
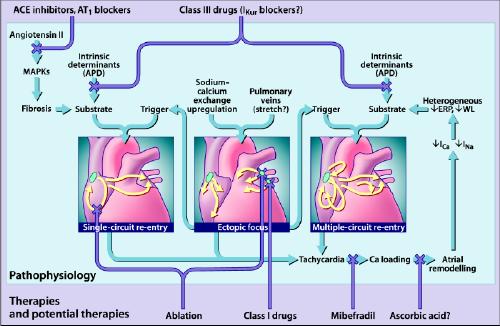
Fig. 1: The primary mechanisms believed to underlie atrial fibrillation (AF) (for detailed discussions, see references 14 and 81). AF may be maintained by rapidly discharging atrial ectopic foci, by a single, rapidly firing atrial re-entry circuit or by multiple functional re-entry circuits. Re-entry mechanisms require both a favourable substrate that can support re-entry and a trigger mechanism to initiate re-entry. The triggers are generally provided by atrial ectopic activity, often originating in the pulmonary veins. The substrate can be produced by angiotensin activation of mitogen-activated protein kinases (MAPKs) that cause tissue fibrosis, or by atrial tachycardia itself, which causes Ca2+ overloading followed by altered atrial electrical properties (“atrial remodelling”), including spatially heterogeneous reductions in effective refractory period (ERP) that promote multiple-circuit re-entry. Ectopic foci can promote single-circuit re-entry by providing triggers for re-entry induction and can promote multiple-circuit re-entry both by causing tachycardias that cause atrial remodelling and by providing triggers for re-entry induction. Single-circuit re-entry can lead to multiple-circuit re-entry by causing atrial remodelling. Both single-circuit re-entry and multiple-circuit re-entry can promote ectopic activity, perhaps by causing Ca2+-loading that favours the occurrence of triggered activity. Thus, the 3 mechanisms shown are not independent but can each play a role in the occurrence of the other. The Xs show potential sites of therapeutic intervention, which can be individualized to the pathophysiology in each patient. Targeted tissue destruction (ablation) can be used to destroy key points in a re-entry circuit or ectopic foci. Angiotensin antagonists (angiotensin-converting-enzyme [ACE] inhibitors or angiotensin-1 receptor blockers [AT1]) may be able to prevent arrhythmogenic fibrosis. The Ca2+ antagonist mibefradil, or possibly even ascorbic acid, may be effective in preventing atrial remodelling. Class III drugs, possibly even atrial-selective agents that target atrial-specific channels like the ultra-rapid potassium current (IKur), may be used to prolong action potential duration (APD) and prevent re-entry. WL = wavelength. Photo: Lianne Friesen and Nicholas Woolridge