

Abstract
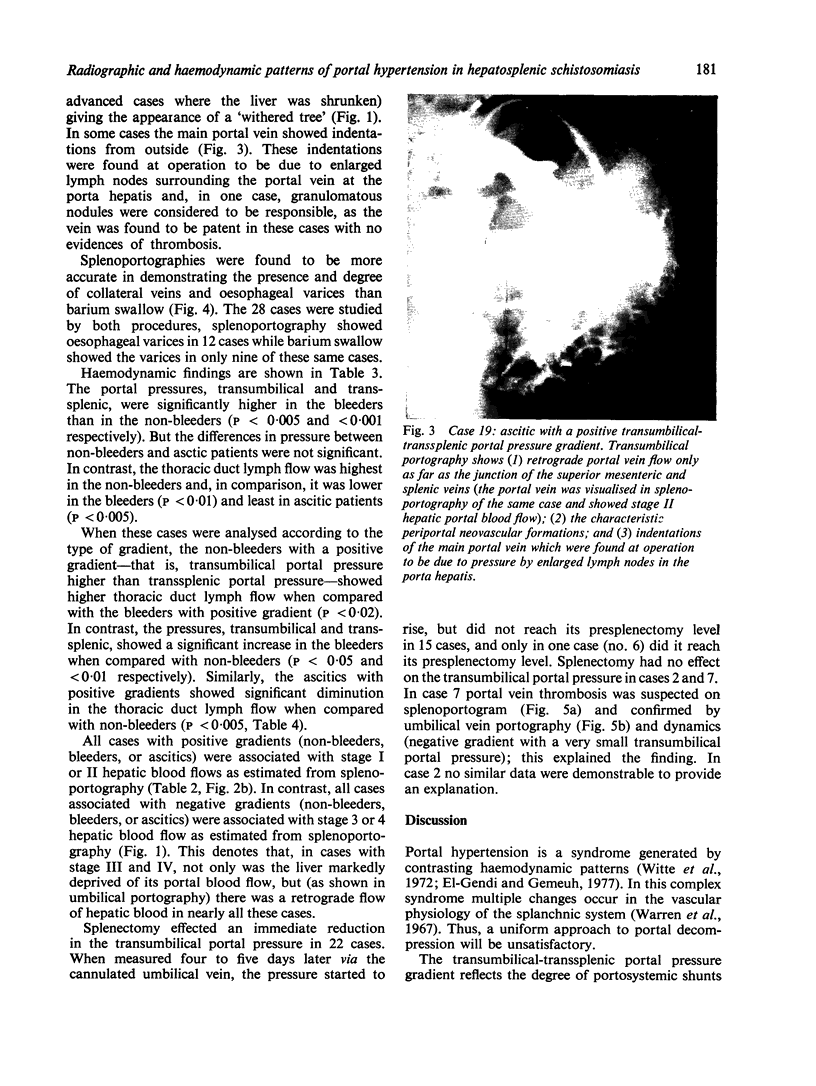
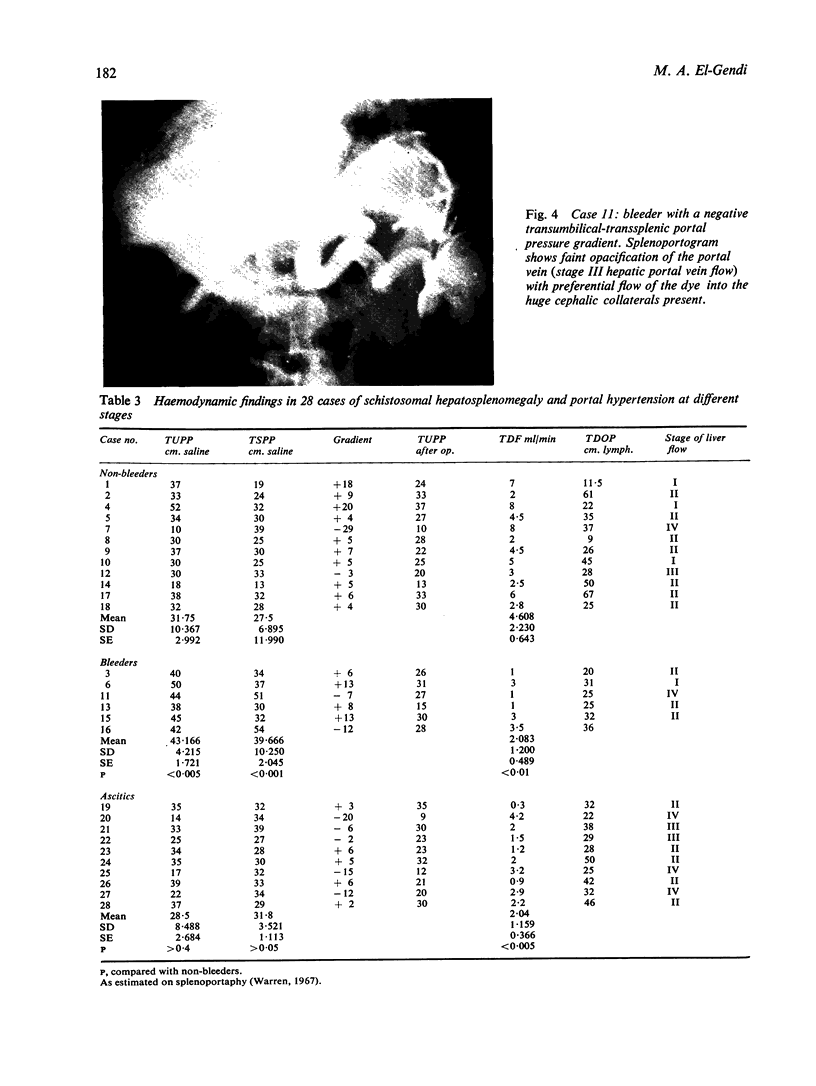
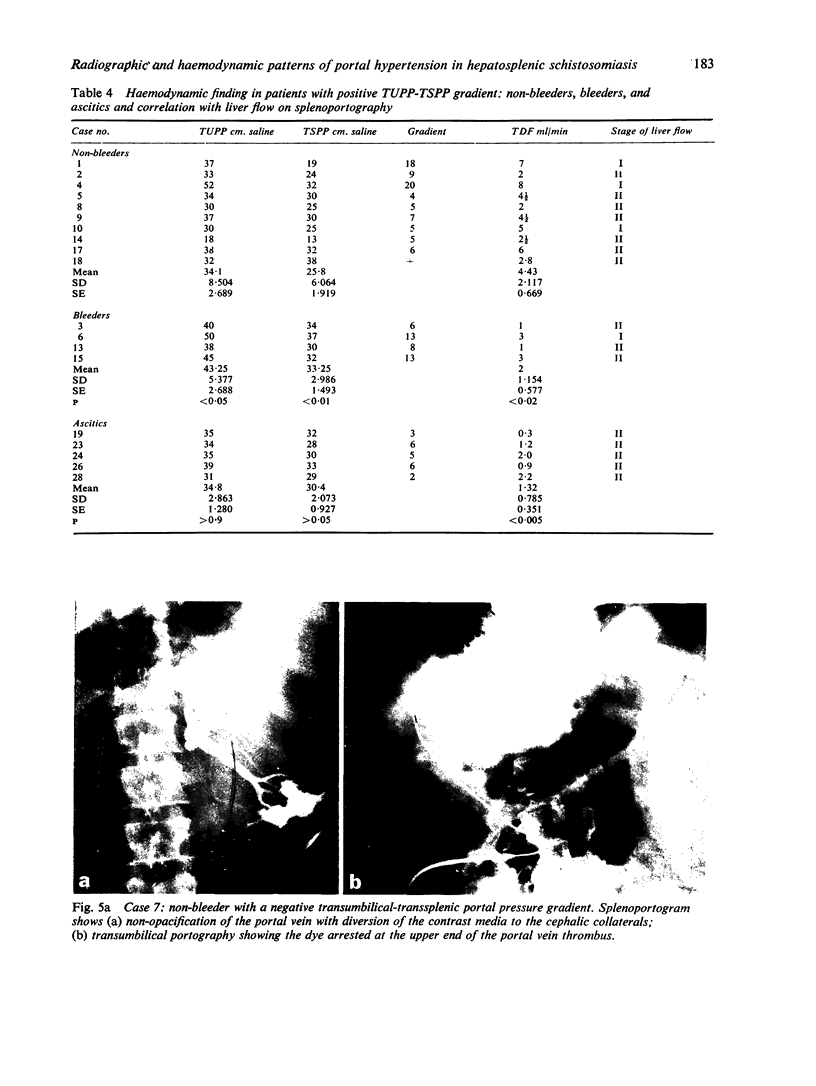
Twenty-eight patients with hepatosplenic schistosomiasis and portal hypertension were studied. The transumbilical portal pressure, transsplenic portal pressure, and thoracic duct occluded pressure were measured simultaneously and thoracic duct lymph flow estimated. Changes in the splanchnic vasculature were studied radiologically barium swallow, splenoportography, and umbilical portography. The transumbilical-transsplenic portal pressure gradient was found to be of particular value. The gradient was considered to be positive when the transumbilical portal pressure was higher than the transsplenic portal pressure, in such cases the primary generating factor of portal hypertension and/or ascites was most probably of hepatic origin. The gradient was considered to be negative when the transumbilical portal pressure was lower than the transsplenic portal pressure; in such cases the primary generating factor of portal hypertension and/or ascites was most probably of splenic or prehepatic origin. A correlation was found between the type of gradient and the radiographic pattern met with. For instance, in cases with positive gradient the hepatic blood flows, as estimated from the splenoportography, were mostly stage I or II, and showed no retrograde portal vein flow on umbilical portography. While, in cases with negative gradients, the hepatic blood flows were mostly stage III or IV, and showed retrograde portal vein flow on umbilical portography. The type of gradient, the clinicopathological stage, and the radiographic changes in the splanchnic vasculature were taken into account in selecting the surgical procedure to be used in each individual case.
Full text
PDF
Images in this article


Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- BRADLEY S. E., INGELFINGER F. J., BRADLEY G. P. Hepatic circulation in cirrhosis of the liver. Circulation. 1952 Mar;5(3):419–429. doi: 10.1161/01.cir.5.3.419. [DOI] [PubMed] [Google Scholar]
- El-Gendi M. A., Gemeuh N. Contrasting haemodynamic patterns of portal hypertension in hepatosplenic schistosomiasis. Lymphology. 1977 Dec;10(4):209–215. [PubMed] [Google Scholar]
- Gitlin N., Grahame G. R., Kreel L., Williams H. S., Sherlock S. Splenic blood flow and resistance in patients with cirrhosis before and after portacaval anastomoses. Gastroenterology. 1970 Aug;59(2):208–213. [PubMed] [Google Scholar]
- KELTY R. H., BAGGENSTOSS A. H., BUTT H. R. The relation of the regenerated liver nodule to the vascular bed in cirrhosis. Gastroenterology. 1950 Jun;15(2):285–295. [PubMed] [Google Scholar]
- PETERS R. M., WOMACK N. A. Surgery of vascular distortions in cirrhosis of the liver. Ann Surg. 1961 Sep;154:432–445. doi: 10.1097/00000658-196109000-00013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Warren W. D., Fomon J. J., Viamonte M., Zeppa R. Preoperative assessment of portal hypertension. Ann Surg. 1967 Jun;165(6):999–1012. doi: 10.1097/00000658-196706000-00015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Witte C. L., Witte M. H., Krone C. L. Contrasting hemodynamic patterns of portal hypertension. Ann Surg. 1972 Jul;176(1):68–79. doi: 10.1097/00000658-197207000-00014. [DOI] [PMC free article] [PubMed] [Google Scholar]