced Nausea and High‐Resolution Manometry,” American Journal of Physiology ‐ Gastrointestinal and Liver Physiology 306, no. 9 (2014): G741–G747: Epub 20140313, 10.1152/ajpgi.00412.2013. [DOI] [PubMed] [Google Scholar]
- 168. Tack J., Caenepeel P., Fischler B., Piessevaux H., and Janssens J., “Symptoms Associated With Hypersensitivity to Gastric Distention in Functional Dyspepsia,” Gastroenterology 121, no. 3 (2001): 526–535, 10.1053/gast.2001.27180. [DOI] [PubMed] [Google Scholar]
- 169. Camilleri M., Bharucha A. E., di Lorenzo C., et al., “American Neurogastroenterology and Motility Society Consensus Statement on Intraluminal Measurement of Gastrointestinal and Colonic Motility in Clinical Practice,” Neuro‐Gastroenterology and Motility 20, no. 12 (2008): 1269–1282, 10.1111/j.1365-2982.2008.01230.x. [DOI] [PubMed] [Google Scholar]
- 170. Stanghellini V. and Tack J., “Gastroparesis: Separate Entity or Just a Part of Dyspepsia?,” Gut 63, no. 12 (2014): 1972–1978: Epub 20140926, 10.1136/gutjnl-2013-306084. [DOI] [PubMed] [Google Scholar]
- 171. Vanheel H., Vanuytsel T., Van Oudenhove L., Farré R., Verbeke K., and Tack J., “Postprandial Symptoms Originating From the Stomach in Functional Dyspepsia,” Neuro‐Gastroenterology and Motility 25, no. 11 (2013): 911‐e703: Epub 20130902, 10.1111/nmo.12227. [DOI] [PubMed] [Google Scholar]
- 172. Bekkelund M., Sangnes D. A., Søfteland E., et al., “Gastroparesis Symptoms Associated With Intestinal Hypomotility: An Explorative Study Using Wireless Motility Capsule,” Clinical and Experimental Gastroenterology 14 (2021): 133–144: Epub 20210428, 10.2147/ceg.S304854. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 173. Kolar G. J., Camilleri M., Burton D., Nadeau A., and Zinsmeister A. R., “Prevalence of Colonic Motor or Evacuation Disorders in Patients Presenting With Chronic Nausea and Vomiting Evaluated by a Single Gastroenterologist in a Tertiary Referral Practice,” Neuro‐Gastroenterology and Motility 26, no. 1 (2014): 131–138: Epub 20131010, 10.1111/nmo.12242. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 174. Ang D., Pannemans J., Vanuytsel T., and Tack J., “A Single‐Center Audit of the Indications and Clinical Impact of Prolonged Ambulatory Small Intestinal Manometry,” Neuro‐Gastroenterology and Motility 30, no. 9 (2018): e13357: Epub 20180501, 10.1111/nmo.13357. [DOI] [PubMed] [Google Scholar]
- 175. Cogliandro R. F., Antonucci A., De Giorgio R., et al., “Patient‐reported Outcomes and Gut Dysmotility in Functional Gastrointestinal Disorders,” Neuro‐Gastroenterology and Motility 23, no. 12 (2011): 1084–1091: Epub 20110914, 10.1111/j.1365-2982.2011.01783.x. [DOI] [PubMed] [Google Scholar]
- 176. Rosa E. S. L., Gerson L., Davila M., and Triadafilopoulos G., “Clinical, Radiologic, and Manometric Characteristics of Chronic Intestinal Dysmotility: The Stanford Experience,” Clinical Gastroenterology and Hepatology 4, no. 7 (2006): 866–873: Epub 20060622, 10.1016/j.cgh.2006.05.001. [DOI] [PubMed] [Google Scholar]
- 177. Lindberg G., Iwarzon M., and Tornblom H., “Clinical Features and Long‐Term Survival in Chronic Intestinal Pseudo‐obstruction and Enteric Dysmotility,” Scandinavian Journal of Gastroenterology 44, no. 6 (2009): 692–699, 10.1080/00365520902839642. [DOI] [PubMed] [Google Scholar]
- 178. Stanghellini V., Cogliandro R. F., De Giorgio R., et al., “Natural History of Chronic Idiopathic Intestinal Pseudo‐obstruction in Adults: A Single Center Study,” Clinical Gastroenterology and Hepatology 3, no. 5 (2005): 449–458, 10.1016/s1542-3565(04)00675-5. [DOI] [PubMed] [Google Scholar]
- 179. Levine M. S., “Role of the Double‐Contrast Upper Gastrointestinal Series in the 1990s,” Gastroenterology Clinics of North America 24, no. 2 (1995): 289–308, 10.1016/s0889-8553(21)00194-1. [DOI] [PubMed] [Google Scholar]
- 180. Shrake P. D., Rex D. K., Lappas J. C., and Maglinte D. D., “Radiographic Evaluation of Suspected Small Bowel Obstruction,” American Journal of Gastroenterology 86, no. 2 (1991): 175–178. [PubMed] [Google Scholar]
- 181. Donckier V., Closset J., Van Gansbeke D., et al., “Contribution of Computed Tomography to Decision Making in the Management of Adhesive Small Bowel Obstruction,” British Journal of Surgery 85, no. 8 (1998): 1071–1074, 10.1046/j.1365-2168.1998.00813.x. [DOI] [PubMed] [Google Scholar]
- 182. Peck J. J., Milleson T., and Phelan J., “The Role of Computed Tomography With Contrast and Small Bowel Follow‐Through in Management of Small Bowel Obstruction,” American Journal of Surgery 177, no. 5 (1999): 375–378, 10.1016/s0002-9610(99)00066-5. [DOI] [PubMed] [Google Scholar]
- 183. Suri S., Gupta S., Sudhakar P. J., Venkataramu N. K., Sood B., and Wig J. D., “Comparative Evaluation of Plain Films, Ultrasound and CT in the Diagnosis of Intestinal Obstruction,” Acta Radiologica 40, no. 4 (1999): 422–428, 10.3109/02841859909177758. [DOI] [PubMed] [Google Scholar]
- 184. Greydanus M. P., Camilleri M., Colemont L. J., Phillips S. F., Brown M. L., and Thomforde G. M., “Ileocolonic Transfer of Solid Chyme in Small Intestinal Neuropathies and Myopathies,” Gastroenterology 99, no. 1 (1990): 158–164, 10.1016/0016-5085(90)91243-y. [DOI] [PubMed] [Google Scholar]
- 185. Camilleri M., Zinsmeister A. R., Greydanus M. P., Brown M. L., and Proano M., “Towards a Less Costly but Accurate Test of Gastric Emptying and Small Bowel Transit,” Digestive Diseases and Sciences 36, no. 5 (1991): 609–615, 10.1007/bf01297027. [DOI] [PubMed] [Google Scholar]
- 186. Grybäck P., Jacobsson H., Blomquist L., Schnell P. O., and Hellström P. M., “Scintigraphy of the Small Intestine: A Simplified Standard for Study of Transit With Reference to Normal Values,” European Journal of Nuclear Medicine and Molecular Imaging 29, no. 1 (2002): 39–45: Epub 20011122, 10.1007/s00259-001-0687-z. [DOI] [PubMed] [Google Scholar]
- 187. Menys A., Butt S., Emmanuel A., et al., “Comparative Quantitative Assessment of Global Small Bowel Motility Using Magnetic Resonance Imaging in Chronic Intestinal Pseudo‐obstruction and Healthy Controls,” Neuro‐Gastroenterology and Motility 28, no. 3 (2016): 376–383: Epub 20151210, 10.1111/nmo.12735. [DOI] [PubMed] [Google Scholar]
- 188. Fuyuki A., Ohkubo H., Higurashi T., et al., “Clinical Importance of Cine‐MRI Assessment of Small Bowel Motility in Patients With Chronic Intestinal Pseudo‐obstruction: A Retrospective Study of 33 Patients,” Journal of Gastroenterology 52, no. 5 (2017): 577–584: Epub 20160822, 10.1007/s00535-016-1251-8. [DOI] [PubMed] [Google Scholar]
- 189. Ohkubo H., Kessoku T., Fuyuki A., et al., “Assessment of Small Bowel Motility in Patients With Chronic Intestinal Pseudo‐obstruction Using Cine‐MRI,” American Journal of Gastroenterology 108, no. 7 (2013): 1130–1139: Epub 20130319, 10.1038/ajg.2013.57. [DOI] [PubMed] [Google Scholar]
- 190. van Rijn K. L., Bredenoord A. J., Smout A., et al., “Fasted and Fed Small Bowel Motility Patterns at Cine‐MRI in Chronic Intestinal Pseudo‐obstruction,” Neuro‐Gastroenterology and Motility 33, no. 6 (2021): e14062: Epub 20201227, 10.1111/nmo.14062. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 191. Summers R. W., Anuras S., and Green J., “Jejunal Manometry Patterns in Health, Partial Intestinal Obstruction, and Pseudoobstruction,” Gastroenterology 85, no. 6 (1983): 1290–1300, 10.1016/s0016-5085(83)80009-2. [DOI] [PubMed] [Google Scholar]
- 192. Schuffler M. D., Rohrmann C. A., Chaffee R. G., Brand D. L., Delaney J. H., and Young J. H., “Chronic Intestinal Pseudo‐obstruction. A Report of 27 Cases and Review of the Literature,” Medicine (Baltimore) 60, no. 3 (1981): 173–196, 10.1097/00005792-198105000-00002. [DOI] [PubMed] [Google Scholar]
- 193. Makanjuola D., “Computed Tomography Compared With Small Bowel Enema in Clinically Equivocal Intestinal Obstruction,” Clinical Radiology 53, no. 3 (1998): 203–208, 10.1016/s0009-9260(98)80101-3. [DOI] [PubMed] [Google Scholar]
- 194. Malagelada C., De Iorio F., Azpiroz F., et al., “New Insight into Intestinal Motor Function via Noninvasive Endoluminal Image Analysis,” Gastroenterology 135, no. 4 (2008): 1155–1162: Epub 20080703, 10.1053/j.gastro.2008.06.084. [DOI] [PubMed] [Google Scholar]
- 195. Fleisher D. R., “The Cyclic Vomiting Syndrome Described,” Journal of Pediatric Gastroenterology and Nutrition 21, no. Suppl 1 (1995): S1–S5, 10.1097/00005176-199501001-00003. [DOI] [PubMed] [Google Scholar]
- 196. Fleisher D. R. and Matar M., “The Cyclic Vomiting Syndrome: A Report of 71 Cases and Literature Review,” Journal of Pediatric Gastroenterology and Nutrition 17, no. 4 (1993): 361–369, 10.1002/j.1536-4801.1993.tb10995.x. [DOI] [PubMed] [Google Scholar]
- 197. Abu‐Arafeh I. and Russell G., “Cyclical Vomiting Syndrome in Children: A Population‐Based Study,” Journal of Pediatric Gastroenterology and Nutrition 21, no. 4 (1995): 454–458, 10.1097/00005176-199511000-00014. [DOI] [PubMed] [Google Scholar]
- 198. Kaul A. and Kaul K. K., “Cyclic Vomiting Syndrome: A Functional Disorder,” Pediatr Gastroenterol Hepatol Nutr 18, no. 4 (2015): 224–229: Epub 20151223, 10.5223/pghn.2015.18.4.224. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 199. Forbes D., “Differential Diagnosis of Cyclic Vomiting Syndrome,” Journal of Pediatric Gastroenterology and Nutrition 21, no. Suppl 1 (1995): S11–S14, 10.1097/00005176-199501001-00005. [DOI] [PubMed] [Google Scholar]
- 200. Li B. U., Murray R. D., Heitlinger L. A., Robbins J. L., and Hayes J. R., “Heterogeneity of Diagnoses Presenting as Cyclic Vomiting,” Pediatrics 102, no. 3 Pt 1 (1998): 583–587, 10.1542/peds.102.3.583. [DOI] [PubMed] [Google Scholar]
- 201. Proceedings of the 2nd International Scientific Symposium on Cyclic Vomiting Syndrome. Milwaukee, Wisconsin, USA. April 17‐18, 1998.” Digestive Diseases and Sciences 44, no. 8 Suppl (1999): 1s–119s. [PubMed] [Google Scholar]
- 202. Li B. U., “Cyclic Vomiting: The Pattern and Syndrome Paradigm,” Journal of Pediatric Gastroenterology and Nutrition 21, no. Suppl 1 (1995): S6–S10, 10.1097/00005176-199501001-00004. [DOI] [PubMed] [Google Scholar]
- 203. Pfau B. T., Li B. U., Murray R. D., Heitlinger L. A., McClung H. J., and Hayes J. R., “Differentiating Cyclic From Chronic Vomiting Patterns in Children: Quantitative Criteria and Diagnostic Implications,” Pediatrics 97, no. 3 (1996): 364–368, 10.1542/peds.97.3.364. [DOI] [PubMed] [Google Scholar]
- 204. Fitzpatrick E., Bourke B., Drumm B., and Rowland M., “The Incidence of Cyclic Vomiting Syndrome in Children: Population‐Based Study,” American Journal of Gastroenterology 103, no. 4 (2008): 991–995: quiz 6. Epub 20071205, 10.1111/j.1572-0241.2007.01668.x. [DOI] [PubMed] [Google Scholar]
- 205. Li B. U., Lefevre F., Chelimsky G. G., et al., “North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition Consensus Statement on the Diagnosis and Management of Cyclic Vomiting Syndrome,” Journal of Pediatric Gastroenterology and Nutrition 47, no. 3 (2008): 379–393, 10.1097/MPG.0b013e318173ed39. [DOI] [PubMed] [Google Scholar]
- 206. Prakash C. and Clouse R. E., “Cyclic Vomiting Syndrome in Adults: Clinical Features and Response to Tricyclic Antidepressants,” American Journal of Gastroenterology 94, no. 10 (1999): 2855–2860, 10.1111/j.1572-0241.1999.01428.x. [DOI] [PubMed] [Google Scholar]
- 207. Lee L. Y., Abbott L., Moodie S., and Anderson S., “Cyclic Vomiting Syndrome in 28 Patients: Demographics, Features and Outcomes,” European Journal of Gastroenterology and Hepatology 24, no. 8 (2012): 939–943, 10.1097/MEG.0b013e328354fc83. [DOI] [PubMed] [Google Scholar]
- 208. Prakash C., Staiano A., Rothbaum R. J., and Clouse R. E., “Similarities in Cyclic Vomiting Syndrome Across Age Groups,” American Journal of Gastroenterology 96, no. 3 (2001): 684–688, 10.1111/j.1572-0241.2001.03606.x. [DOI] [PubMed] [Google Scholar]
- 209. Li B. U. and Misiewicz L., “Cyclic Vomiting Syndrome: A Brain‐Gut Disorder,” Gastroenterology Clinics of North America 32, no. 3 (2003): 997–1019, 10.1016/s0889-8553(03)00045-1. [DOI] [PubMed] [Google Scholar]
- 210. Kumar N., Bashar Q., Reddy N., et al., “Cyclic Vomiting Syndrome (CVS): Is There a Difference Based on Onset of Symptoms‐‐Pediatric versus Adult?,” BMC Gastroenterology 12, no. 1 (2012): 52: Epub 20120528, 10.1186/1471-230x-12-52. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 211. Kovacic K., Sood M., and Venkatesan T., “Cyclic Vomiting Syndrome in Children and Adults: What Is New in 2018?,” Current Gastroenterology Reports 20, no. 10 (2018): 46: Epub 20180829, 10.1007/s11894-018-0654-5. [DOI] [PubMed] [Google Scholar]
- 212. Li B. U., “Cyclic Vomiting Syndrome: Light Emerging From the Black Box,” Journal of Pediatrics 135, no. 3 (1999): 276–277, 10.1016/s0022-3476(99)70119-8. [DOI] [PubMed] [Google Scholar]
- 213. Fleisher D. R., Gornowicz B., Adams K., Burch R., and Feldman E. J., “Cyclic Vomiting Syndrome in 41 Adults: The Illness, the Patients, and Problems of Management,” BMC Medicine 3, no. 1 (2005): 20: Epub 20051221, 10.1186/1741-7015-3-20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 214. Venkatesan T., Sengupta J., Lodhi A., et al., “An Internet Survey of Marijuana and Hot Shower Use in Adults With Cyclic Vomiting Syndrome (CVS),” Experimental Brain Research 232, no. 8 (2014): 2563–2570: Epub 20140504, 10.1007/s00221-014-3967-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 215. Li B. U., “Cyclic Vomiting Syndrome: Age‐Old Syndrome and New Insights,” Seminars in Pediatric Neurology 8, no. 1 (2001): 13–21, 10.1053/spen.2001.23456. [DOI] [PubMed] [Google Scholar]
- 216. Withers G. D., Silburn S. R., and Forbes D. A., “Precipitants and Aetiology of Cyclic Vomiting Syndrome,” Acta Paediatrica 87, no. 3 (1998): 272–277, 10.1080/08035259850157318. [DOI] [PubMed] [Google Scholar]
- 217. Forbes D. and Fairbrother S., “Cyclic Nausea and Vomiting in Childhood,” Australian Family Physician 37, no. 1‐2 (2008): 33–36. [PubMed] [Google Scholar]
- 218. Hasler W. L., Levinthal D. J., Tarbell S. E., et al., “Cyclic Vomiting Syndrome: Pathophysiology, Comorbidities, and Future Research Directions,” Neuro‐Gastroenterology and Motility 31, no. Suppl 2 (2019): e13607: (Suppl 2), 10.1111/nmo.13607. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 219. Zaki E. A., Freilinger T., Klopstock T., et al., “Two Common Mitochondrial DNA Polymorphisms Are Highly Associated With Migraine Headache and Cyclic Vomiting Syndrome,” Cephalalgia 29, no. 7 (2009): 719–728: Epub 20090210, 10.1111/j.1468-2982.2008.01793.x. [DOI] [PubMed] [Google Scholar]
- 220. Bhandari S. and Venkatesan T., “Clinical Characteristics, Comorbidities and Hospital Outcomes in Hospitalizations With Cyclic Vomiting Syndrome: A Nationwide Analysis,” Digestive Diseases and Sciences 62, no. 8 (2017): 2035–2044: Epub 20170103, 10.1007/s10620-016-4432-7. [DOI] [PubMed] [Google Scholar]
- 221. Abell T. L., Adams K. A., Boles R. G., et al., “Cyclic Vomiting Syndrome in Adults,” Neuro‐Gastroenterology and Motility 20, no. 4 (2008): 269–284, 10.1111/j.1365-2982.2008.01113.x. [DOI] [PubMed] [Google Scholar]
- 222. Thurler A. H. and Kuo B., “From Heave to Leave: Understanding Cyclic Vomiting Syndrome,” Gastroenterology Nursing 36, no. 6 (2013): 407–413, 10.1097/sga.0000000000000013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 223. Hayes W. J., VanGilder D., Berendse J., Lemon M. D., and Kappes J. A., “Cyclic Vomiting Syndrome: Diagnostic Approach and Current Management Strategies,” Clinical and Experimental Gastroenterology 11 (2018): 77–84: Epub 20180226, 10.2147/ceg.S136420. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 224. Popa S. L., Chiarioni G., David L., Golea G. I., and Dumitrascu D. L., “Functional Emesis,” J Gastrointestin Liver Dis 28, no. 3 (2019): 319–325: Epub 20190901, 10.15403/jgld-236. [DOI] [PubMed] [Google Scholar]
- 225. Frazier R. and Venkatesan T., “Current Understanding of the Etiology of Cyclic Vomiting Syndrome and Therapeutic Strategies in its Management,” Expert Review of Clinical Pharmacology 15, no. 11 (2022): 1305–1316: Epub 20221104, 10.1080/17512433.2022.2138341. [DOI] [PubMed] [Google Scholar]
- 226. Namin F., Patel J., Lin Z., et al., “Clinical, Psychiatric and Manometric Profile of Cyclic Vomiting Syndrome in Adults and Response to Tricyclic Therapy,” Neuro‐Gastroenterology and Motility 19, no. 3 (2007): 196–202, 10.1111/j.1365-2982.2006.00867.x. [DOI] [PubMed] [Google Scholar]
- 227. Thavamani A., Umapathi K. K., Khatana J., Bhandari S., Kovacic K., and Venkatesan T., “Cyclic Vomiting Syndrome‐Related Hospitalizations Trends, Comorbidities & Health Care Costs in Children: A Population Based Study,” Children 9, no. 1 (2022): 55: Epub 20220103, 10.3390/children9010055. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 228. Hejazi R. A., Lavenbarg T. H., and McCallum R. W., “Spectrum of Gastric Emptying Patterns in Adult Patients With Cyclic Vomiting Syndrome,” Neuro‐Gastroenterology and Motility 22, no. 12 (2010): 1298–1302: e338. Epub 20100819, 10.1111/j.1365-2982.2010.01584.x. [DOI] [PubMed] [Google Scholar]
- 229. Boles R. G., Zaki E. A., Lavenbarg T., et al., “Are Pediatric and Adult‐Onset Cyclic Vomiting Syndrome (CVS) Biologically Different Conditions? Relationship of Adult‐Onset CVS With the Migraine and Pediatric CVS‐Associated Common mtDNA Polymorphisms 16519T and 3010A,” Neuro‐Gastroenterology and Motility 21, no. 9 (2009): 936‐e72: Epub 20090408, 10.1111/j.1365-2982.2009.01305.x. [DOI] [PubMed] [Google Scholar]
- 230. Hejazi R. A., Lavenbarg T. H., Pasnoor M., et al., “Autonomic Nerve Function in Adult Patients With Cyclic Vomiting Syndrome,” Neuro‐Gastroenterology and Motility 23, no. 5 (2011): 439–443: Epub 20110216, 10.1111/j.1365-2982.2011.01679.x. [DOI] [PubMed] [Google Scholar]
- 231. Hejazi R. A., Lavenbarg T. H., and McCallum R. W., “Elevated Serum Ghrelin Levels in Adult Patients With Cyclic Vomiting Syndrome,” American Journal of Gastroenterology 106, no. 10 (2011): 1858–1859, 10.1038/ajg.2011.181. [DOI] [PubMed] [Google Scholar]
- 232. Venkatesan T., Zadvornova Y., Raff H., and Hillard C. J., “Endocannabinoid‐related Lipids Are Increased During an Episode of Cyclic Vomiting Syndrome,” Neuro‐Gastroenterology and Motility 28, no. 9 (2016): 1409–1418: Epub 20160420, 10.1111/nmo.12843. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 233. Pattathan M. B., Hejazi R. A., and McCallum R. W., “Association of Marijuana Use and Cyclic Vomiting Syndrome,” Pharmaceuticals 5, no. 7 (2012): 719–726: Epub 20120629, 10.3390/ph5070719. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 234. Bashashati M. and McCallum R. W., “Neurochemical Mechanisms and Pharmacologic Strategies in Managing Nausea and Vomiting Related to Cyclic Vomiting Syndrome and Other Gastrointestinal Disorders,” European Journal of Pharmacology 722 (2014): 79–94: Epub 20131022, 10.1016/j.ejphar.2013.09.075. [DOI] [PubMed] [Google Scholar]
- 235. Lee L. Y., Abbott L., Mahlangu B., Moodie S. J., and Anderson S., “The Management of Cyclic Vomiting Syndrome: A Systematic Review,” European Journal of Gastroenterology and Hepatology 24, no. 9 (2012): 1001–1006: Epub 2012/05/29, 10.1097/MEG.0b013e328355638f. [DOI] [PubMed] [Google Scholar]
- 236. Li B. U., Murray R. D., Heitlinger L. A., Robbins J. L., and Hayes J. R., “Is Cyclic Vomiting Syndrome Related to Migraine?,” Journal of Pediatrics 134, no. 5 (1999): 567–572: Epub 1999/05/06, 10.1016/s0022-3476(99)70242-8. [DOI] [PubMed] [Google Scholar]
- 237. Dipasquale V., Falsaperla R., Bongiovanni A., Ruggieri M., and Romano C., “Clinical Features and Long‐Term Outcomes in Pediatric Cyclic Vomiting Syndrome: A 9‐year Experience at Three Tertiary Academic Centers,” Neuro‐Gastroenterology and Motility 34, no. 3 (2022): e14224: Epub 2021/08/26, 10.1111/nmo.14224. [DOI] [PubMed] [Google Scholar]
- 238. Partovi Op M., Cheng S., Garacci Z., and Venkatesan T., “Clinical Characteristics and Long‐Term Outcomes in Patients With Cyclic Vomiting Syndrome: A 12‐Year Experience At a Tertiary Referral Center,” Gastroenterology (2022): S69–S70. [DOI] [PubMed] [Google Scholar]
- 239. Boles R. G., Adams K., and Li B. U., “Maternal Inheritance in Cyclic Vomiting Syndrome,” American Journal of Medical Genetics, Part A 133a, no. 1 (2005): 71–77: Epub 2005/01/12, 10.1002/ajmg.a.30524. [DOI] [PubMed] [Google Scholar]
- 240. Veenin K., Wattanasirichaigoon D., Suktitipat B., et al., “Association of Mitochondrial DNA Polymorphisms With Pediatric‐Onset Cyclic Vomiting Syndrome,” Frontiers in pediatrics 10 (2022): 876436: Epub 2022/06/11, 10.3389/fped.2022.876436. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 241. Ellingsen D. M., Garcia R. G., Lee J., et al., “Cyclic Vomiting Syndrome Is Characterized by Altered Functional Brain Connectivity of the Insular Cortex: A Cross‐Comparison With Migraine and Healthy Adults,” Neuro‐Gastroenterology and Motility 29, no. 6 (2017): Epub 2016/12/03, 10.1111/nmo.13004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 242. Rashid S., Weaver S., Al‐Robaidi K., Dure L., and Singh S., “Brain Magnetic Resonance Imaging (MRI) White Matter Hyperintensities in Cyclic Vomiting Syndrome With or Without Migraine,” Journal of Child Neurology 37, no. 3 (2022): 218–221: Epub 2021/12/09, 10.1177/08830738211027972. [DOI] [PubMed] [Google Scholar]
- 243. Sagar R. C., Sood R., Gracie D. J., et al., “Cyclic Vomiting Syndrome Is a Prevalent and Under‐recognized Condition in the Gastroenterology Outpatient Clinic,” Neuro‐Gastroenterology and Motility 30, no. 1 (2018): Epub 2017/07/27, 10.1111/nmo.13174. [DOI] [PubMed] [Google Scholar]
- 244. Taranukha T., Charan Suresh Kumar V., Seamon A., Sahr N., Szabo A., and Venkatesan T., “Depression, Young Age, Chronic Marijuana Use, and Interepisodic Symptoms Predict Psychological Distress in Patients With Cyclic Vomiting Syndrome,” Neuro‐Gastroenterology and Motility 30, no. 4 (2018): e13245: Epub 20171120, 10.1111/nmo.13245. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 245. Aziz I., Palsson O. S., Whitehead W. E., Sperber A. D., Simrén M., and Törnblom H., “Epidemiology, Clinical Characteristics, and Associations for Rome IV Functional Nausea and Vomiting Disorders in Adults,” Clinical Gastroenterology and Hepatology 17, no. 5 (2019): 878–886: Epub 20180529, 10.1016/j.cgh.2018.05.020. [DOI] [PubMed] [Google Scholar]
- 246. Dang‐Vu G., Rein L., Szabo A., and Venkatesan T., “Low Patient Engagement Is Associated With Reduced Health‐Related Quality of Life in Adults With Cyclic Vomiting Syndrome,” Scandinavian Journal of Gastroenterology 57, no. 9 (2022): 1030–1035: Epub 20220429, 10.1080/00365521.2022.2064724. [DOI] [PubMed] [Google Scholar]
- 247. Tarbell S. E. and Li B. U., “Health‐related Quality of Life in Children and Adolescents With Cyclic Vomiting Syndrome: A Comparison With Published Data on Youth With Irritable Bowel Syndrome and Organic Gastrointestinal Disorders,” Journal of Pediatrics 163, no. 2 (2013): 493–497: Epub 20130226, 10.1016/j.jpeds.2013.01.025. [DOI] [PubMed] [Google Scholar]
- 248. Tarbell S. E. and Li B. U., “Anxiety Measures Predict Health‐Related Quality of Life in Children and Adolescents With Cyclic Vomiting Syndrome,” Journal of Pediatrics 167, no. 3 (2015): 633–638.e1: Epub 20150618, 10.1016/j.jpeds.2015.05.032. [DOI] [PubMed] [Google Scholar]
- 249. Namin F., Patel J., Lin Z., Dusing R., Foran P., and McCallum R., “Recognizing Abnormal Patterns on PET Brain Images in Adult Patients With Cyclic Vomiting Syndrome (CVS),” Gastroenterology 125 (2006): A124. [Google Scholar]
- 250. Drossman D. A. and Hasler W. L., “Rome IV‐Functional GI Disorders: Disorders of Gut‐Brain Interaction,” Gastroenterology 150, no. 6 (2016): 1257–1261, 10.1053/j.gastro.2016.03.035. [DOI] [PubMed] [Google Scholar]
- 251. Sikand M. and Sharma P., “Psychological Intervention in Cyclic Vomiting Syndrome in Adolescents: A Case Series,” Journal of Child and Adolescent Mental Health 31, no. 3 (2019): 182–188, 10.2989/17280583.2019.1674660. [DOI] [PubMed] [Google Scholar]
- 252. Ogiso K., Koriyama N., Akao A., et al., “Type 1 Diabetes Complicated With Uncontrollable Adult Cyclic Vomiting Syndrome: A Case Report,” Journal of Diabetes and Metabolic Disorders 14 (2015): 72: Epub 2015/09/25, 10.1186/s40200-015-0206-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 253. Sawhney M. S., Prakash C., Lustman P. J., and Clouse R. E., “Tricyclic Antidepressants for Chronic Vomiting in Diabetic Patients,” Digestive Diseases and Sciences 52, no. 2 (2007): 418–424: Epub 2007/01/02, 10.1007/s10620-006-9378-8. [DOI] [PubMed] [Google Scholar]
- 254. Bhandari S. and Venkatesan T., “Novel Treatments for Cyclic Vomiting Syndrome: Beyond Ondansetron and Amitriptyline,” Current Treatment Options in Gastroenterology 14, no. 4 (2016): 495–506: Epub 2016/10/21, 10.1007/s11938-016-0114-y. [DOI] [PubMed] [Google Scholar]
- 255. Hee W., “Acupuncture in the Treatment of Hysterical Muslim and Functional Vomiting,” Medical Journal of Malaysia, no. 2 (1978): XXXIII. [PubMed] [Google Scholar]
- 256. Isoldi S., Di Nardo G., Mallardo S., et al., “Cyclic Vomiting Syndrome in Children: A Nationwide Survey of Current Practice on Behalf of the Italian Society of Pediatric Gastroenterology, Hepatology and Nutrition (SIGENP) and Italian Society of Pediatric Neurology (SINP),” Italian Journal of Pediatrics 48, no. 1 (2022): 156: Epub 20220830, 10.1186/s13052-022-01346-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 257. Cristofori F., Thapar N., Saliakellis E., et al., “Efficacy of the Neurokinin‐1 Receptor Antagonist Aprepitant in Children With Cyclical Vomiting Syndrome,” Alimentary Pharmacology & Therapeutics 40, no. 3 (2014): 309–317: Epub 20140605, 10.1111/apt.12822. [DOI] [PubMed] [Google Scholar]
- 258. Bagherian Z., Yaghini O., Saneian H., and Badihian S., “Comparison of the Efficacy of Amitriptyline and Topiramate in Prophylaxis of Cyclic Vomiting Syndrome,” Iranian Journal of Child Neurology 13, no. 1 (2019): 37–44. [PMC free article] [PubMed] [Google Scholar]
- 259. Badihian N., Saneian H., Badihian S., and Yaghini O., “Prophylactic Therapy of Cyclic Vomiting Syndrome in Children: Comparison of Amitriptyline and Cyproheptadine: A Randomized Clinical Trial,” American Journal of Gastroenterology 113, no. 1 (2018): 135–140: Epub 20170718, 10.1038/ajg.2017.194. [DOI] [PubMed] [Google Scholar]
- 260. Boles R. G., Lovett‐Barr M. R., Preston A., Li B. U., and Adams K., “Treatment of Cyclic Vomiting Syndrome With Co‐enzyme Q10 and Amitriptyline, a Retrospective Study,” BMC Neurology 10, no. 1 (2010): 10: Epub 2010/01/30, 10.1186/1471-2377-10-10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 261. McLoughlin L. M., Trimble E. R., Jackson P., and Chong S. K., “L‐Carnitine in Cyclical Vomiting Syndrome,” Archives of Disease in Childhood 89, no. 12 (2004): 1180, 10.1136/adc.2003.047183. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 262. Tillman E. M. and Harvath E. M., “Cyclic Vomiting Syndrome in Pediatric Patients: A Review of Therapeutics,” Journal of Pediatric Pharmacology and Therapeutics: JPPT: the official journal of PPAG 27, no. 1 (2022): 12–18: Epub 2022/01/11, 10.5863/1551-6776-27.1.12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 263. Boles R. G., “High Degree of Efficacy in the Treatment of Cyclic Vomiting Syndrome With Combined Co‐enzyme Q10, L‐Carnitine and Amitriptyline, a Case Series,” BMC Neurology 11, no. 1 (2011): 102: Epub 2011/08/19, 10.1186/1471-2377-11-102. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 264. Li B. U. K., “Managing Cyclic Vomiting Syndrome in Children: Beyond the Guidelines,” European Journal of Pediatrics 177, no. 10 (2018): 1435–1442: Epub 2018/08/05, 10.1007/s00431-018-3218-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 265. Sorensen C. J., DeSanto K., Borgelt L., Phillips K. T., and Monte A. A., “Cannabinoid Hyperemesis Syndrome: Diagnosis, Pathophysiology, and Treatment‐A Systematic Review,” Journal of Medical Toxicology 13, no. 1 (2017): 71–87: Epub 20161220, 10.1007/s13181-016-0595-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 266. Venkatesan T., Levinthal D. J., Li B. U. K., et al., “Role of Chronic Cannabis Use: Cyclic Vomiting Syndrome vs Cannabinoid Hyperemesis Syndrome,” Neuro‐Gastroenterology and Motility 31, no. S2 (2019), 10.1111/nmo.13606. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 267. UNODC , World Drug Report 2022 (United nations, 2022): (United Nations publication, 2022 https://www.unodc.org/unodc/en/data‐and‐analysis/world‐drug‐report‐2022.html. [Google Scholar]
- 268. Whiting P. F., Wolff R. F., Deshpande S., et al., “Cannabinoids for Medical Use: A Systematic Review and Meta‐Analysis,” JAMA 313, no. 24 (2015): 2456–2473, 10.1001/jama.2015.6358. [DOI] [PubMed] [Google Scholar]
- 269. Bruguera P., Miquel L., López‐Pelayo H., and Balcells‐ Oliveró M., “Cannabinoid Hyperemesis Syndrome; a Prevalence Study,” European Neuropsychopharmacology 25 (2015): S622–S623. [Google Scholar]
- 270. Venkatesan T., Rein L., Banerjee A., Hillard C., and Lisdahl K. M., “Patterns of Cannabis Use and Effects on Symptoms in Patients With Cyclic Vomiting Syndrome,” Gastroenterology 154, no. 6 (2018): S‐555–S‐6, 10.1016/S0016-5085(18)32055-9. [DOI] [PubMed] [Google Scholar]
- 271. Blumentrath C. G., Dohrmann B., and Ewald N., “Cannabinoid Hyperemesis and the Cyclic Vomiting Syndrome in Adults: Recognition, Diagnosis, Acute and Long‐Term Treatment,” GMS German Medical Science 15 (2017): Doc06: Epub 20170321, 10.3205/000247. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 272. Galli J. A., Sawaya R. A., and Friedenberg F. K., “Cannabinoid Hyperemesis Syndrome,” Current Drug Abuse Reviews 4, no. 4 (2011): 241–249, 10.2174/1874473711104040241. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 273. Darmani N. A., “The Potent Emetogenic Effects of the Endocannabinoid, 2‐AG (2‐arachidonoylglycerol) Are Blocked by Delta(9)‐Tetrahydrocannabinol and Other Cannnabinoids,” Journal of Pharmacology and Experimental Therapeutics 300, no. 1 (2002): 34–42, 10.1124/jpet.300.1.34. [DOI] [PubMed] [Google Scholar]
- 274. Sontineni S. P., Chaudhary S., Sontineni V., and Lanspa S. J., “Cannabinoid Hyperemesis Syndrome: Clinical Diagnosis of an Underrecognised Manifestation of Chronic Cannabis Abuse,” World Journal of Gastroenterology 15, no. 10 (2009): 1264–1266, 10.3748/wjg.15.1264. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 275. Allen J. H., de Moore G. M., Heddle R., and Twartz J. C., “Cannabinoid Hyperemesis: Cyclical Hyperemesis in Association With Chronic Cannabis Abuse,” Gut 53, no. 11 (2004): 1566–1570, 10.1136/gut.2003.036350. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 276. Simonetto D. A., Oxentenko A. S., Herman M. L., and Szostek J. H., “Cannabinoid Hyperemesis: A Case Series of 98 Patients,” Mayo Clinic Proceedings 87, no. 2 (2012): 114–119, 10.1016/j.mayocp.2011.10.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 277. Morris R. and Fisher M., “Cannabinoid Hyperemesis Syndrome: A Specific Cause of Cyclical Vomiting,” International Journal of Adolescent Medicine and Health 26, no. 1 (2014): 153–156, 10.1515/ijamh-2012-0113. [DOI] [PubMed] [Google Scholar]
- 278. Richards J. R., Gordon B. K., Danielson A. R., and Moulin A. K., “Pharmacologic Treatment of Cannabinoid Hyperemesis Syndrome: A Systematic Review,” Pharmacotherapy: The Journal of Human Pharmacology and Drug Therapy 37, no. 6 (2017): 725–734: Epub 20170512, 10.1002/phar.1931. [DOI] [PubMed] [Google Scholar]
- 279. Hammerman S., Shelton S., Mills E., et al., “Antiemetics Effectiveness for Cannabinoid Hyperemesis Syndrome (CHS) Emergency Department,” Clinical Toxicology 57, no. 10 (2019): 873: encounters, 10.1080/15563650.2019.1636569. [DOI] [Google Scholar]
- 280. Dezieck L., Hafez Z., Conicella A., et al., “Resolution of Cannabis Hyperemesis Syndrome With Topical Capsaicin in the Emergency Department: A Case Series,” Clinical Toxicology 55, no. 8 (2017): 908–913: Epub 20170511, 10.1080/15563650.2017.1324166. [DOI] [PubMed] [Google Scholar]
- 281. Dean D. J., Sabagha N., Rose K., et al., “A Pilot Trial of Topical Capsaicin Cream for Treatment of Cannabinoid Hyperemesis Syndrome,” Academic Emergency Medicine 27, no. 11 (2020): 1166–1172: Epub 20200720, 10.1111/acem.14062. [DOI] [PubMed] [Google Scholar]
- 282. Pourmand A., Esmailian G., Mazer‐Amirshahi M., Lee‐Park O., and Tran Q. K., “Topical Capsaicin for the Treatment of Cannabinoid Hyperemesis Syndrome, a Systematic Review and Meta‐Analysis,” American Journal of Emergency Medicine 43 (2021): 35–40: Epub 20210115, 10.1016/j.ajem.2021.01.004. [DOI] [PubMed] [Google Scholar]
- 283. Wagner S., Hoppe J., Zuckerman M., Schwarz K., and McLaughlin J., “Efficacy and Safety of Topical Capsaicin for Cannabinoid Hyperemesis Syndrome in the Emergency Department,” Clinical Toxicology 58, no. 6 (2020): 471–475, 10.1080/15563650.2019.1660783. [DOI] [PubMed] [Google Scholar]
- 284. Yusuf H. M., Geier C., Staidle A., and Montoy J. C. C., “Efficacy of Topical Capsaicin for the Treatment of Cannabinoid Hyperemesis Syndrome: A Retrospective Cohort Study,” American Journal of Emergency Medicine 43 (2021): 142–148: Epub 20210129, 10.1016/j.ajem.2021.01.073. [DOI] [PubMed] [Google Scholar]
- 285. Valdovinos E. M., Frazee B. W., Hailozian C., Haro D. A., and HerringNonopioid A. A. A., “Nonbenzodiazepine Treatment Approach for Intractable Nausea and Vomiting in the Emergency Department,” Journal of Clinical Gastroenterology 54, no. 4 (2020): 327–332, 10.1097/MCG.0000000000001258. [DOI] [PubMed] [Google Scholar]
- 286. Senderovich H., Patel P., Jimenez Lopez B., and Waicus S., “A Systematic Review on Cannabis Hyperemesis Syndrome and its Management Options,” Medical Principles and Practice 31, no. 1 (2022): 29–38: Epub 20211101, 10.1159/000520417. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 287. Gajendran M., Sifuentes J., Bashashati M., and McCallum R., “Cannabinoid Hyperemesis Syndrome: Definition, Pathophysiology, Clinical Spectrum, Insights into Acute and Long‐Term Management,” Journal of Investigative Medicine 68, no. 8 (2020): 1309–1316, 10.1136/jim-2020-001564. [DOI] [PubMed] [Google Scholar]
- 288. Absah I., Rishi A., Talley N. J., Katzka D., and Halland M., “Rumination Syndrome: Pathophysiology, Diagnosis, and Treatment,” Neuro‐Gastroenterology and Motility 29, no. 4 (2017): Epub 20161020, 10.1111/nmo.12954. [DOI] [PubMed] [Google Scholar]
- 289. Amarnath R. P., Abell T. L., and Malagelada J. R., “The Rumination Syndrome in Adults. A Characteristic Manometric Pattern,” Annals of Internal Medicine 105, no. 4 (1986): 513–518, 10.7326/0003-4819-105-4-513. [DOI] [PubMed] [Google Scholar]
- 290. Soykan I., Chen J., Kendall B. J., and McCallum R. W., “The Rumination Syndrome: Clinical and Manometric Profile, Therapy, and Long‐Term Outcome,” Digestive Diseases and Sciences 42, no. 9 (1997): 1866–1872, 10.1023/a:1018854925196. [DOI] [PubMed] [Google Scholar]
- 291. Barba E., Burri E., Accarino A., et al., “Biofeedback‐guided Control of Abdominothoracic Muscular Activity Reduces Regurgitation Episodes in Patients With Rumination,” Clinical Gastroenterology and Hepatology 13, no. 1 (2015): 100–106.e1: Epub 20140424, 10.1016/j.cgh.2014.04.018. [DOI] [PubMed] [Google Scholar]
- 292. Lopez‐Colombo A., Morgan D., Bravo‐Gonzalez D., Montiel‐Jarquin A., Mendez‐Martinez S., and Schmulson M., “The Epidemiology of Functional Gastrointestinal Disorders in Mexico: A Population‐Based Study,” Gastroenterology research and practice 2012 (2012): 606174–606178, 10.1155/2012/606174. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 293. Schmulson M., Ortiz O., Santiago‐Lomeli M., et al., “Frequency of Functional Bowel Disorders Among Healthy Volunteers in Mexico City,” Digestive Diseases 24, no. 3‐4 (2006): 342–347, 10.1159/000092887. [DOI] [PubMed] [Google Scholar]
- 294. Thompson W. G., Irvine E. J., Pare P., Ferrazzi S., and Rance L., “Functional Gastrointestinal Disorders in Canada: First Population‐Based Survey Using Rome II Criteria With Suggestions for Improving the Questionnaire,” Digestive Diseases and Sciences 47, no. 1 (2002): 225–235, 10.1023/a:1013208713670. [DOI] [PubMed] [Google Scholar]
- 295. Koloski N. A., Talley N. J., and Boyce P. M., “Epidemiology and Health Care Seeking in the Functional GI Disorders: A Population‐Based Study,” American Journal of Gastroenterology 97, no. 9 (2002): 2290–2299, 10.1111/j.1572-0241.2002.05783.x. [DOI] [PubMed] [Google Scholar]
- 296. Boyce P. M., Talley N. J., Burke C., and Koloski N. A., “Epidemiology of the Functional Gastrointestinal Disorders Diagnosed According to Rome II Criteria: An Australian Population‐Based Study,” Internal Medicine Journal 36, no. 1 (2006): 28–36, 10.1111/j.1445-5994.2006.01006.x. [DOI] [PubMed] [Google Scholar]
- 297. Zand I. M., Jones M. P., Halland M., et al., “Prevalence, Symptoms and Risk Factor Profile of Rumination Syndrome and Functional Dyspepsia: A Population‐Based Study,” Alimentary Pharmacology & Therapeutics 54, no. 11‐12 (2021): 1416–1431: Epub 20211009, 10.1111/apt.16630. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 298. Josefsson A., Hreinsson J. P., Simrén M., et al., “Global Prevalence and Impact of Rumination Syndrome,” Gastroenterology 162, no. 3 (2022): 731–742.e9: Epub 20211111, 10.1053/j.gastro.2021.11.008. [DOI] [PubMed] [Google Scholar]
- 299. Almansa C., Rey E., Sanchez R. G., Sanchez A. A., and Diaz‐Rubio M., “Prevalence of Functional Gastrointestinal Disorders in Patients With Fibromyalgia and the Role of Psychologic Distress,” Clinical Gastroenterology and Hepatology 7, no. 4 (2009): 438–445, 10.1016/j.cgh.2008.12.005. [DOI] [PubMed] [Google Scholar]
- 300. Wang X., Luscombe G. M., Boyd C., Kellow J., and Abraham S., “Functional Gastrointestinal Disorders in Eating Disorder Patients: Altered Distribution and Predictors Using ROME III Compared to ROME II Criteria,” World Journal of Gastroenterology 20, no. 43 (2014): 16293–16299, 10.3748/wjg.v20.i43.16293. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 301. Lewis M. L., Palsson O. S., Whitehead W. E., and van Tilburg M. A. L., “Prevalence of Functional Gastrointestinal Disorders in Children and Adolescents,” Journal of Pediatrics 177 (2016): 39–43 e3, 10.1016/j.jpeds.2016.04.008. [DOI] [PubMed] [Google Scholar]
- 302. Peralta‐Palmezano J. J. and Guerrero‐Lozano R., “Prevalence of Functional Gastrointestinal Disorders in School Children and Adolescents,” Korean journal of gastroenterology = Taehan Sohwagi Hakhoe chi 73, no. 4 (2019): 207–212, 10.4166/kjg.2019.73.4.207. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 303. Chogle A., Velasco‐Benitez C. A., Koppen I. J., Moreno J. E., Ramirez Hernandez C. R., and Saps M., “A Population‐Based Study on the Epidemiology of Functional Gastrointestinal Disorders in Young Children,” Journal of Pediatrics 179 (2016): 139–143 e1, 10.1016/j.jpeds.2016.08.095. [DOI] [PubMed] [Google Scholar]
- 304. Rogers B., Stratton P., Victor J., Kennedy B., and Andres M., “Chronic Regurgitation Among Persons With Mental Retardation: A Need for Combined Medical and Interdisciplinary Strategies,” American Journal on Mental Retardation: American Journal of Mental Retardation 96, no. 5 (1992): 522–527. [PubMed] [Google Scholar]
- 305. Levine D. F., Wingate D. L., Pfeffer J. M., and Butcher P., “Habitual Rumination: A Benign Disorder,” British Medical Journal 287, no. 6387 (1983): 255–256, 10.1136/bmj.287.6387.255. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 306. Nakagawa K., Sawada A., Hoshikawa Y., et al., “Persistent Postprandial Regurgitation vs Rumination in Patients With Refractory Gastroesophageal Reflux Disease Symptoms: Identification of a Distinct Rumination Pattern Using Ambulatory Impedance‐pH Monitoring,” American Journal of Gastroenterology 114, no. 8 (2019): 1248–1255: Epub 2019/06/28, 10.14309/ajg.0000000000000295. [DOI] [PubMed] [Google Scholar]
- 307. Nikaki K. and Sifrim D., “Rumination Syndrome “Real Prevalence”: A Need to Increase Awareness, Early Recognition, and Specific Management,” Gastroenterology 162, no. 3 (2022): 696–697: Epub 20211211, 10.1053/j.gastro.2021.12.237. [DOI] [PubMed] [Google Scholar]
- 308. Chial H. J., Camilleri M., Williams D. E., Litzinger K., and Perrault J., “Rumination Syndrome in Children and Adolescents: Diagnosis, Treatment, and Prognosis,” Pediatrics 111, no. 1 (2003): 158–162, 10.1542/peds.111.1.158. [DOI] [PubMed] [Google Scholar]
- 309. Thumshirn M., Camilleri M., Hanson R. B., Williams D. E., Schei A. J., and Kammer P. P., “Gastric Mechanosensory and Lower Esophageal Sphincter Function in Rumination Syndrome,” American Journal of Physiology 275, no. 2 (1998): G314–G321, 10.1152/ajpgi.1998.275.2.G314. [DOI] [PubMed] [Google Scholar]
- 310. Kessing B. F., Bredenoord A. J., and Smout A. J., “Objective Manometric Criteria for the Rumination Syndrome,” American Journal of Gastroenterology 109, no. 1 (2014): 52–59, 10.1038/ajg.2013.428. [DOI] [PubMed] [Google Scholar]
- 311. Geysen H., Michielsen S., Rommel N., Vanuytsel T., Tack J., and Pauwels A., “The Gastro‐Sphincteric Pressure Gradient: A New Parameter to Diagnose a Rumination Episode,” Neuro‐Gastroenterology and Motility 33, no. 6 (2021): e14068: Epub 2020/12/23, 10.1111/nmo.14068. [DOI] [PubMed] [Google Scholar]
- 312. DeLay K., Pandolfino J. E., Roman S., et al., “Diagnostic Yield and Reliability of Post‐prandial High‐Resolution Manometry and Impedance‐Ph for Detecting Rumination and Supragastric Belching in PPI Non‐responders,” Neuro‐Gastroenterology and Motility 33, no. 10 (2021): e14106: Epub 2021/03/10, 10.1111/nmo.14106. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 313. Nikaki K., Rybak A., Nakagawa K., et al., “Rumination Syndrome in Children Presenting With Refractory Gastroesophageal Reflux Symptoms,” Journal of Pediatric Gastroenterology and Nutrition 70, no. 3 (2020): 330–335: Epub 2020/02/23, 10.1097/MPG.0000000000002569. [DOI] [PubMed] [Google Scholar]
- 314. Stanghellini V., Chan F. K., Hasler W. L., et al., “Gastroduodenal Disorders,” Gastroenterology 150, no. 6 (2016): 1380–1392, 10.1053/j.gastro.2016.02.011. [DOI] [PubMed] [Google Scholar]
- 315. Bredenoord A. J., Chial H. J., Camilleri M., Mullan B. P., and Murray J. A., “Gastric Accommodation and Emptying in Evaluation of Patients With Upper Gastrointestinal Symptoms,” Clinical Gastroenterology and Hepatology 1, no. 4 (2003): 264–272, 10.1053/s1542-3565(03)00130-7. [DOI] [PubMed] [Google Scholar]
- 316. Jones M. P., Tack J., Van Oudenhove L., et al., “Mood and Anxiety Disorders Precede Development of Functional Gastrointestinal Disorders in Patients but Not in the Population,” Clinical Gastroenterology and Hepatology 15, no. 7 (2017): 1014–1020 e4, 10.1016/j.cgh.2016.12.032. [DOI] [PubMed] [Google Scholar]
- 317. Tucker E., Knowles K., Wright J., and Fox M. R., “Rumination Variations: Aetiology and Classification of Abnormal Behavioural Responses to Digestive Symptoms Based on High‐Resolution Manometry Studies,” Alimentary Pharmacology & Therapeutics 37, no. 2 (2013): 263–274: Epub 2012/11/24, 10.1111/apt.12148. [DOI] [PubMed] [Google Scholar]
- 318. Yadlapati R., Tye M., Roman S., Kahrilas P. J., Ritter K., and Pandolfino J. E., “Postprandial High‐Resolution Impedance Manometry Identifies Mechanisms of Nonresponse to Proton Pump Inhibitors,” Clinical Gastroenterology and Hepatology 16, no. 2 (2018): 211–218.e1: Epub 2017/09/16, 10.1016/j.cgh.2017.09.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 319. Koukias N., Woodland P., Yazaki E., and Sifrim D., “Supragastric Belching: Prevalence and Association With Gastroesophageal Reflux Disease and Esophageal Hypomotility,” J Neurogastroenterol Motil 21, no. 3 (2015): 398–403: Epub 2015/07/02, 10.5056/jnm15002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 320. Glasinovic E., Wynter E., Arguero J., et al., “Treatment of Supragastric Belching With Cognitive Behavioral Therapy Improves Quality of Life and Reduces Acid Gastroesophageal Reflux,” American Journal of Gastroenterology 113, no. 4 (2018): 539–547: Epub 2018/02/21, 10.1038/ajg.2018.15. [DOI] [PubMed] [Google Scholar]
- 321. Halland M., “Rumination Syndrome: When to Suspect and How to Treat,” Current Opinion in Gastroenterology 35, no. 4 (2019): 387–393, 10.1097/mog.0000000000000549. [DOI] [PubMed] [Google Scholar]
- 322. Friesen H. J., Rosen J., Low Kapalu C., et al., “Mucosal Eosinophils, Mast Cells, and Intraepithelial Lymphocytes in Youth With Rumination Syndrome,” Neuro‐Gastroenterology and Motility 33, no. 10 (2021): e14155: Epub 2021/04/11, 10.1111/nmo.14155. [DOI] [PubMed] [Google Scholar]
- 323. Murray H. B., Pasricha T. S., Jehangir A., Thomas J. J., Kuo B., and Parkman H. P., “Detection and Characteristics of Rumination Syndrome in Patients Presenting for Gastric Symptom Evaluation,” Neuro‐Gastroenterology and Motility 33, no. 8 (2021): e14103: Epub 2021/03/18, 10.1111/nmo.14103. [DOI] [PubMed] [Google Scholar]
- 324. Cai J. X., Wong D., Lee D. J. H., and Chan W. W., “Eating and Psychiatric Disorders Are Independent Risk Factors for Rumination Syndrome,” Journal of Clinical Gastroenterology 56, no. 3 (2022): 228–233: Epub 2021/05/15, 10.1097/mcg.0000000000001510. [DOI] [PubMed] [Google Scholar]
- 325. Lindvall Dahlgren C., Wisting L., and Rø Ø, “Feeding and Eating Disorders in the DSM‐5 Era: A Systematic Review of Prevalence Rates in Non‐clinical Male and Female Samples,” Journal of Eating Disorders 5, no. 1 (2017): 56: Epub 20171228, 10.1186/s40337-017-0186-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 326. Guidelines‐‐Rome III Diagnostic Criteria for Functional Gastrointestinal Disorders.” Journal of Gastrointestinal and Liver Diseases 15, no. 3 (2006): 307–312. [PubMed] [Google Scholar]
- 327. Avalos D. J., Robles A., Paik I. J., Hershman M., and McCallum R. W., Nausea, Belching, and Rumination Disorders. Clinical and Basic Neurogastroenterology and Motility (Elsevier, 2020), 293–304. [Google Scholar]
- 328. Chial H. J. and Camilleri M., “A Twenty‐One‐Year‐Old College Student With Postprandial Regurgitation and Weight Loss,” Clinical Gastroenterology and Hepatology 4, no. 11 (2006): 1314–1317: Epub 20061023, 10.1016/j.cgh.2006.09.008. [DOI] [PubMed] [Google Scholar]
- 329. Chitkara D. K., Bredenoord A. J., Talley N. J., and Whitehead W. E., “Aerophagia and Rumination: Recognition and Therapy,” Current Treatment Options in Gastroenterology 9, no. 4 (2006): 305–313, 10.1007/s11938-006-0012-9. [DOI] [PubMed] [Google Scholar]
- 330. Clouse R. E., Richter J. E., Heading R. C., Janssens J., and Wilson J. A., “Functional Esophageal Disorders,” Gut 45, no. Suppl 2 (1999): 6–ii36: (Suppl 2):Ii31, 10.1136/gut.45.2008.ii31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 331. Eckern M., Stevens W., and Mitchell J., “The Relationship Between Rumination and Eating Disorders,” International Journal of Eating Disorders 26, no. 4 (1999): 414–419, 10.1002/(sici)1098-108x(199912)26:4<414::aid-eat7>3.0.co;2-8. [DOI] [PubMed] [Google Scholar]
- 332. Gupta R., Kalla M., and Gupta J. B., “Adult Rumination Syndrome: Differentiation From Psychogenic Intractable Vomiting,” Indian Journal of Psychiatry 54, no. 3 (2012): 283–285, 10.4103/0019-5545.102434. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 333. Jones C. J. and Samuel J., “The Diagnosis of Eating Disorders in Adults With Learning Disabilities: Conceptualisation and Implications for Clinical Practice,” European Eating Disorders Review 18, no. 5 (2010): 352–366, 10.1002/erv.1007. [DOI] [PubMed] [Google Scholar]
- 334. O'Brien M. D., Bruce B. K., and Camilleri M., “The Rumination Syndrome: Clinical Features rather Than Manometric Diagnosis,” Gastroenterology 108, no. 4 (1995): 1024–1029: Epub 1995/04/01, 10.1016/0016-5085(95)90199-x. [DOI] [PubMed] [Google Scholar]
- 335. Dinkler L. and Bryant‐Waugh R., “Assessment of Avoidant Restrictive Food Intake Disorder, pica and Rumination Disorder: Interview and Questionnaire Measures,” Current Opinion in Psychiatry 34, no. 6 (2021): 532–542, 10.1097/yco.0000000000000736. [DOI] [PubMed] [Google Scholar]
- 336. Matson J. L. and Kuhn D. E., “Identifying Feeding Problems in Mentally Retarded Persons: Development and Reliability of the Screening Tool of Feeding Problems (STEP),” Research in Developmental Disabilities 22, no. 2 (2001): 165–172, 10.1016/s0891-4222(01)00065-8. [DOI] [PubMed] [Google Scholar]
- 337. Sysko R., Glasofer D. R., Hildebrandt T., et al., “The Eating Disorder Assessment for DSM‐5 (EDA‐5): Development and Validation of a Structured Interview for Feeding and Eating Disorders,” International Journal of Eating Disorders 48, no. 5 (2015): 452–463: Epub 20150130, 10.1002/eat.22388. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 338. Bryant‐Waugh R., Micali N., Cooke L., Lawson E. A., Eddy K. T., and Thomas J. J., “Development of the Pica, ARFID, and Rumination Disorder Interview, a Multi‐Informant, Semi‐structured Interview of Feeding Disorders Across the Lifespan: A Pilot Study for Ages 10‐22,” International Journal of Eating Disorders 52, no. 4 (2019): 378–387: Epub 20181012, 10.1002/eat.22958. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 339. Gyawali C. P., Carlson D. A., Chen J. W., Patel A., Wong R. J., and Yadlapati R. H., “ACG Clinical Guidelines: Clinical Use of Esophageal Physiologic Testing,” American Journal of Gastroenterology 115, no. 9 (2020): 1412–1428, 10.14309/ajg.0000000000000734. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 340. Gyawali C. P. and Penagini R., “Clinical Usefulness of Esophageal High Resolution Manometry and Adjunctive Tests: An Update,” Digestive and Liver Disease 53, no. 11 (2021): 1373–1380: Epub 20210511, 10.1016/j.dld.2021.04.007. [DOI] [PubMed] [Google Scholar]
- 341. Rommel N., Tack J., Arts J., Caenepeel P., Bisschops R., and Sifrim D., “Rumination or Belching‐Regurgitation? Differential Diagnosis Using Oesophageal Impedance‐Manometry,” Neuro‐Gastroenterology and Motility 22, no. 4 (2010): e97–e104: Epub 20091125, 10.1111/j.1365-2982.2009.01431.x. [DOI] [PubMed] [Google Scholar]
- 342. Gourcerol G., Dechelotte P., Ducrotte P., and Leroi A. M., “Rumination Syndrome: When the Lower Oesophageal Sphincter Rises,” Digestive and Liver Disease 43, no. 7 (2011): 571–574: Epub 20110216, 10.1016/j.dld.2011.01.005. [DOI] [PubMed] [Google Scholar]
- 343. Pandolfino J. E., “Esophageal Function Testing,” Gastrointest Endosc Clin N Am 24, no. 4 (2014): xiii–xiv, 10.1016/j.giec.2014.07.003. [DOI] [PubMed] [Google Scholar]
- 344. Saleh C. M. and Bredenoord A. J., “Utilization of Esophageal Function Testing for the Diagnosis of the Rumination Syndrome and Belching Disorders,” Gastrointest Endosc Clin N Am 24, no. 4 (2014): 633–642: Epub 20140801, 10.1016/j.giec.2014.06.002. [DOI] [PubMed] [Google Scholar]
- 345. Sasegbon A., Hasan S. S., Disney B. R., and Vasant D. H., “Rumination Syndrome: Pathophysiology, Diagnosis and Practical Management,” Frontline Gastroenterology 13, no. 5 (2022): 440–446: Epub 20220111, 10.1136/flgastro-2021-101856. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 346. Kessing B. F., Govaert F., Masclee A. A., and Conchillo J. M., “Impedance Measurements and High‐Resolution Manometry Help to Better Define Rumination Episodes,” Scandinavian Journal of Gastroenterology 46, no. 11 (2011): 1310–1315: Epub 20110805, 10.3109/00365521.2011.605467. [DOI] [PubMed] [Google Scholar]
- 347. Kessing B. F., Smout A. J., and Bredenoord A. J., “Clinical Applications of Esophageal Impedance Monitoring and High‐Resolution Manometry,” Current Gastroenterology Reports 14, no. 3 (2012): 197–205, 10.1007/s11894-012-0253-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 348. Ravi K. and Katzka D. A., “Esophageal Impedance Monitoring: Clinical Pearls and Pitfalls,” American Journal of Gastroenterology 111, no. 9 (2016): 1245–1256: Epub 20160621, 10.1038/ajg.2016.256. [DOI] [PubMed] [Google Scholar]
- 349. Kessing B. F., Smout A. J., and Bredenoord A. J., “Current Diagnosis and Management of the Rumination Syndrome,” Journal of Clinical Gastroenterology 48, no. 6 (2014): 478–483, 10.1097/mcg.0000000000000142. [DOI] [PubMed] [Google Scholar]
- 350. Halland M., Ravi K., Nelson H. A., Katzka D. A., Talley N. J., and Crowell M. D., “Baseline Impedance Measured During High‐Resolution Esophageal Impedance Manometry in Patients With Rumination Syndrome is as Abnormal as in Patients With GERD,” Journal of Clinical Gastroenterology 54, no. 1 (2020): 28–34, 10.1097/mcg.0000000000001159. [DOI] [PubMed] [Google Scholar]
- 351. Fox M. R., Sweis R., Yadlapati R., et al., “Chicago Classification Version 4.0(©) Technical Review: Update on Standard High‐Resolution Manometry Protocol for the Assessment of Esophageal Motility,” Neuro‐Gastroenterology and Motility 33, no. 4 (2021): e14120: Epub 20210317, 10.1111/nmo.14120. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 352. Savarino E., Marabotto E., Bodini G., et al., “Advancements in the Use of Manometry and Impedance Testing for Esophageal Functional Disorders,” Expert Review of Gastroenterology & Hepatology 13, no. 5 (2019): 425–435: Epub 20190321, 10.1080/17474124.2019.1595587. [DOI] [PubMed] [Google Scholar]
- 353. Tack J., Pauwels A., Roman S., Savarino E., and Smout A., “European Society for Neurogastroenterology and Motility (ESNM) Recommendations for the Use of High‐Resolution Manometry of the Esophagus,” Neuro‐Gastroenterology and Motility 33, no. 5 (2021): e14043: Epub 20201204, 10.1111/nmo.14043. [DOI] [PubMed] [Google Scholar]
- 354. Zerbib F., Bredenoord A. J., Fass R., et al., “ESNM/ANMS Consensus Paper: Diagnosis and Management of Refractory Gastro‐Esophageal Reflux Disease,” Neuro‐Gastroenterology and Motility 33, no. 4 (2021): e14075: Epub 20201228, 10.1111/nmo.14075. [DOI] [PubMed] [Google Scholar]
- 355. Lee H., Rhee P. L., Park E. H., et al., “Clinical Outcome of Rumination Syndrome in Adults Without Psychiatric Illness: A Prospective Study,” Journal of Gastroenterology and Hepatology 22, no. 11 (2007): 1741–1747, 10.1111/j.1440-1746.2006.04617.x. [DOI] [PubMed] [Google Scholar]
- 356. Pauwels A., Broers C., Van Houtte B., Rommel N., Vanuytsel T., and Tack J., “A Randomized Double‐Blind, Placebo‐Controlled, Cross‐Over Study Using Baclofen in the Treatment of Rumination Syndrome,” American Journal of Gastroenterology 113, no. 1 (2018): 97–104: Epub 20171205, 10.1038/ajg.2017.441. [DOI] [PubMed] [Google Scholar]
- 357. Halland M., Parthasarathy G., Bharucha A. E., and Katzka D. A., “Diaphragmatic Breathing for Rumination Syndrome: Efficacy and Mechanisms of Action,” Neuro‐Gastroenterology and Motility 28, no. 3 (2016): 384–391: Epub 20151210, 10.1111/nmo.12737. [DOI] [PubMed] [Google Scholar]
- 358. Barba E., Accarino A., Soldevilla A., Malagelada J. R., and Azpiroz F., “Randomized, Placebo‐Controlled Trial of Biofeedback for the Treatment of Rumination,” American Journal of Gastroenterology 111, no. 7 (2016): 1007–1013: Epub 20160517, 10.1038/ajg.2016.197. [DOI] [PubMed] [Google Scholar]
- 359. Riehl M. E., Kinsinger S., Kahrilas P. J., Pandolfino J. E., and Keefer L., “Role of a Health Psychologist in the Management of Functional Esophageal Complaints,” Diseases of the Esophagus 28, no. 5 (2015): 428–436: Epub 20140403, 10.1111/dote.12219. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 360. Blondeau K., Boecxstaens V., Rommel N., et al., “Baclofen Improves Symptoms and Reduces Postprandial Flow Events in Patients With Rumination and Supragastric Belching,” Clinical Gastroenterology and Hepatology 10, no. 4 (2012): 379–384: Epub 20111109, 10.1016/j.cgh.2011.10.042. [DOI] [PubMed] [Google Scholar]
- 361. Robles A., Romero Y. A., Tatro E., Quezada H., and McCallum R. W., “Outcomes of Treating Rumination Syndrome With a Tricyclic Antidepressant and Diaphragmatic Breathing,” American Journal of the Medical Sciences 360, no. 1 (2020): 42–49: Epub 20200412, 10.1016/j.amjms.2020.04.003. [DOI] [PubMed] [Google Scholar]
- 362. Rajindrajith S., Devanarayana N. M., and Crispus Perera B. J., “Rumination Syndrome in Children and Adolescents: A School Survey Assessing Prevalence and Symptomatology,” BMC Gastroenterology 12, no. 1 (2012): 163, 10.1186/1471-230X-12-163. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 363. Khan S., Hyman P. E., Cocjin J., and Di Lorenzo C., “Rumination Syndrome in Adolescents,” Journal of Pediatrics 136, no. 4 (2000): 528–531: Epub 2001/02/07, 10.1016/s0022-3476(00)90018-0. [DOI] [PubMed] [Google Scholar]
- 364. Green A. D., Alioto A., Mousa H., and Di Lorenzo C., “Severe Pediatric Rumination Syndrome: Successful Interdisciplinary Inpatient Management,” Journal of Pediatric Gastroenterology and Nutrition 52, no. 4 (2011): 414–418: Epub 2011/03/17, 10.1097/MPG.0b013e3181fa06f3. [DOI] [PubMed] [Google Scholar]
- 365. Lamparyk K. and Stephens T. N., “Protocol and Outcome Evaluation of Comprehensive Outpatient Treatment of Adolescent Rumination Syndrome,” Journal of Pediatric Gastroenterology and Nutrition 75, no. 3 (2022): e38–e42: Epub 2022/06/11, 10.1097/mpg.0000000000003524. [DOI] [PubMed] [Google Scholar]
- 366. Tack J., Carbone F., Holvoet L., Vanheel H., Vanuytsel T., and Vandenberghe A., “The Use of Pictograms Improves Symptom Evaluation by Patients With Functional Dyspepsia,” Alimentary Pharmacology & Therapeutics 40, no. 5 (2014): 523–530: Epub 20140722, 10.1111/apt.12855. [DOI] [PubMed] [Google Scholar]
- 367. Jung H. K., Tae C. H., Moon C. M., Kim S. E., Shim K. N., and Jung S. A., “Chronic Unexplained Nausea in Adults: Prevalence, Impact on Quality of Life, and Underlying Organic Diseases in a Cohort of 5096 Subjects Comprehensively Investigated,” PLoS One 14, no. 12 (2019): e0225364: Epub 20191219, 10.1371/journal.pone.0225364. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 368. Camilleri M., Dubois D., Coulie B., et al., “Prevalence and Socioeconomic Impact of Upper Gastrointestinal Disorders in the United States: Results of the US Upper Gastrointestinal Study,” Clinical Gastroenterology and Hepatology 3, no. 6 (2005): 543–552, 10.1016/s1542-3565(05)00153-9. [DOI] [PubMed] [Google Scholar]
- 369. Wauters L., Dickman R., Drug V., et al., “United European Gastroenterology (UEG) and European Society for Neurogastroenterology and Motility (ESNM) Consensus on Functional Dyspepsia,” United European Gastroenterology Journal 9, no. 3 (2021): 307–331, 10.1002/ueg2.12061. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 370. Aanpreung P. and Vajaradul C., “Cyclic Vomiting Syndrome in Thai Children,” Medical Journal of the Medical Association of Thailand 85, no. Suppl 2 (2002): S743–S748. [PubMed] [Google Scholar]
- 371. Forbes D., Withers G., Silburn S., and McKelvey R., “Psychological and Social Characteristics and Precipitants of Vomiting in Children With Cyclic Vomiting Syndrome,” Digestive Diseases and Sciences 44, no. 8 Suppl (1999): 19S–22S. [PubMed] [Google Scholar]
- 372. Hejazi R. A., Patil H., and McCallum R. W., “Dumping Syndrome: Establishing Criteria for Diagnosis and Identifying New Etiologies,” Digestive Diseases and Sciences 55, no. 1 (2010): 117–123, 10.1007/s10620-009-0939-5. [DOI] [PubMed] [Google Scholar]
- 373. Abell T. L., Familoni B., Voeller G., et al., “Electrophysiologic, Morphologic, and Serologic Features of Chronic Unexplained Nausea and Vomiting: Lessons Learned From 121 Consecutive Patients,” Surgery 145, no. 5 (2009): 476–485: Epub 20090226, 10.1016/j.surg.2008.12.006. [DOI] [PubMed] [Google Scholar]
- 374. Angeli T. R., Cheng L. K., Du P., et al., “Loss of Interstitial Cells of Cajal and Patterns of Gastric Dysrhythmia in Patients With Chronic Unexplained Nausea and Vomiting,” Gastroenterology 149, no. 1 (2015): 56–66.e5: Epub 20150408, 10.1053/j.gastro.2015.04.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 375. To J., Issenman R. M., and Kamath M. V., “Evaluation of Neurocardiac Signals in Pediatric Patients With Cyclic Vomiting Syndrome through Power Spectral Analysis of Heart Rate Variability,” Journal of Pediatrics 135, no. 3 (1999): 363–366, 10.1016/s0022-3476(99)70135-6. [DOI] [PubMed] [Google Scholar]
- 376. Zhao Y., Ke M., Wang Z., et al., “Pathophysiological and Psychosocial Study in Patients With Functional Vomiting,” J Neurogastroenterol Motil 16, no. 3 (2010): 274–280: Epub 20100726, 10.5056/jnm.2010.16.3.274. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 377. Cavestro C., Montrucchio F., Benci P., et al., “Headache Prevalence and Related Symptoms, Family History, and Treatment Habits in a Representative Population of Children in Alba, Italy,” Pediatric Neurology 51, no. 3 (2014): 348–353: Epub 20140529, 10.1016/j.pediatrneurol.2014.05.022. [DOI] [PubMed] [Google Scholar]
- 378. Hasler W. L. and Chey W. D., “Nausea and Vomiting,” Gastroenterology 125, no. 6 (2003): 1860–1867, 10.1053/j.gastro.2003.09.040. [DOI] [PubMed] [Google Scholar]
- 379. Van Oudenhove L., Levy R. L., Crowell M. D., et al., “Biopsychosocial Aspects of Functional Gastrointestinal Disorders: How Central and Environmental Processes Contribute to the Development and Expression of Functional Gastrointestinal Disorders,” Gastroenterology 150, no. 6 (2016): 1355–1367. e2, 10.1053/j.gastro.2016.02.027. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 380. Levy R. L., Olden K. W., Naliboff B. D., et al., “Psychosocial Aspects of the Functional Gastrointestinal Disorders,” Gastroenterology 130, no. 5 (2006): 1447–1458, 10.1053/j.gastro.2005.11.057. [DOI] [PubMed] [Google Scholar]
- 381. Olden K. W. and Crowell M. D., “Chronic Nausea and Vomiting: New Insights and Approach to Treatment,” Current Treatment Options in Gastroenterology 8, no. 4 (2005): 305–310, 10.1007/s11938-005-0023-y. [DOI] [PubMed] [Google Scholar]
- 382. Kovacic K., Williams S., Li B. U., Chelimsky G., and Miranda A., “High Prevalence of Nausea in Children With Pain‐Associated Functional Gastrointestinal Disorders: Are Rome criteria Applicable?,” Journal of Pediatric Gastroenterology and Nutrition 57, no. 3 (2013): 311–315, 10.1097/MPG.0b013e3182964203. [DOI] [PubMed] [Google Scholar]
- 383. Lacy B. E., Crowell M. D., Mathis C., Bauer D., and Heinberg L. J., “Gastroparesis: Quality of Life and Health Care Utilization,” Journal of Clinical Gastroenterology 52, no. 1 (2018): 20–24, 10.1097/mcg.0000000000000728. [DOI] [PubMed] [Google Scholar]
- 384. Balaban C. D. and Yates B. J., “What Is Nausea? A Historical Analysis of Changing Views,” Autonomic Neuroscience 202 (2017): 5–17: Epub 20160716, 10.1016/j.autneu.2016.07.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 385. Carson D. A., Bhat S., Hayes T. C. L., et al., “Abnormalities on Electrogastrography in Nausea and Vomiting Syndromes: A Systematic Review, Meta‐Analysis, and Comparison to Other Gastric Disorders,” Digestive Diseases and Sciences 67, no. 3 (2022): 773–785: Epub 20210506, 10.1007/s10620-021-07026-x. [DOI] [PubMed] [Google Scholar]
- 386. Wang W. J., Foong D., Calder S., et al., “Gastric Alimetry Expands Patient Phenotyping in Gastroduodenal Disorders Compared With Gastric Emptying Scintigraphy,” American Journal of Gastroenterology 119, no. 2 (2024): 331–341: Epub 20231030, 10.14309/ajg.0000000000002528. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 387. Grover M., Dasari S., Bernard C. E., et al., “Proteomics in Gastroparesis: Unique and Overlapping Protein Signatures in Diabetic and Idiopathic Gastroparesis,” American Journal of Physiology ‐ Gastrointestinal and Liver Physiology 317, no. 5 (2019): G716–G726: Epub 20190904, 10.1152/ajpgi.00115.2019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 388. Chikkamenahalli L. L., Pasricha P. J., Farrugia G., and Grover M., “Gastric Biopsies in Gastroparesis: Insights into Gastric Neuromuscular Disorders to Aid Treatment,” Gastroenterology Clinics of North America 49, no. 3 (2020): 557–570: Epub 20200614, 10.1016/j.gtc.2020.04.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 389. Saleem S., Aziz M., Khan A. A., et al., “Gastric Electrical Stimulation for the Treatment of Gastroparesis or Gastroparesis‐like Symptoms: A Systemic Review and Meta‐Analysis,” Neuromodulation 27, no. 2 (2024): 221–228: Epub 20221202, 10.1016/j.neurom.2022.10.048. [DOI] [PubMed] [Google Scholar]
- 390. Gourcerol G., Huet E., Vandaele N., et al., “Long Term Efficacy of Gastric Electrical Stimulation in Intractable Nausea and Vomiting,” Digestive and Liver Disease 44, no. 7 (2012): 563–568: Epub 20120303, 10.1016/j.dld.2012.01.013. [DOI] [PubMed] [Google Scholar]
- 391. Hedjoudje A., Huet E., Leroi A. M., Desprez C., Melchior C., and Gourcerol G., “Efficacy of Gastric Electrical Stimulation in Intractable Nausea and Vomiting at 10 Years: A Retrospective Analysis of Prospectively Collected Data,” Neuro‐Gastroenterology and Motility 32, no. 11 (2020): e13949: Epub 20200805, 10.1111/nmo.13949. [DOI] [PubMed] [Google Scholar]
- 392. Gottfried‐Blackmore A., Adler E. P., Fernandez‐Becker N., Clarke J., Habtezion A., and Nguyen L., “Open‐label Pilot Study: Non‐invasive Vagal Nerve Stimulation Improves Symptoms and Gastric Emptying in Patients With Idiopathic Gastroparesis,” Neuro‐Gastroenterology and Motility 32, no. 4 (2020): e13769: Epub 20191205, 10.1111/nmo.13769. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 393. Browne P. D., den Hollander B., Speksnijder E. M., et al., “Gut‐directed Hypnotherapy versus Standard Medical Treatment for Nausea in Children With Functional Nausea or Functional Dyspepsia: Protocol of a Multicentre Randomised Trial,” BMJ Open 9, no. 4 (2019): e024903: Epub 20190411, 10.1136/bmjopen-2018-024903. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 394. Browne P. D., de Bruijn C. M. A., Speksnijder E. M., et al., “Skills or Pills: Randomized Trial Comparing Hypnotherapy to Medical Treatment in Children With Functional Nausea,” Clinical Gastroenterology and Hepatology 20, no. 8 (2022): 1847–1856.e6: Epub 20211027, 10.1016/j.cgh.2021.10.029. [DOI] [PubMed] [Google Scholar]
- 395. Kravits K. G., “Hypnosis for the Management of Anticipatory Nausea and Vomiting,” J Adv Pract Oncol 6, no. 3 (2015): 225–229: Epub 20150501, 10.6004/jadpro.2015.6.3.4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 396. Richardson J., Smith J. E., McCall G., Richardson A., Pilkington K., and Kirsch I., “Hypnosis for Nausea and Vomiting in Cancer Chemotherapy: A Systematic Review of the Research Evidence,” European Journal of Cancer Care 16, no. 5 (2007): 402–412, 10.1111/j.1365-2354.2006.00736.x. [DOI] [PubMed] [Google Scholar]
- 397. Ozgoli G. and Saei Ghare Naz M., “Effects of Complementary Medicine on Nausea and Vomiting in Pregnancy: A Systematic Review,” International Journal of Preventive Medicine 9, no. 1 (2018): 75: Epub 20180830, 10.4103/ijpvm.IJPVM_430_16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 398. Brown S., North D., Marvel M. K., and Fons R., “Acupressure Wrist Bands to Relieve Nausea and Vomiting in Hospice Patients: Do They Work?,” Am J Hosp Palliat Care 9, no. 4 (1992): 26–29, 10.1177/104990919200900409. [DOI] [PubMed] [Google Scholar]
- 399. Pan C. X., Morrison R. S., Ness J., Fugh‐Berman A., and Leipzig R. M., “Complementary and Alternative Medicine in the Management of Pain, Dyspnea, and Nausea and Vomiting Near the End of Life. A Systematic Review,” Journal of Pain and Symptom Management 20, no. 5 (2000): 374–387, 10.1016/s0885-3924(00)00190-1. [DOI] [PubMed] [Google Scholar]
- 400. Venkatesan T., Porcelli A., Matapurkar A., et al., “An Integrative Healthcare Model With Heartfulness Meditation and Care Coordination Improves Outcomes in Cyclic Vomiting Syndrome,” Neuro‐Gastroenterology and Motility 33, no. 11 (2021): e14132: Epub 20210328, 10.1111/nmo.14132. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 401. Hasler W. L., “Symptomatic Management for Gastroparesis: Antiemetics, Analgesics, and Symptom Modulators,” Gastroenterology Clinics of North America 44, no. 1 (2015): 113–126: Epub 20141226, 10.1016/j.gtc.2014.11.009. [DOI] [PubMed] [Google Scholar]
- 402. Macario A., Ronquillo R. B., Brose W. G., and Gaeta R. R., “Improved Outcome With Chronic Subcutaneous Infusion of Odansetron for Intractable Nausea and Vomiting,” Anesthesia & Analgesia 83, no. 1 (1996): 194–195, 10.1097/00000539-199607000-00042. [DOI] [PubMed] [Google Scholar]
- 403. Simmons K. and Parkman H. P., “Granisetron Transdermal System Improves Refractory Nausea and Vomiting in Gastroparesis,” Digestive Diseases and Sciences 59, no. 6 (2014): 1231–1234: Epub 20140311, 10.1007/s10620-014-3097-3. [DOI] [PubMed] [Google Scholar]
- 404. Midani D. and Parkman H. P., “Granisetron Transdermal System for Treatment of Symptoms of Gastroparesis: A Prescription Registry Study,” J Neurogastroenterol Motil 22, no. 4 (2016): 650–655, 10.5056/jnm15203. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 405. Patel A., Sayuk G. S., Kushnir V. M., and Gyawali C. P., “Sensory Neuromodulators in Functional Nausea and Vomiting: Predictors of Response,” Postgraduate Medical Journal 89, no. 1049 (2013): 131–136: Epub 20121030, 10.1136/postgradmedj-2012-131284. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 406. Braak B., Klooker T. K., Wouters M. M., Lei A., van den Wijngaard R. M., and Boeckxstaens G. E., “Randomised Clinical Trial: The Effects of Amitriptyline on Drinking Capacity and Symptoms in Patients With Functional Dyspepsia, a Double‐Blind Placebo‐Controlled Study,” Alimentary Pharmacology & Therapeutics 34, no. 6 (2011): 638–648: Epub 20110719, 10.1111/j.1365-2036.2011.04775.x. [DOI] [PubMed] [Google Scholar]
- 407. Malamood M., Roberts A., Kataria R., Parkman H. P., and Schey R., “Mirtazapine for Symptom Control in Refractory Gastroparesis,” Drug Design, Development and Therapy 11 (2017): 1035–1041: Epub 20170330, 10.2147/dddt.S125743. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 408. Cangemi D. J. and Kuo B., “Practical Perspectives in the Treatment of Nausea and Vomiting,” Journal of Clinical Gastroenterology 53, no. 3 (2019): 170–178, 10.1097/mcg.0000000000001164. [DOI] [PubMed] [Google Scholar]
- 409. Tack J., Ly H. G., Carbone F., et al., “Efficacy of Mirtazapine in Patients With Functional Dyspepsia and Weight Loss,” Clinical Gastroenterology and Hepatology 14, no. 3 (2016): 385–392.e4: Epub 20151030, 10.1016/j.cgh.2015.09.043. [DOI] [PubMed] [Google Scholar]
- 410. Gotfried J., Naftali T., and Schey R., “Role of Cannabis and its Derivatives in Gastrointestinal and Hepatic Disease,” Gastroenterology 159, no. 1 (2020): 62–80: Epub 20200422, 10.1053/j.gastro.2020.03.087. [DOI] [PubMed] [Google Scholar]
- 411. Pasricha P. J., Yates K. P., Sarosiek I., et al., “Aprepitant Has Mixed Effects on Nausea and Reduces Other Symptoms in Patients With Gastroparesis and Related Disorders,” Gastroenterology 154, no. 1 (2018): 65–76.e11: Epub 20171028, 10.1053/j.gastro.2017.08.033. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 412. Ashat M., Lewis A., Liaquat H., et al., “Intravenous Immunoglobulin in Drug and Device Refractory Patients With the Symptoms of Gastroparesis‐An Open‐Label Study,” Neuro‐Gastroenterology and Motility 30, no. 3 (2018): Epub 20171204, 10.1111/nmo.13256. [DOI] [PubMed] [Google Scholar]
- 413. Pasricha P. J., McKnight M., Villatoro L., et al., “Joint Hypermobility, Autonomic Dysfunction, Gastrointestinal Dysfunction, and Autoimmune Markers: Clinical Associations and Response to Intravenous Immunoglobulin Therapy,” American Journal of Gastroenterology 119, no. 11 (2024): 2298–2306: Epub 20240724, 10.14309/ajg.0000000000002910. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 414. Parkman H. P., Yates K. P., Hasler W. L., et al., “Dietary Intake and Nutritional Deficiencies in Patients With Diabetic or Idiopathic Gastroparesis,” Gastroenterology 141, no. 2 (2011): 486–498: 98.e1‐7. Epub 20110428, 10.1053/j.gastro.2011.04.045. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 415. Limketkai B. N., LeBrett W., Lin L., and Shah N. D., “Nutritional Approaches for Gastroparesis,” Lancet Gastroenterol Hepatol 5, no. 11 (2020): 1017–1026, 10.1016/s2468-1253(20)30078-9. [DOI] [PubMed] [Google Scholar]
- 416. Homko C. J., Duffy F., Friedenberg F. K., Boden G., and Parkman H. P., “Effect of Dietary Fat and Food Consistency on Gastroparesis Symptoms in Patients With Gastroparesis,” Neuro‐Gastroenterology and Motility 27, no. 4 (2015): 501–508: Epub 20150119, 10.1111/nmo.12519. [DOI] [PubMed] [Google Scholar]
- 417. Hasler W. L., Wilson L. A., Parkman H. P., et al., “Bloating in Gastroparesis: Severity, Impact, and Associated Factors,” American Journal of Gastroenterology 106, no. 8 (2011): 1492–1502: Epub 20110412, 10.1038/ajg.2011.81. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 418. Olausson E. A., Störsrud S., Grundin H., Isaksson M., Attvall S., and Simrén M., “A Small Particle Size Diet Reduces Upper Gastrointestinal Symptoms in Patients With Diabetic Gastroparesis: A Randomized Controlled Trial,” American Journal of Gastroenterology 109, no. 3 (2014): 375–385: Epub 20140114, 10.1038/ajg.2013.453. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supporting Information S1
Supporting Information S2
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.