

Abstract
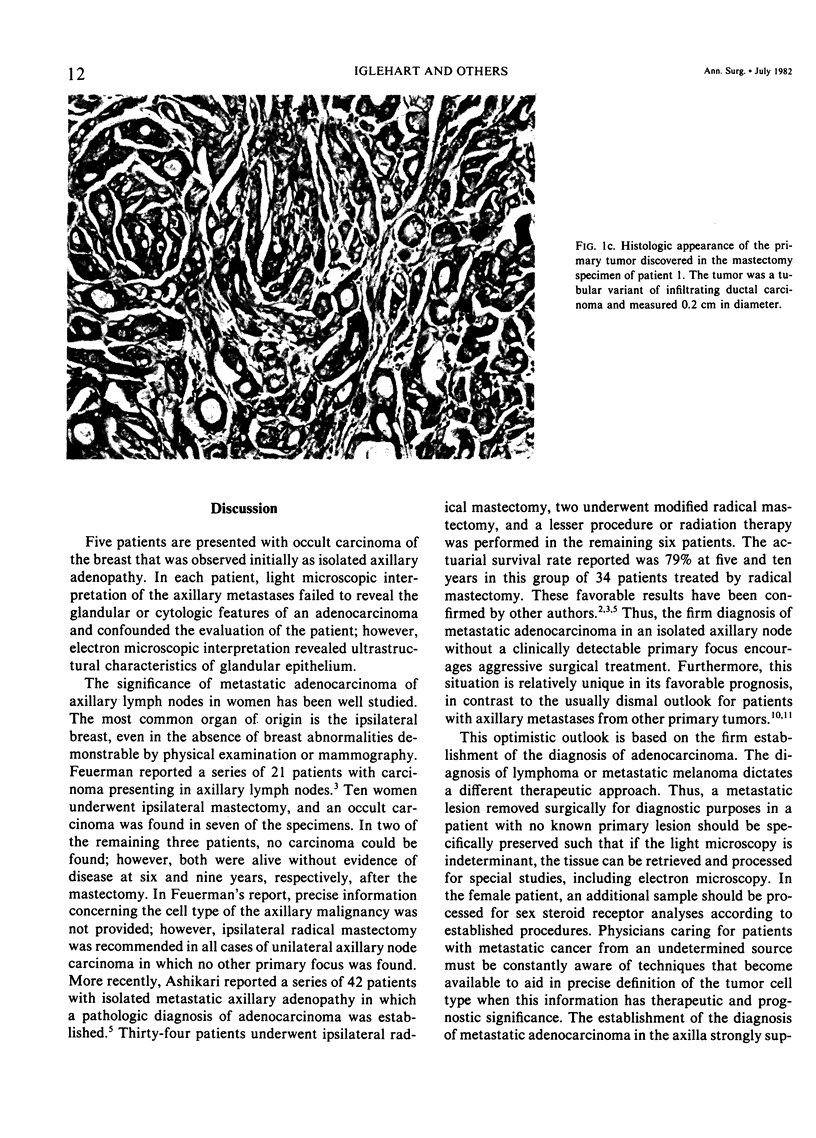
Metastatic adenocarcinoma in the axillary lymph nodes of a female patient often originates from a primary tumor in the ipsilateral breast. Mastectomy may be recommended if adenocarcinoma is found in the axillary nodes even when the primary tumor is not clinically detectable. In these circumstances, the recommendation for mastectomy should be based on the firm histologic diagnosis of adenocarcinoma. In the present report, five female patients are discussed who presented with axillary lymphadenopathy without clinically evident breast masses or mammographic evidence of malignancy. Axillary lymph node biopsies, performed in each patient, were inconclusive after conventional light microscopic examination. Electron microscopy established the diagnosis of adenocarcinoma. These findings were complemented by sex steroid analyses of the tumors where possible. Each patient underwent ipsilateral mastectomy, and in each specimen an occult breast carcinoma was found. The necessity of making a precise tissue diagnosis in all cases of metastatic cancer from an unknown primary is stressed, and special techniques to accomplish this must be considered preoperatively. This is particularly important in the female patient with metastatic breast carcinoma in an isolated axillary lymph node, since ipsilateral mastectomy may be curative.
Full text
PDF
Images in this article
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Ashikari R., Rosen P. P., Urban J. A., Senoo T. Breast cancer presenting as an axillary mass. Ann Surg. 1976 Apr;183(4):415–417. doi: 10.1097/00000658-197604000-00015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- DOCKERTY M. B., GRAY H. K., PIERCE E. H. Surgical significance of isolated axillary adenopathy. Ann Surg. 1957 Jan;145(1):104–107. doi: 10.1097/00000658-195701000-00011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- FEUERMAN L., ATTIE J. N., ROSENBERG B. Carcinoma in axillary lymph nodes as an indicator of breast cancer. Surg Gynecol Obstet. 1962 Jan;114:5–8. [PubMed] [Google Scholar]
- Kesterson G. H., Georgiade N., Seigler H. F., Barton T. K., McCarty K. S., Sr, McCarty K. S., Jr Cystosarcoma phylloides. A steroid receptor and ultrastructure analysis. Ann Surg. 1979 Nov;190(5):640–647. doi: 10.1097/00000658-197911000-00014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kiang D. T., Kennedy B. J. Estrogen receptor assay in the differential diagnosis of adenocarcinomas. JAMA. 1977 Jul 4;238(1):32–34. [PubMed] [Google Scholar]
- Krementz E. T., Cerise E. J., Ciaravella J. M., Jr, Morgan L. R. Metastases of undetermined source. CA Cancer J Clin. 1977 Sep-Oct;27(5):289–300. doi: 10.3322/canjclin.27.5.289. [DOI] [PubMed] [Google Scholar]
- Seiger H. F., Shingleton W. W., Metzgar R. S., Buckley C. E., 3rd Immunotherapy in patients with melanoma. Ann Surg. 1973 Sep;178(3):352–359. doi: 10.1097/00000658-197309000-00015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Smith P. E., Krementz E. T., Chapman W. Metastatic cancer without a detectable primary site. Am J Surg. 1967 May;113(5):633–637. doi: 10.1016/0002-9610(67)90309-1. [DOI] [PubMed] [Google Scholar]
- Stewart J. F., Tattersall M. H., Woods R. L., Fox R. M. Unknown primary adenocarcinoma: incidence of overinvestigation and natural history. Br Med J. 1979 Jun 9;1(6177):1530–1533. doi: 10.1136/bmj.1.6177.1530. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Westbrook K. C., Gallager H. S. Breast carcinoma presenting as an axillary mass. Am J Surg. 1971 Nov;122(5):607–611. doi: 10.1016/0002-9610(71)90287-x. [DOI] [PubMed] [Google Scholar]