

Abstract
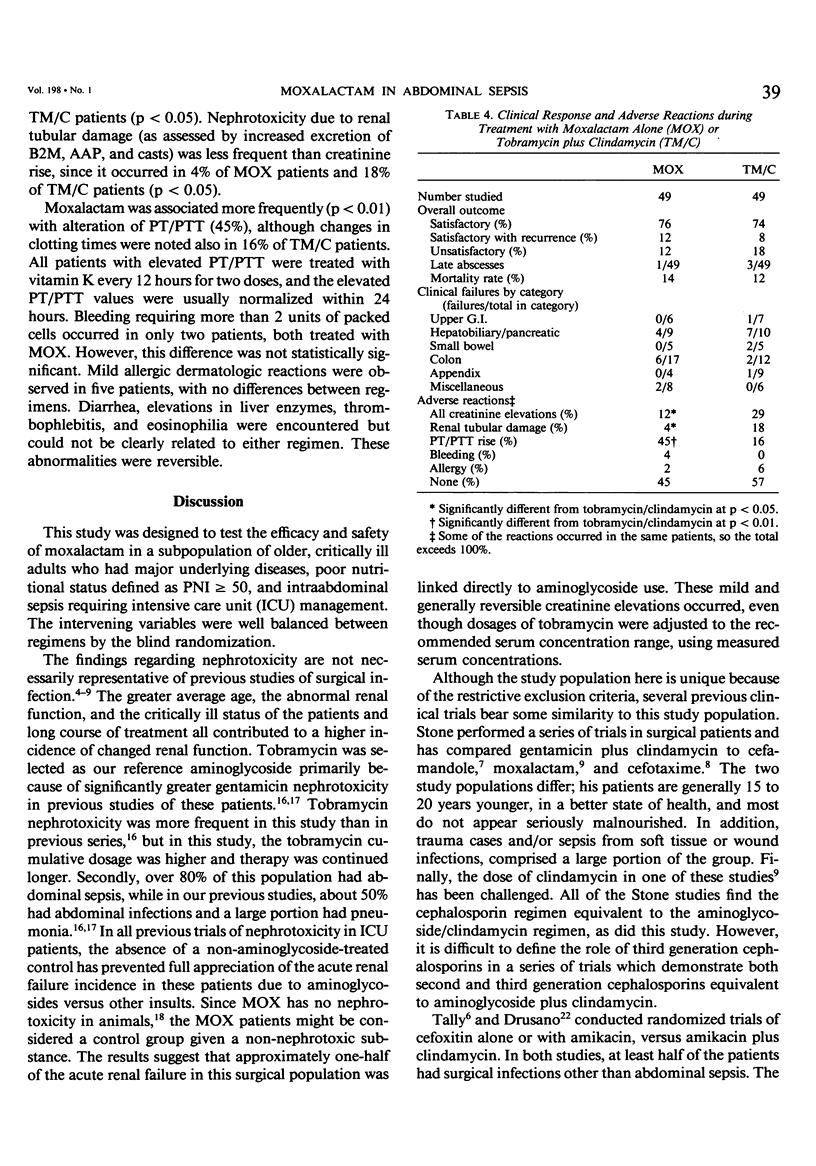
One hundred patients with intraabdominal infections were assigned randomly in double-blind fashion to receive either the combination of tobramycin plus clindamycin (TM/C) or moxalactam (MOX) alone. Fifty patients comprised each group, but one patient in each group died of infection before 48 hours treatment. In the remaining 98 patients, the average age was 62 years, initial serum albumin was 3.0 mg/dl, serum creatinine was 1.5 mg/dl, and over half of the patients were nutritionally deficient by the prognostic nutritional index criteria. In approximately one-half of the patients, the source of infection was perforated colon or perforated appendix. There were no significant differences in demographic factors between these groups, except that those who were given TM/C were older, while those who were given MOX had a more serious long-term prognosis due to underlying disease. The average length of treatment was 11 days, and the average hospitalization time was 24 days. Clinical response to therapy was identical, since 74% of the TM/C patients and 76% of the MOX patients had satisfactory responses. Bacteria persisted at the site of infection in 63% of the TM/C patients and in 65% of the MOX patients, with the most common isolate being Staphylococcus epidermidis. Pseudomonas infections were the most difficult to cure in both groups. The two regimens differed only in side effects; TM/C was a more frequent (p less than 0.05) cause of nephrotoxicity, and elevated prothrombin time/partial thromboplastin time (PT/PTT) was more frequently (p less than 0.05) observed in MOX. All PT/PTT elevations responded to injections of vitamin K, and no serious bleeding occurred. Choice between these regimens depends on the risk of renal versus hematologic side effects, rather than efficacy.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Buzby G. P., Mullen J. L., Matthews D. C., Hobbs C. L., Rosato E. F. Prognostic nutritional index in gastrointestinal surgery. Am J Surg. 1980 Jan;139(1):160–167. doi: 10.1016/0002-9610(80)90246-9. [DOI] [PubMed] [Google Scholar]
- Christensen G. D., Bisno A. L., Parisi J. T., McLaughlin B., Hester M. G., Luther R. W. Nosocomial septicemia due to multiply antibiotic-resistant Staphylococcus epidermidis. Ann Intern Med. 1982 Jan;96(1):1–10. doi: 10.7326/0003-4819-96-1-1. [DOI] [PubMed] [Google Scholar]
- Dionigi P., Nazari S., Bonoldi A. P., Cividini F., Olezza S., Dionigi R. Nutritional assessment and surgical infections in patients with gastric cancer or peptic ulcer. JPEN J Parenter Enteral Nutr. 1982 Mar-Apr;6(2):128–133. doi: 10.1177/0148607182006002128. [DOI] [PubMed] [Google Scholar]
- Harding G. K., Buckwold F. J., Ronald A. R., Marrie T. J., Brunton S., Koss J. C., Gurwith M. J., Albritton W. L. Prospective, randomized comparative study of clindamycin, chloramphenicol, and ticarcillin, each in combination with gentamicin, in therapy for intraabdominal and female genital tract sepsis. J Infect Dis. 1980 Sep;142(3):384–393. doi: 10.1093/infdis/142.3.384. [DOI] [PubMed] [Google Scholar]
- Lennard E. S., Dellinger E. P., Wertz M. J., Minshew B. H. Implications of leukocytosis and fever at conclusion of antibiotic therapy for intra-abdominal sepsis. Ann Surg. 1982 Jan;195(1):19–24. doi: 10.1097/00000658-198201001-00003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Luft F. C., Aronoff G. R., Evan A. P., Connors B. A., Blase D. K., Gattone V. H. Effects of moxalactam and cefotaxime on rabbit renal tissue. Antimicrob Agents Chemother. 1982 May;21(5):830–835. doi: 10.1128/aac.21.5.830. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mondorf A. W., Breier J., Hendus J., Scherberich J. E., Mackenrodt G., Shah P. M., Stille W., Schoeppe W. Effect of aminoglycosides on proximal tubular membranes of the human kidney. Eur J Clin Pharmacol. 1978 May 17;13(2):133–142. doi: 10.1007/BF00609758. [DOI] [PubMed] [Google Scholar]
- Schentag J. J., Cerra F. B., Plaut M. E. Clinical and pharmacokinetic characteristics of aminoglycoside nephrotoxicity in 201 critically ill patients. Antimicrob Agents Chemother. 1982 May;21(5):721–726. doi: 10.1128/aac.21.5.721. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schentag J. J., Plaut M. E., Cerra F. B. Comparative nephrotoxicity of gentamicin and tobramycin: pharmacokinetic and clinical studies in 201 patients. Antimicrob Agents Chemother. 1981 May;19(5):859–866. doi: 10.1128/aac.19.5.859. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schentag J. J., Plaut M. E. Patterns of urinary beta 2-microglobulin excretion by patients treated with aminoglycosides. Kidney Int. 1980 May;17(5):654–661. doi: 10.1038/ki.1980.77. [DOI] [PubMed] [Google Scholar]
- Smith J. A., Skidmore A. G., Forward A. D., Clarke A. M., Sutherland E. Prospective, randomized, double-blind comparison of metronidazole and tobramycin with clindamycin and tobramycin in the treatment of intra-abdominal sepsis. Ann Surg. 1980 Aug;192(2):213–220. doi: 10.1097/00000658-198008000-00015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stone H. H., Geheber C. E., Kolb L. D., Dunlop W. E. Clinical comparison of cefotaxime versus the combination of gentamicin plus clindamycin in the treatment of peritonitis and similar polymicrobial soft-tissue surgical sepsis. Clin Ther. 1981;4 (Suppl A):67–80. [PubMed] [Google Scholar]
- Stone H. H., Kolb L. D., Geheber C. E., Dawkins E. J. Use of aminoglycosides in surgical infections. Ann Surg. 1976 Jun;183(6):660–666. doi: 10.1097/00000658-197606000-00007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tally F. P., McGowan K., Kellum J. M., Gorbach S. L., O'Donnell T. F. A randomized comparison of cefoxitin with or without amikacin and clindamycin plus amikacin in surgical sepsis. Ann Surg. 1981 Mar;193(3):318–323. doi: 10.1097/00000658-198103000-00011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Weinstein W. M., Onderdonk A. B., Bartlett J. G., Louie T. J., Gorbach S. L. Antimicrobial therapy of experimental intraabdominal sepsis. J Infect Dis. 1975 Sep;132(3):282–286. doi: 10.1093/infdis/132.3.282. [DOI] [PubMed] [Google Scholar]
- Yu V. L. Enterococcal superinfection and colonization after therapy with moxalactam, a new broad-spectrum antibiotic. Ann Intern Med. 1981 Jun;94(6):784–785. doi: 10.7326/0003-4819-94-6-784. [DOI] [PubMed] [Google Scholar]
- Ziemniak J. A., Chiarmonte D. A., Miner D. J., Schentag J. J. HPLC determination of D and L moxalactam in human serum and urine. J Pharm Sci. 1982 Apr;71(4):399–402. doi: 10.1002/jps.2600710406. [DOI] [PubMed] [Google Scholar]