

Abstract
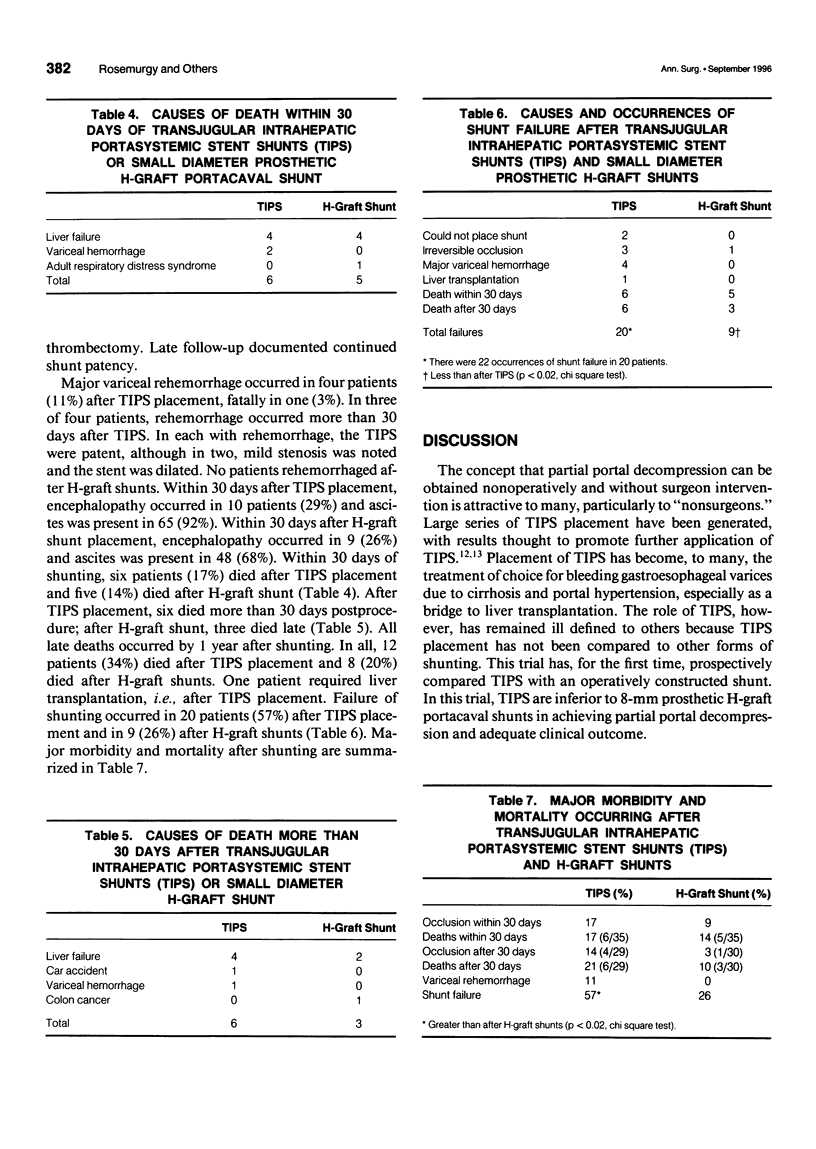
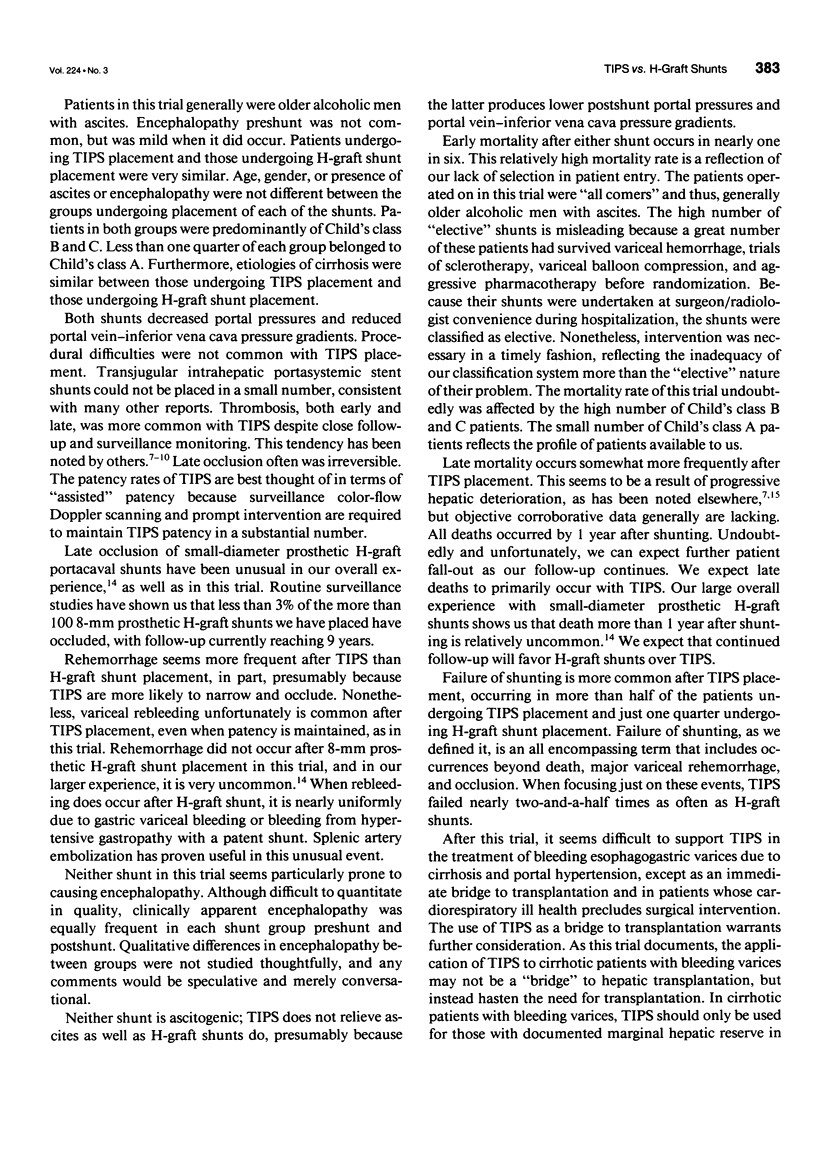
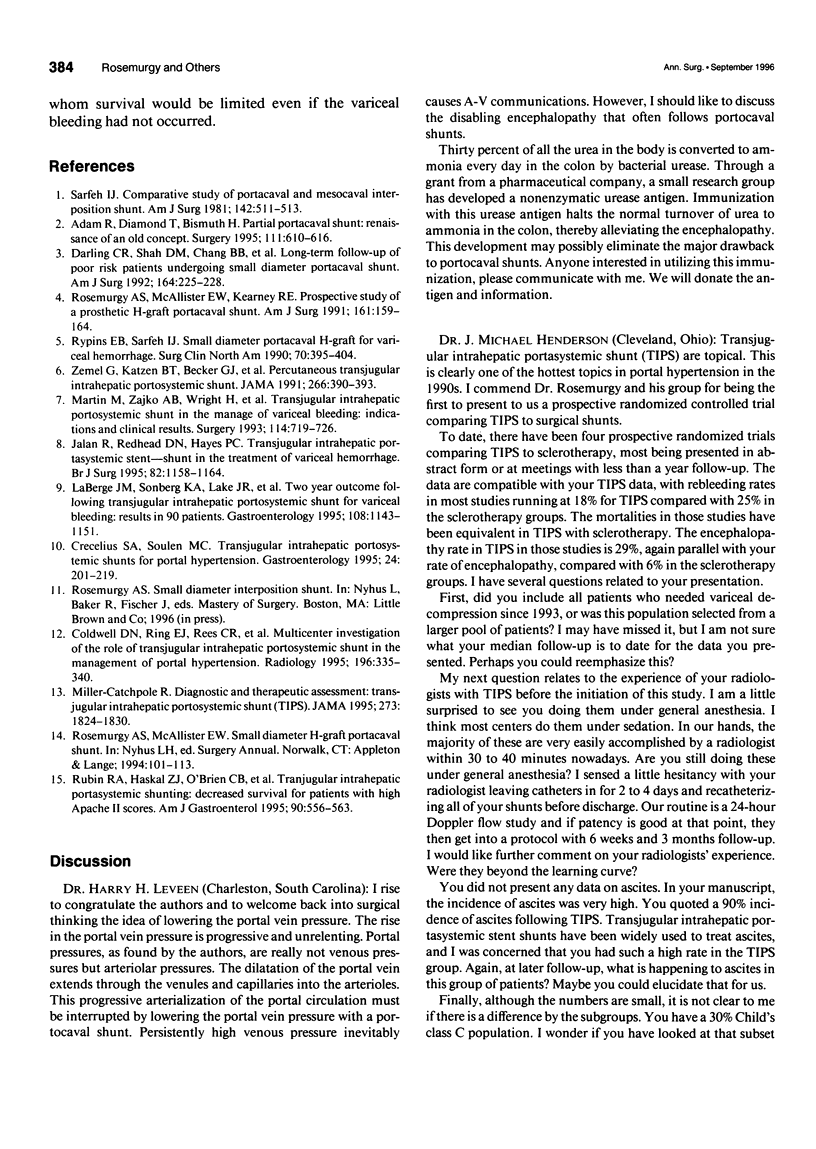
OBJECTIVE: The authors compare transjugular intrahepatic portasystemic stent shunts (TIPS) to small-diameter prosthetic H-graft portacaval shunts (HGPCS). SUMMARY BACKGROUND DATA: Transjugular intrahepatic portasystemic stent shunts have been embraced as a first-line therapy in the treatment of bleeding varices due to portal hypertension, although they have not been compared to operatively placed shunts in a prospective trial. METHODS: In 1993, the authors began a prospective, randomized trial to compare TIPS with HGPCSs. All patients had bleeding varices and had failed nonoperative management. Shunting was undertaken as definitive therapy in all. Failure of shunting was defined as an inability to accomplish shunting despite repeated attempts, unexpected liver failure leading to transplantation, irreversible shunt occlusion, major variceal rehemorrhage, or death. Mortality and failure rates were analyzed at 30 days (early) and after 30 days (late) using Fischer's exact test. RESULTS: There were 35 patients in each group, with no difference in age, gender, Child's class, etiology of cirrhosis, urgency of shunting, or incidence of ascites or encephalopathy between groups. In two patients, TIPS could not be placed despite repeated attempts. Transjugular intrahepatic portasystemic stent shunts reduced portal pressures from 32 +/- 7.5 mmHg (standard deviation) to 25 +/- 7.5 mmHg (p < 0.01), whereas HGPCS reduced them from 30 +/- 4.6 mmHg to 19 +/- 5.3 mmHg (p < 0.01; paired Student's test). Irreversible occlusion occurred in three patients after placement of TIPS. Total failure rate after TIPS placement was 57%; after HGPCS placement, it was 26% (p < 0.02). CONCLUSIONS: Both TIPS and HGPCS reduced portal pressure. Placement of TIPS resulted in more deaths, more rebleeding, and more than twice the treatment failures. Mortality and failure rates promote the application of HGPCS over TIPS.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Adam R., Diamond T., Bismuth H. Partial portacaval shunt: renaissance of an old concept. Surgery. 1992 Jun;111(6):610–616. [PubMed] [Google Scholar]
- Coldwell D. M., Ring E. J., Rees C. R., Zemel G., Darcy M. D., Haskal Z. J., McKusick M. A., Greenfield A. J. Multicenter investigation of the role of transjugular intrahepatic portosystemic shunt in management of portal hypertension. Radiology. 1995 Aug;196(2):335–340. doi: 10.1148/radiology.196.2.7617842. [DOI] [PubMed] [Google Scholar]
- Crecelius S. A., Soulen M. C. Transjugular intrahepatic portosystemic shunts for portal hypertension. Gastroenterol Clin North Am. 1995 Jun;24(2):201–219. [PubMed] [Google Scholar]
- Darling R. C., 3rd, Shah D. M., Chang B. B., Thompson P. N., Leather R. P. Long-term follow-up of poor-risk patients undergoing small-diameter portacaval shunts. Am J Surg. 1992 Sep;164(3):225–228. doi: 10.1016/s0002-9610(05)81075-x. [DOI] [PubMed] [Google Scholar]
- Jalan R., Redhead D. N., Hayes P. C. Transjugular intrahepatic portasystemic stent-shunt in the treatment of variceal haemorrhage. Br J Surg. 1995 Sep;82(9):1158–1164. doi: 10.1002/bjs.1800820905. [DOI] [PubMed] [Google Scholar]
- LaBerge J. M., Somberg K. A., Lake J. R., Gordon R. L., Kerlan R. K., Jr, Ascher N. L., Roberts J. P., Simor M. M., Doherty C. A., Hahn J. Two-year outcome following transjugular intrahepatic portosystemic shunt for variceal bleeding: results in 90 patients. Gastroenterology. 1995 Apr;108(4):1143–1151. doi: 10.1016/0016-5085(95)90213-9. [DOI] [PubMed] [Google Scholar]
- Martin M., Zajko A. B., Orons P. D., Dodd G., Wright H., Colangelo J., Tartar R. Transjugular intrahepatic portosystemic shunt in the management of variceal bleeding: indications and clinical results. Surgery. 1993 Oct;114(4):719–727. [PubMed] [Google Scholar]
- Miller-Catchpole R. Diagnostic and therapeutic technology assessment. Transjugular intrahepatic portosystemic shunt (TIPS). JAMA. 1995 Jun 21;273(23):1824–1830. [PubMed] [Google Scholar]
- Rosemurgy A. S., McAllister E. W., Kearney R. E. Prospective study of a prosthetic H-graft portacaval shunt. Am J Surg. 1991 Jan;161(1):159–164. doi: 10.1016/0002-9610(91)90378-q. [DOI] [PubMed] [Google Scholar]
- Rubin R. A., Haskal Z. J., O'Brien C. B., Cope C., Brass C. A. Transjugular intrahepatic portosystemic shunting: decreased survival for patients with high APACHE II scores. Am J Gastroenterol. 1995 Apr;90(4):556–563. [PubMed] [Google Scholar]
- Rypins E. B., Sarfeh I. J. Small-diameter portacaval H-graft for variceal hemorrhage. Surg Clin North Am. 1990 Apr;70(2):395–404. doi: 10.1016/s0039-6109(16)45088-7. [DOI] [PubMed] [Google Scholar]
- Sarfeh I. J. Comparative study of portacaval and mesocaval interposition shunts. Am J Surg. 1981 Oct;142(4):511–513. doi: 10.1016/0002-9610(81)90386-x. [DOI] [PubMed] [Google Scholar]
- Zemel G., Katzen B. T., Becker G. J., Benenati J. F., Sallee D. S. Percutaneous transjugular portosystemic shunt. JAMA. 1991 Jul 17;266(3):390–393. [PubMed] [Google Scholar]