

Abstract
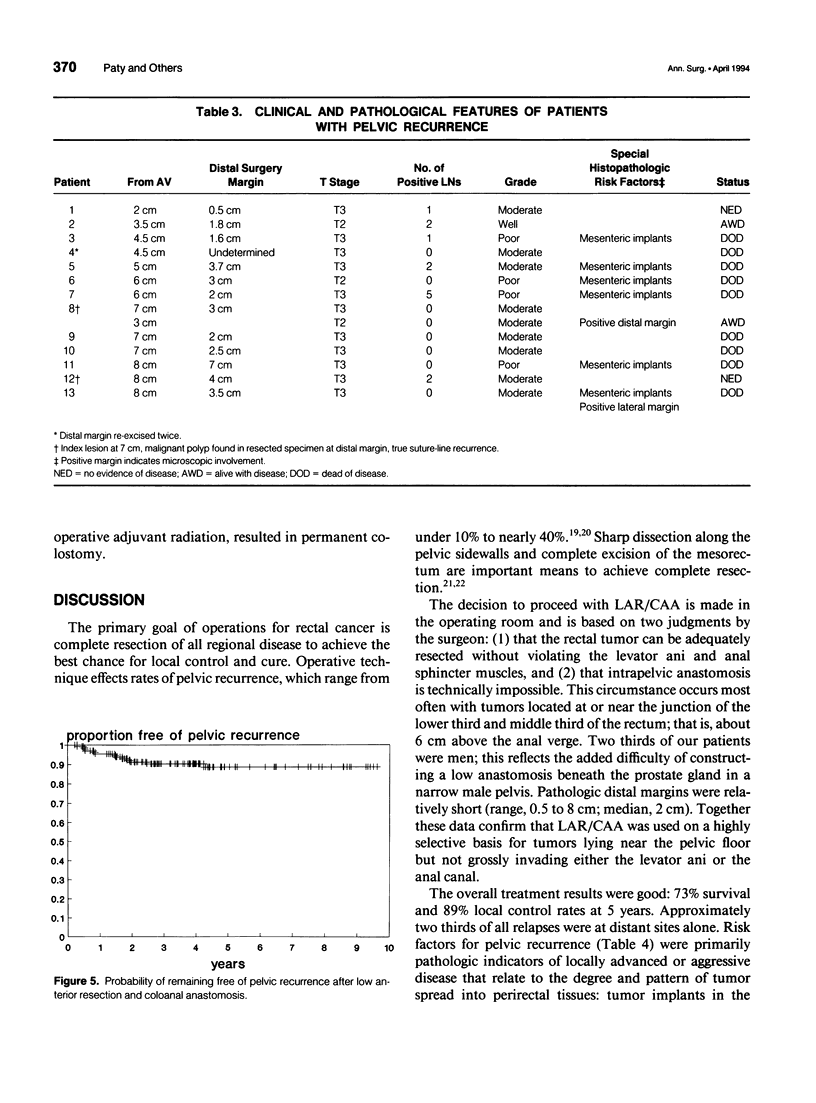
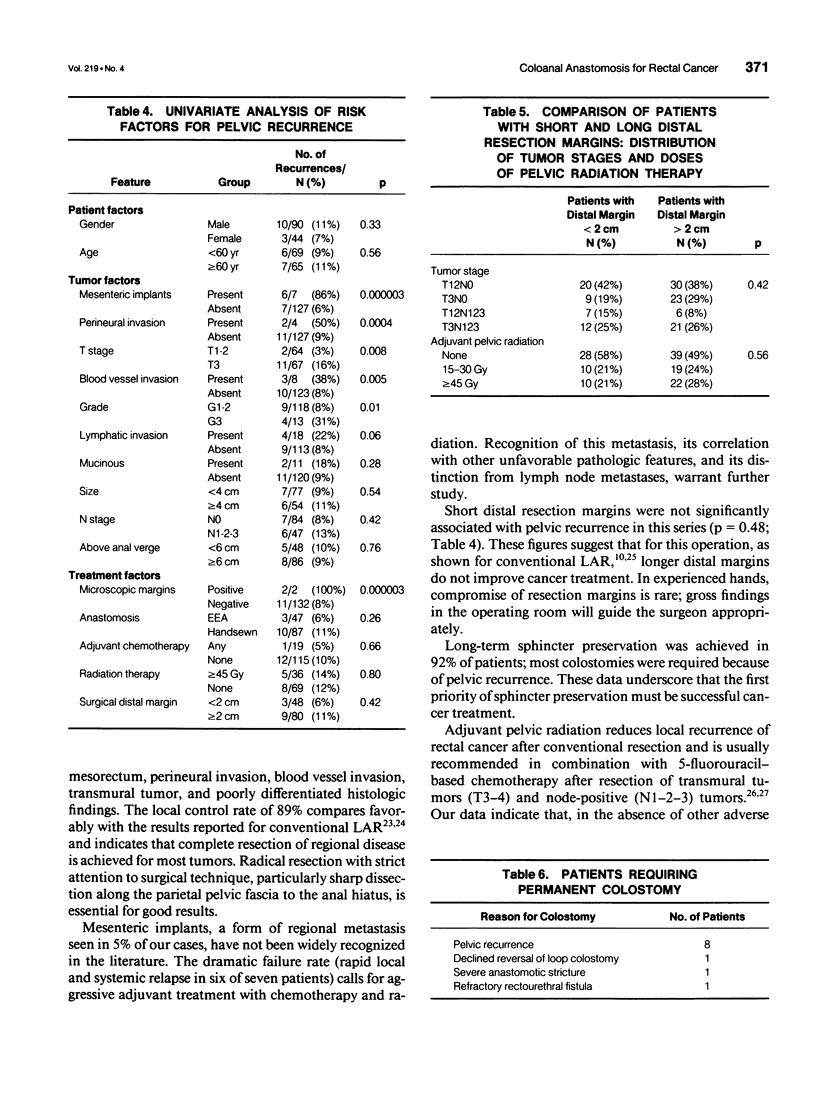
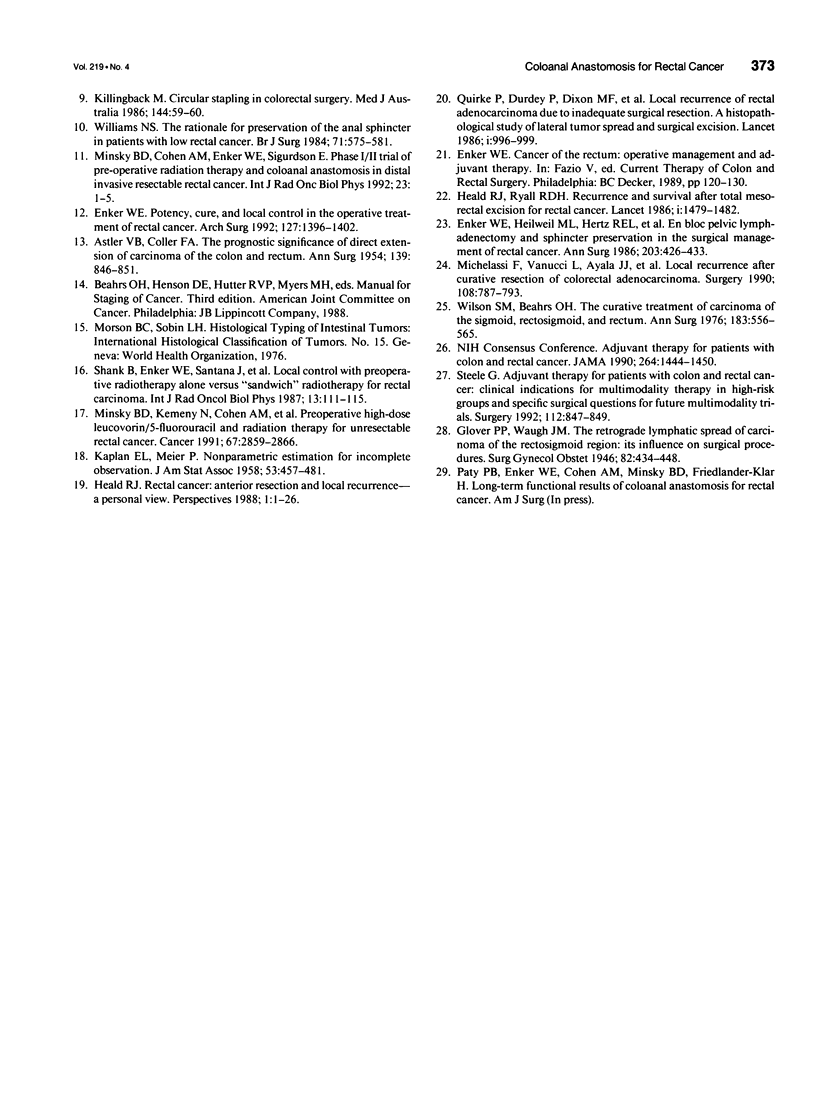
OBJECTIVE: Our institution's experience with low anterior resection in combination with coloanal anastomosis (LAR/CAA) for primary rectal cancer was reviewed (1) to determine cancer treatment results, 2) to identify risk factors for pelvic recurrence, and 3) to assess the long-term success of sphincter preservation. SUMMARY BACKGROUND DATA: Use of sphincter-preserving resection for mid-rectal and selected distal-rectal cancers continues to increase. As surgical techniques and adjuvant therapy evolve, treatment results must be carefully assessed. METHODS: One hundred thirty-four patients treated for primary rectal cancer by LAR/CAA between 1977 and 1990 were studied retrospectively. All pathologic slides were reviewed. Median follow-up was 4 years. RESULTS: Actuarial 5-year survival for all patients was 73%. Among 36 patients who relapsed, distant metastatic disease had developed at the time of first clinical relapse in most (86%). Pelvic recurrence was detected in 13 patients, an actuarial rate of 11% at 5 years. Mesenteric implants, positive microscopic resection margin, T3 tumor, perineural invasion, blood vessel invasion, and high tumor grade were associated with increased risk for pelvic recurrence. Eleven patients ultimately required permanent colostomy, and in eight instances the cause was pelvic recurrence. CONCLUSIONS: Low anterior resection combined with coloanal anastomosis provides good treatment for mid-rectal cancers and for some distal rectal cancers. Pelvic recurrence is not associated with short distal resection margins but is correlated with the presence of histopathologic markers of aggressive disease in the primary tumor. Long-term preservation of anal sphincter function depends primarily on control of pelvic tumor and can be achieved in more than 90% of patients.
Full text
PDF

Images in this article

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- ASTLER V. B., COLLER F. A. The prognostic significance of direct extension of carcinoma of the colon and rectum. Ann Surg. 1954 Jun;139(6):846–852. doi: 10.1097/00000658-195406000-00015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cohen A. M., Enker W. E., Minsky B. D. Proctectomy and coloanal reconstruction for rectal cancer. Dis Colon Rectum. 1990 Jan;33(1):40–43. doi: 10.1007/BF02053200. [DOI] [PubMed] [Google Scholar]
- Enker W. E., Pilipshen S. J., Heilweil M. L., Stearns M. W., Jr, Janov A. J., Hertz R. E., Sternberg S. S. En bloc pelvic lymphadenectomy and sphincter preservation in the surgical management of rectal cancer. Ann Surg. 1986 Apr;203(4):426–433. doi: 10.1097/00000658-198604000-00015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Enker W. E. Potency, cure, and local control in the operative treatment of rectal cancer. Arch Surg. 1992 Dec;127(12):1396–1402. doi: 10.1001/archsurg.1992.01420120030005. [DOI] [PubMed] [Google Scholar]
- Enker W. E., Stearns M. W., Jr, Janov A. J. Peranal coloanal anastomosis following low anterior resection for rectal carcinoma. Dis Colon Rectum. 1985 Aug;28(8):576–581. doi: 10.1007/BF02554147. [DOI] [PubMed] [Google Scholar]
- Hautefeuille P., Valleur P., Perniceni T., Martin B., Galian A., Cherqui D., Hoang C. Functional and oncologic results after coloanal anastomosis for low rectal carcinoma. Ann Surg. 1988 Jan;207(1):61–64. doi: 10.1097/00000658-198801000-00012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Heald R. J., Leicester R. J. The low stapled anastomosis. Dis Colon Rectum. 1981 Sep;24(6):437–444. doi: 10.1007/BF02626778. [DOI] [PubMed] [Google Scholar]
- Heald R. J., Ryall R. D. Recurrence and survival after total mesorectal excision for rectal cancer. Lancet. 1986 Jun 28;1(8496):1479–1482. doi: 10.1016/s0140-6736(86)91510-2. [DOI] [PubMed] [Google Scholar]
- Holt L. B. Acid intoxication theory of scurvy. Proc R Soc Med. 1972 Jan;65(1):47–48. [PMC free article] [PubMed] [Google Scholar]
- Killingback M. Circular stapling in colorectal surgery. Med J Aust. 1986 Jan 20;144(2):59–60. doi: 10.5694/j.1326-5377.1986.tb113658.x. [DOI] [PubMed] [Google Scholar]
- Lazorthes F., Fages P., Chiotasso P., Bugat R. Synchronous abdominotrans-sphincteric resection of low rectal cancer: new technique for direct colo-anal anastomosis. Br J Surg. 1986 Jul;73(7):573–575. doi: 10.1002/bjs.1800730720. [DOI] [PubMed] [Google Scholar]
- Marks G., Mohiuddin M., Goldstein S. D. Sphincter preservation for cancer of the distal rectum using high dose preoperative radiation. Int J Radiat Oncol Biol Phys. 1988 Nov;15(5):1065–1068. doi: 10.1016/0360-3016(88)90185-x. [DOI] [PubMed] [Google Scholar]
- Michelassi F., Vannucci L., Ayala J. J., Chappel R., Goldberg R., Block G. E. Local recurrence after curative resection of colorectal adenocarcinoma. Surgery. 1990 Oct;108(4):787–793. [PubMed] [Google Scholar]
- Minsky B. D., Kemeny N., Cohen A. M., Enker W. E., Kelsen D. P., Reichman B., Saltz L., Sigurdson E. R., Frankel J. Preoperative high-dose leucovorin/5-fluorouracil and radiation therapy for unresectable rectal cancer. Cancer. 1991 Jun 1;67(11):2859–2866. doi: 10.1002/1097-0142(19910601)67:11<2859::aid-cncr2820671126>3.0.co;2-w. [DOI] [PubMed] [Google Scholar]
- Parks A. G., Percy J. P. Resection and sutured colo-anal anastomosis for rectal carcinoma. Br J Surg. 1982 Jun;69(6):301–304. doi: 10.1002/bjs.1800690602. [DOI] [PubMed] [Google Scholar]
- Quirke P., Durdey P., Dixon M. F., Williams N. S. Local recurrence of rectal adenocarcinoma due to inadequate surgical resection. Histopathological study of lateral tumour spread and surgical excision. Lancet. 1986 Nov 1;2(8514):996–999. doi: 10.1016/s0140-6736(86)92612-7. [DOI] [PubMed] [Google Scholar]
- Shank B., Enker W., Santana J., Morrissey K., Daly J., Quan S., Knapper W. Local control with pre-operative radiotherapy alone versus "sandwich" radiotherapy for rectal carcinoma. Int J Radiat Oncol Biol Phys. 1987 Jan;13(1):111–115. doi: 10.1016/0360-3016(87)90267-7. [DOI] [PubMed] [Google Scholar]
- Steele G., Jr Adjuvant therapy for patients with colon and rectal cancer: clinical indications for multimodality therapy in high-risk groups and specific surgical questions for future multimodality trials. Surgery. 1992 Nov;112(5):847–849. [PubMed] [Google Scholar]
- Williams N. S. The rationale for preservation of the anal sphincter in patients with low rectal cancer. Br J Surg. 1984 Aug;71(8):575–581. doi: 10.1002/bjs.1800710802. [DOI] [PubMed] [Google Scholar]
- Wilson S. M., Beahrs O. H. The curative treatment of carcinoma of the sigmoid, rectosigmoid, and rectum. Ann Surg. 1976 May;183(5):556–565. doi: 10.1097/00000658-197605000-00013. [DOI] [PMC free article] [PubMed] [Google Scholar]