

Abstract
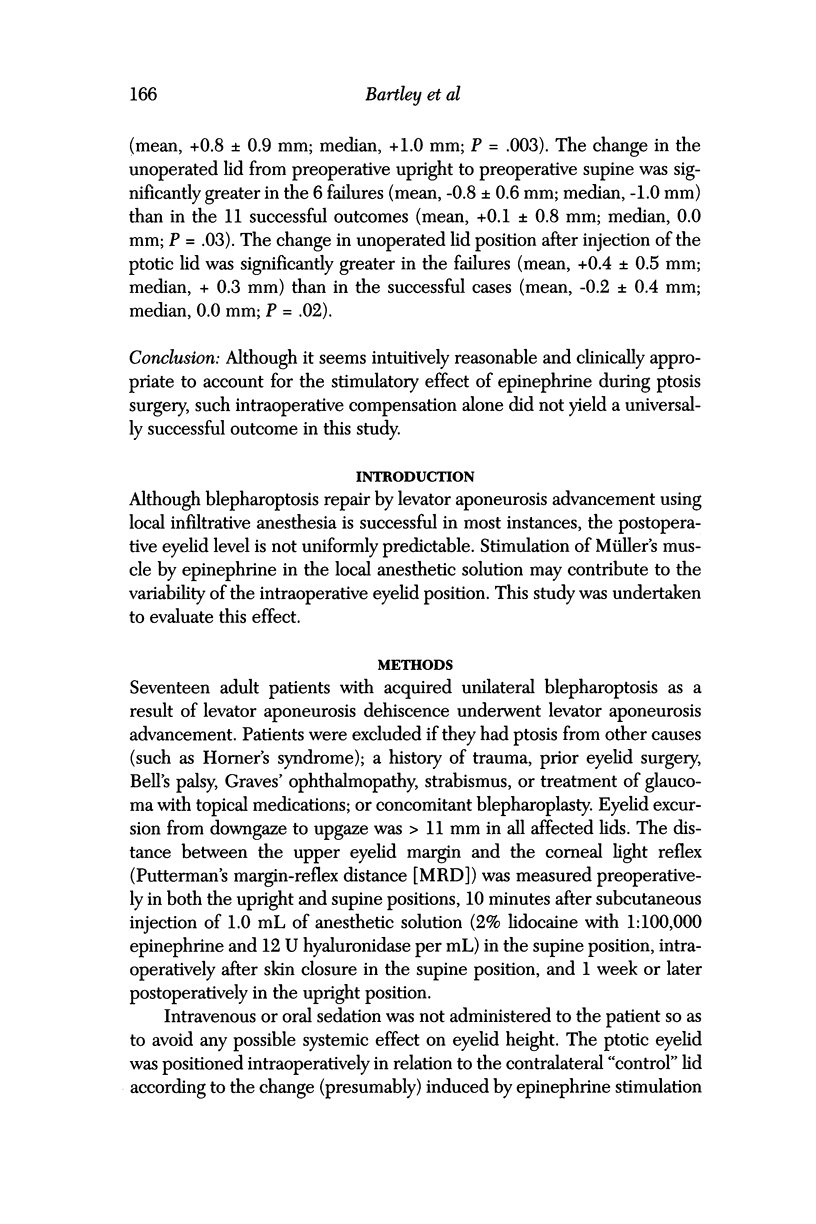
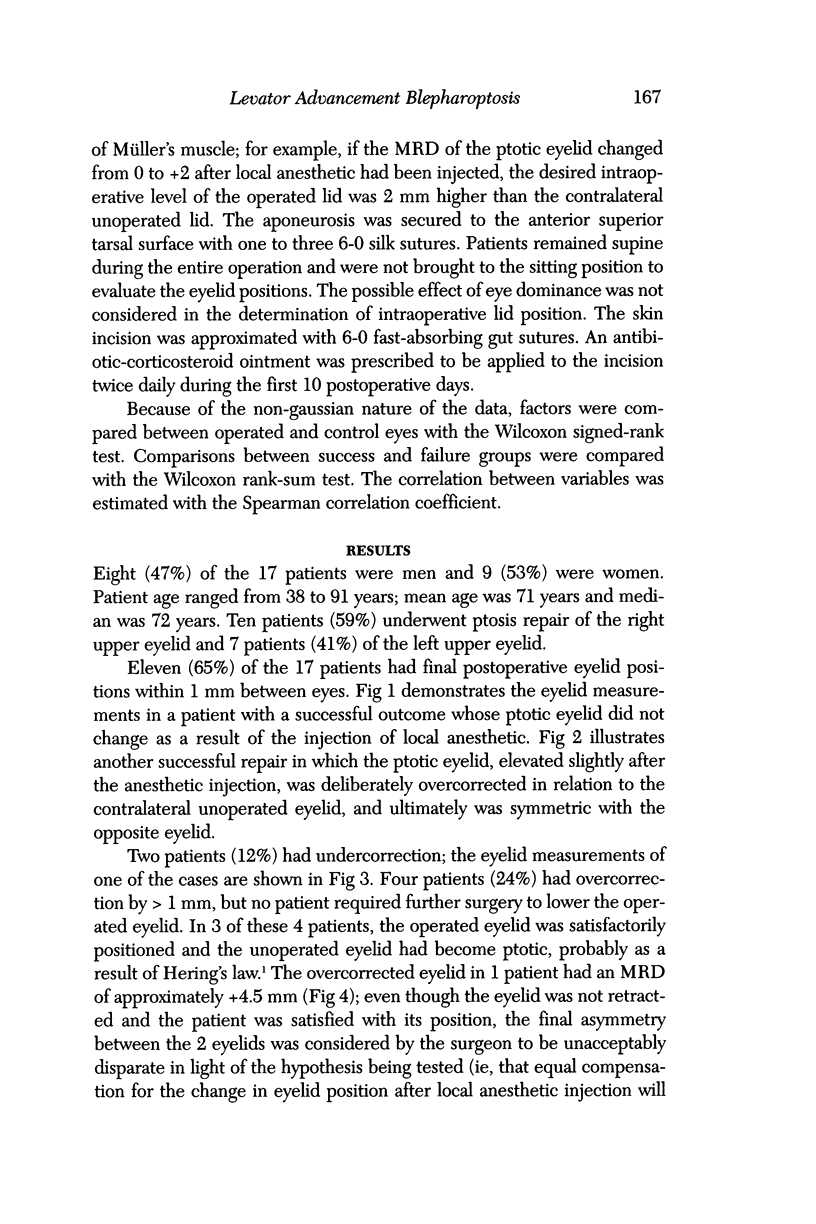
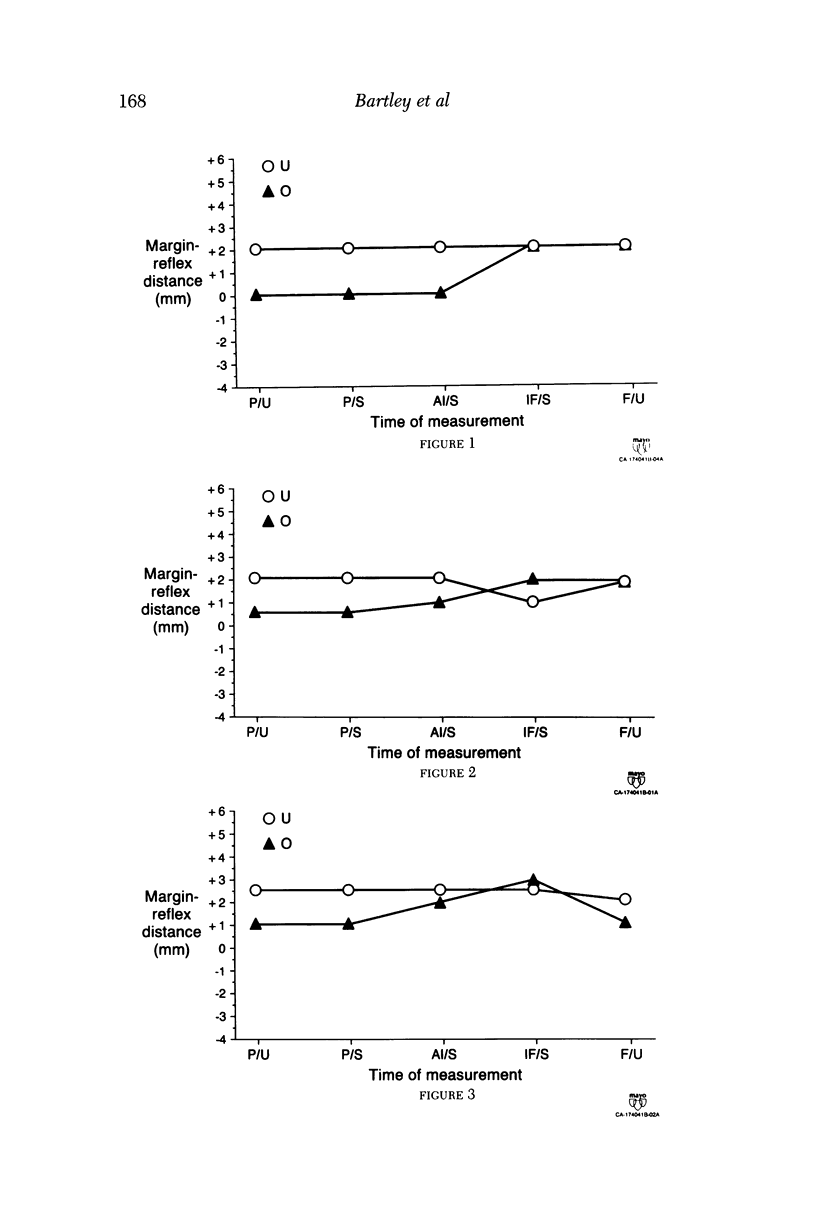
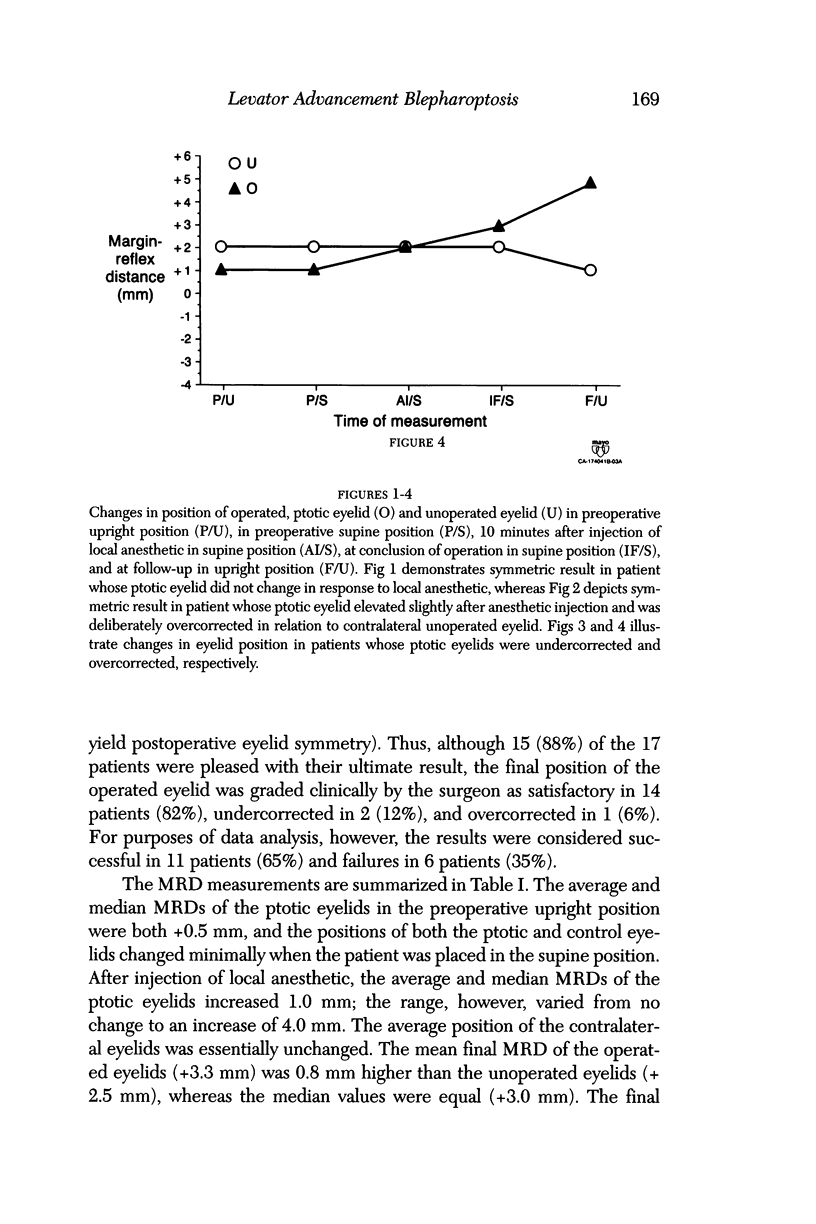
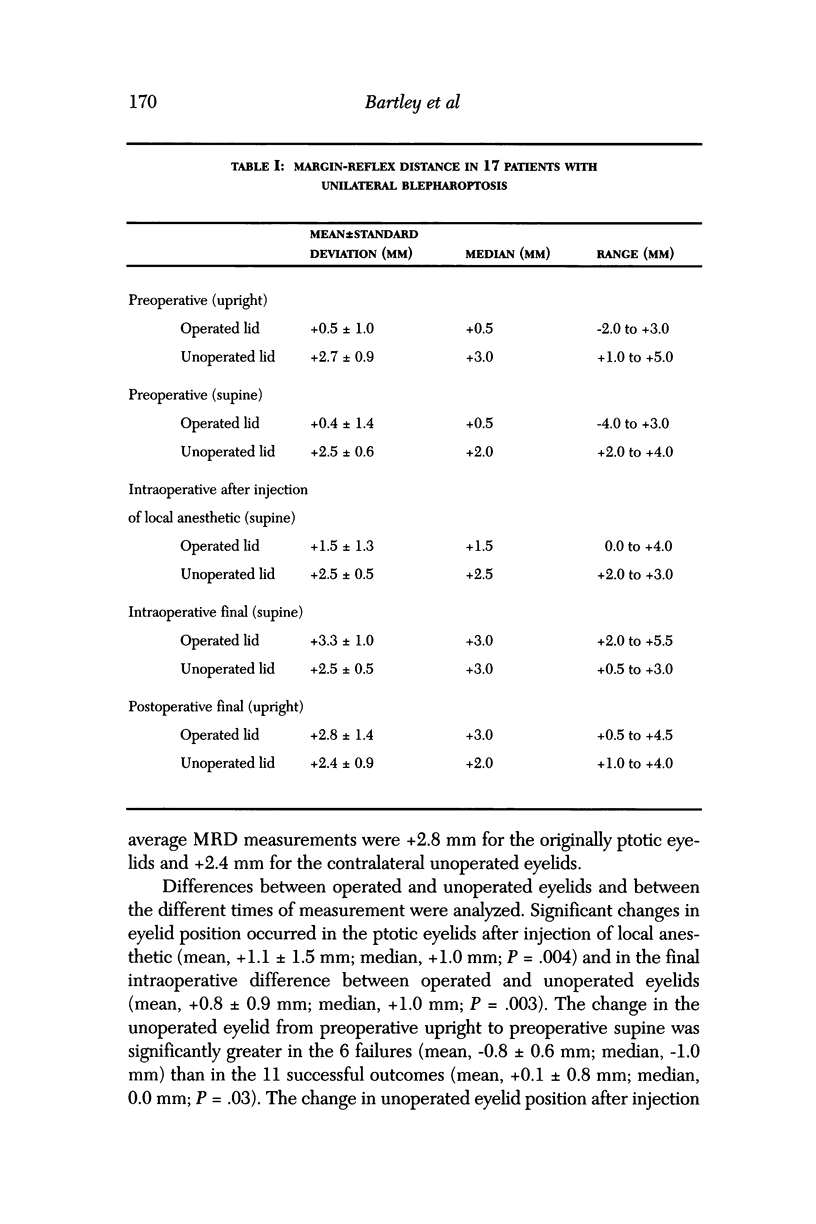
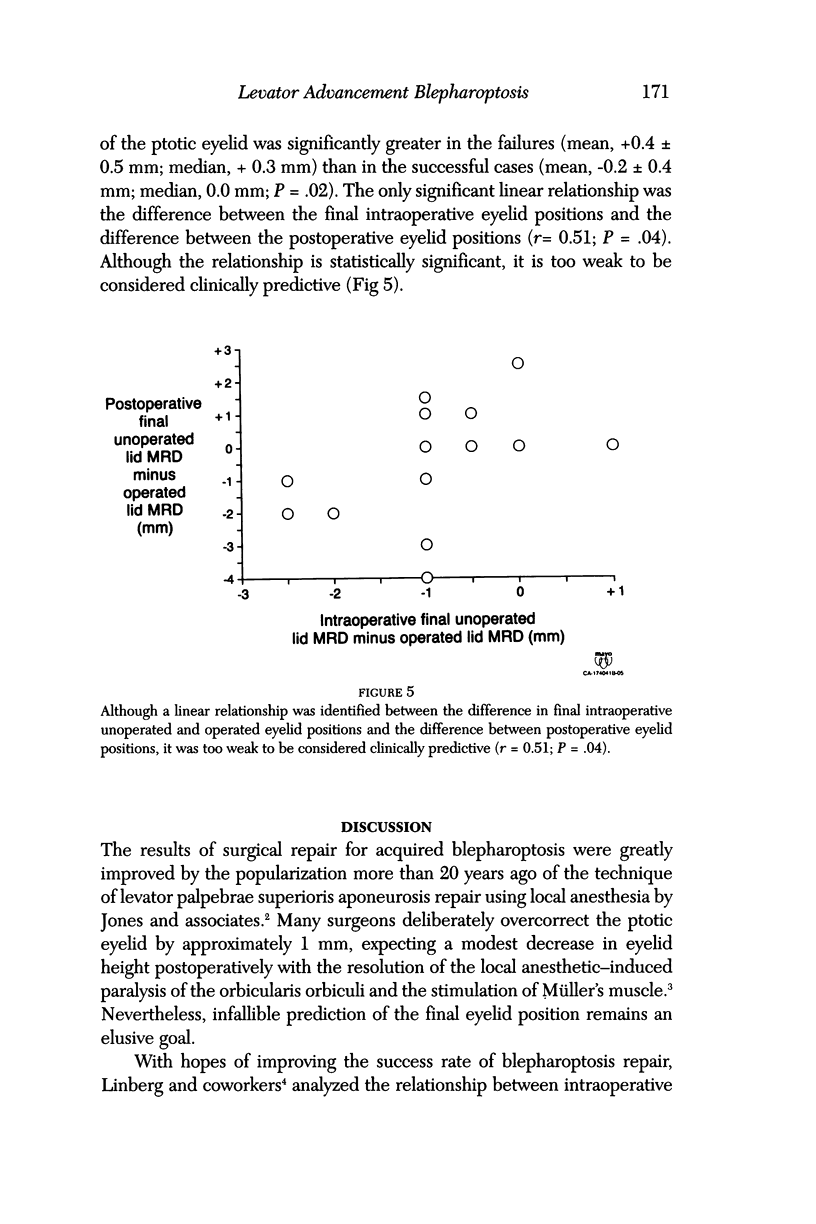
PURPOSE: Blepharoptosis repair by levator advancement is successful in most instances, but the postoperative eyelid level is not uniformly predictable. This study was undertaken to evaluate the possible effect of epinephrine (from local anesthetic) on eyelid position. METHODS: Seventeen adults with acquired unilateral ptosis as a result of levator aponeurosis dehiscence underwent levator aponeurosis advancement. The distance between the upper eyelid margin and the central corneal light reflex was measured preoperatively with the patient in both the upright and the supine position, 10 minutes after injection of 1.0 mL of anesthetic solution (2% lidocaine with 1:100,000 epinephrine and 12 U hyaluronidase per mL) in the supine position, intraoperatively after skin closure in the supine position, and 1 week or more postoperatively in the upright position. The ptotic lid was positioned intraoperatively in relation to the contralateral unoperated lid according to the change (presumably) induced by epinephrine stimulation of Müller's muscle. RESULTS: Eleven (65%) of the 17 patients had final postoperative lid positions within 1 mm between eyes. Two patients (12%) had undercorrection. Four patients (24%) had overcorrection by > 1 mm. The overcorrected lids were satisfactorily positioned, however, and none required further surgery; in 3 of these 4 patients, the unoperated lid had become ptotic, probably as a result of Hering's law. Differences between operated and unoperated lids and between the different times of measurement were analyzed. Significant changes in lid position occurred in the ptotic lids after injection (mean, +1.1 +/- 1.5 mm; median, +1.0 mm; P = .004) and in the final intraoperative difference between operated and unoperated lids (mean, +0.8 +/- 0.9 mm; median, +1.0 mm; P = .003). The change in the unoperated lid from preoperative upright to preoperative supine was significantly greater in the 6 failures (mean, -0.8 +/- 0.6 mm; median, -1.0 mm) than in the 11 successful outcomes (mean, +0.1 +/- 0.8 mm; median, 0.0 mm; P = .03). The change in unoperated lid position after injection of the ptotic lid was significantly greater in the failures (mean, +0.4 +/- 0.5 mm; median, +0.3 mm) than in the successful cases (mean, -0.2 +/- 0.4 mm; median, 0.0 mm; P = .02). CONCLUSION: Although it seems intuitively reasonable and clinically appropriate to account for the stimulatory effect of epinephrine during ptosis surgery, such intraoperative compensation alone did not yield a universally successful outcome in this study.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Anderson R. L., Dixon R. S. Aponeurotic ptosis surgery. Arch Ophthalmol. 1979 Jun;97(6):1123–1128. doi: 10.1001/archopht.1979.01020010577015. [DOI] [PubMed] [Google Scholar]
- Berlin A. J., Vestal K. P. Levator aponeurosis surgery. A retrospective review. Ophthalmology. 1989 Jul;96(7):1033–1037. [PubMed] [Google Scholar]
- Bodian M. Lip droop following contralateral ptosis repair. Arch Ophthalmol. 1982 Jul;100(7):1122–1124. doi: 10.1001/archopht.1982.01030040100018. [DOI] [PubMed] [Google Scholar]
- Dortzbach R. K., Kronish J. W. Early revision in the office for adults after unsatisfactory blepharoptosis correction. Am J Ophthalmol. 1993 Jan;115(1):68–75. doi: 10.1016/s0002-9394(14)73527-5. [DOI] [PubMed] [Google Scholar]
- Jones L. T., Quickert M. H., Wobig J. L. The cure of ptosis by aponeurotic repair. Arch Ophthalmol. 1975 Aug;93(8):629–634. doi: 10.1001/archopht.1975.01010020601008. [DOI] [PubMed] [Google Scholar]
- Jordan D. R., Anderson R. L. A simple procedure for adjusting eyelid position after aponeurotic ptosis surgery. Arch Ophthalmol. 1987 Sep;105(9):1288–1291. doi: 10.1001/archopht.1987.01060090146046. [DOI] [PubMed] [Google Scholar]
- Linberg J. V., Vasquez R. J., Chao G. M. Aponeurotic ptosis repair under local anesthesia. Prediction of results from operative lid height. Ophthalmology. 1988 Aug;95(8):1046–1052. doi: 10.1016/s0161-6420(88)33060-5. [DOI] [PubMed] [Google Scholar]
- Lyon D. B., Gonnering R. S., Dortzbach R. K., Lemke B. N. Unilateral ptosis and eye dominance. Ophthal Plast Reconstr Surg. 1993 Dec;9(4):237–240. doi: 10.1097/00002341-199312000-00002. [DOI] [PubMed] [Google Scholar]
- Meyer D. R., Wobig J. L. Detection of contralateral eyelid retraction associated with blepharoptosis. Ophthalmology. 1992 Mar;99(3):366–375. doi: 10.1016/s0161-6420(92)31963-3. [DOI] [PubMed] [Google Scholar]
- Older J. J. Levator aponeurosis surgery for the correction of acquired ptosis. Analysis of 113 procedures. Ophthalmology. 1983 Sep;90(9):1056–1059. doi: 10.1016/s0161-6420(83)80047-5. [DOI] [PubMed] [Google Scholar]