

Abstract
Peru's expanding population and rapid urbanization—a result of migration to its largest cities—have stressed the country's public services infrastructure and the provision of public health and environmental health services. In response, the Ministry of Health established the General Directorate of Environmental Health (DIGESA), the branch charged with assuring adequate environmental health services to populations in rural and urban areas. The magnitude of the environmental health problems in peri-urban settlements, however, has exceeded the capacity of DIGESA to respond. The Urban Environmental Health Project is an effort to develop the ability of local communities to address these problems
THE URBAN ENVIRONMENTAL Health Project (in Spanish, Salud Ambiental Urbana), operated by the Cooperative for Assistance and Relief Everywhere (CARE) Peru through the CARE–Centers for Disease Control and Prevention (CDC) Health Initiative (CCHI), initiated its activities in November 1999. The project's aim is to strengthen the capacity of municipalities and local public and private organizations to work with DIGESA to resolve environmental health problems.
Project objectives include the following:
• To create sustainable inter-institutional Committees for the Improvement of Environmental Health (CIMSAs), with representatives from local public, private, and governmental organizations.
• To develop each CIMSA's capacity to diagnose local environmental health problems.
• To inform authorities and leaders of existing and potential environmental health problems.
• To engage CIMSAs, public decision makers, and community members in the development of environmental health interventions.
TWO INTERVENTIONS
After the preliminary evaluation, the project team defined 2 areas of intervention. The first area, San Juan de Lurigancho, is the largest and most populated district in Lima; it is a peri-urban area with an arid climate. Approximately 50% of the 731 739 inhabitants of this settlement live on the steep hillsides common to the region; many homes are inaccessible by road and therefore to the trucks that distribute water. In addition, the steep slopes and rocky soil make it difficult to construct adequate latrines. The second area of intervention was the settlement Manuel Cardozo Davila in the city of Iquitos in the Amazonian jungle; this settlement is located in a zone with one of the highest growth rates in the country. In Cardozo, unlike in San Juan de Lurigancho, water is abundant; however, wells may be affected by unsanitary disposal of sewage and solid waste.
Project collaborators used the Protocol for Assessing Community Excellence in Environmental Health (PACE-EH) to conduct community-based environmental health assessments in the 2 project sites. CARE Peru, through CCHI, directed this first implementation of PACE-EH outside the United States. This instrument is designed to assist environmental health staff in conducting a community-based environmental health assessment and in creating an accurate profile of a community's environmental health status. The PACE-EH process consists of 13 tasks that help to
• Characterize and evaluate local environmental health conditions and concerns;
• Identify populations at risk of exposure to environmental hazards;
• Identify and collect meaningful environmental health data; and
• Establish priorities for local action to address environmental health problems.
The first phase of the project identified and engaged participants to set priorities and resolve community environmental health problems. This process involved participation by local government representatives, local health and education authorities, community-based social organizations, nongovernmental organizations (NGOs) operating in the project areas, and representative private enterprises. These organizations formed CIMSAs in the 2 project sites. The primary purpose of a CIMSA is to provide community members with an opportunity to be heard and participate in the community decision-making process.
In this first phase, the project team conducted a diagnostic study of environmental health conditions. A launch workshop at the project sites formally initiated the activities of the CIMSAs and enabled the project team to obtain a participatory, in-depth diagnosis of the environmental health situation. The diagnosis involved an epidemiologic and demographic profile of the project site, key-informant interviews, focus group discussions, and a review of past studies in the region. On the basis of the project site diagnosis, community participants identified and prioritized environmental health problems.
After identifying water as a priority, the assessment team used the environmental health systems method to create a water supply profile for each community. This method describes the water system from source to user and identifies needed improvements. More specifically, the process focuses on 5 attributes that are common to all water systems: quality, quantity, cost, coverage, and continuity. The water system assessments describe the condition of the water system, the factors that contribute to these conditions, and their possible antecedents. The findings of these assessments are summarized in the accompanying case studies, which describe the outcomes of the successful application of this process in these 2 diverse communities.
San Juan De Lurigancho
The Peru Ministry of Health reports that in 1999, there were 350 cases of diarrhea (loose, watery stools occurring more than 3 times in 24 hours) per 1000 children younger than 5 years in the district of San Juan de Luri-gancho. The World Health Organization (WHO) suggests that morbidity levels associated with diarrhea can be reduced by 50% with improvements in microbiological water quality.
CARE Peru's Urban Environmental Health Project conducted an assessment of the water delivery system, including microbiological analysis of 77 randomly selected water samples and completion of 58 sanitary surveys. The sanitary survey instruments assessed behaviors and storage practices that could contaminate drinking water. Instruments were used to collect information on water filling stations, water delivery trucks, and household water storage containers. A fourth instrument was used to gather information on the quantity of water used by families in their homes.
Local environmental health technicians familiar with the community, CARE Peru staff, and CDC consultants developed the survey instruments. The forms were designed for ease of use, adaptability, and simplicity of analysis. The instruments collected quantifiable data considered useful in facilitating preventive or corrective actions at the local level.
Results
• Laboratory analysis revealed microbiological contamination at every point in the chain of the water supply system: 2 of the 6 water filling stations (33%) and 2 of the 9 sampled water delivery trucks (22%) tested positive for coliform bacteria. Nine of the 43 water samples collected from drinking water receptacles (21%) tested positive for Escherichia coli.
• The average daily water use per capita is 15 L. This is on the low end of the 20 to 40 L recommended by WHO.
• Households stated that their water service was intermittent. In the 2-week period before the survey, 306 of 352 households (87%) stated that they had no water when it was needed; at the time of the survey, 38 of 356 households (11%) reported that they were without water.
• Households that are most marginalized and incapable of paying high water costs are paying 10% of their monthly income (the average monthly income is US $155.00) for poor-quality services.
• Sanitary surveys indicate that deficiencies exist in the assessed water supply system: 2 of 6 water filling stations (33%) have insufficient free chlorine residuals, 8 of 9 water delivery trucks (89%) do not protect water transfer hoses while not in use, 12 of 19 outdoor household water containers (63%) were not fitted with a protective cover, and 40 of 43 households (93%) draw drinking water by submerging receptacles into water containers.
Manuel Cardozo Davila
The city of Iquitos—at the confluence of the Itaya, Nanay, and Amazon rivers in the Amazonian forest—is the capital of the province of the Maynas; almost 79% of the provincial population (377 304 of 477 601 people) lives there. As a result of rapid urbanization, numerous settlements have developed on the periphery of the city. One such settlement is Manuel Cardozo Davila (approximate population 4750).
Water-associated diseases reported in the Cardozo epidemiologic profile are the main environmental concern of the residents. Prevalence data for the first 4 months of 2000 report the following:
Enteric parasites—23%
Superficial skin mycosis—8%
Acute diarrheal disease—7%
Furthermore, in a recent household survey completed by CARE Peru, 42 of 93 surveyed households (45%) reported 1 or more children with diarrhea for more than 1 day during the 2-week period prior to the survey.
Cardozo is served by 11 community groundwater wells with elevated storage tanks. Residents also obtain water from 13 shallow dug wells. Given the existing water distribution system, in October 2000 the CARE Peru Urban Environmental Health Project, with technical assistance from the CDC, developed an instrument to assess human behaviors, water storage practices, and water system conditions that could adversely affect water quality. CARE and CDC staff worked closely with technicians in Cardozo to assess the water supply system. Forty-four water samples were collected and analyzed by the Directorate of Environmental Health reference laboratory.
Water system assessments were conducted to determine the microbiological quality of the source water, assess the water supply system, and identify behaviors that may lead to the contamination of drinking water.
Results
• Twelve of 13 shallow dug wells (92%) tested positive for coliforms.
• Inadequate management of human waste and the existence of many poorly developed dug wells may allow contamination of the groundwater source and community drinking water wells.
• Only 1 of the 11 community wells (9%) tested positive for coliforms. The source of contamination was a nearby abandoned well that had recently been converted to a pit latrine.
• Substantial deficiencies were found in in-home water storage practices: 12 of 17 water samples collected from household containers (71%) tested positive for coliforms.
NEXT STEPS
The community-based environmental health assessment method has proved its applicability in the Peruvian context. Owing to the success of this experience, CARE Peru plans to incorporate the community-based environmental health assessment process in new projects. Future projects will include expansion of community coalitions and building of CIMSAs in other localities. Furthermore, CARE Peru will continue to advocate for inclusion of community work groups at the national level.
KEY FINDINGS
• The PACE-EH community environmental health assessment model proved applicable in Peru's coastal and jungle regions—building consensus among diverse community groups, mobilizing residents to identify problems and expect solutions, and alerting authorities to environmental problems.
• CARE Peru's building of local environmental health coalitions was fundamental to implementation of the environmental health assessment process in two peri-urban communities.
• Including community residents throughout the assessment process aided their understanding of complex environmental health issues and enabled them to develop practical and effective interventions.
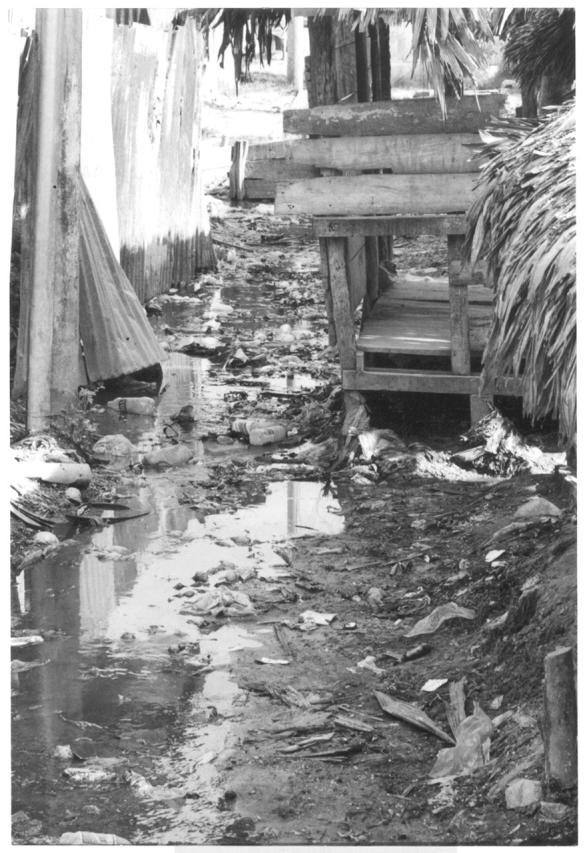
Figure 1.

Top. Many settlements in the district of San Juan de Lurigancho depend on water delivery trucks. Households are often inaccessible by road, however, and 22% of families rely on neighbors for access to drinking water.
Bottom. The Cardozo settlement in Iquitos lacks adequate sewage and drainage systems. The community relies on open sewage canals, as shown here next to the settlement's open market.
Acknowledgments
This project was supported by the R. W. Woodruff Foundation through the CARE–CDC Health Initiative (CCHI). CCHI is a collaborative effort between the US Centers for Disease Control and Prevention (CDC) and CARE International to improve global health. The CDC technical advisor for this project is employed by the CDC's National Center for Environmental Health. None of the authors have financial or other relationships that pose a conflict of interest with the reporting or interpretation of this report.
V. Baffigo, B. Hubbard, and J. Sarisky conceptualized and wrote the report. J. Sarisky, B. Hubbard, L. Nauca, and J. Albinagorta designed and conducted the field activities, and B. Hubbard and J. Sarisky analyzed the data. All of the authors contributed to the development of the CIMSA groups and reviewed the manuscript.
Resources
• Basis for the Analysis of the Health Situation. Lima, Peru: General Office of Epidemiology, Peru Ministry of Health; 1999.
• Measures of Household Security: Results of the Diagnosis in the Zones of Masusa, Belén, and South of Iquitos. Iquitos: CARE Peru–Loreto; April 2000.
• PACE-EH: Protocol for Assessing Community Excellence in Environmental Health: A Guidance Document for Local Health Officials. Washington, DC: National Association of County and City Health Officials and CDC National Center for Environmental Health; 2000.
• World Health Organization. Guidelines for Drinking Water Quality. 2nd ed. Geneva, Switzerland: World Health Organization; 1997.
• Additional information on the PACE-EH Community Environmental Health Assessment process is available from the National Association of County and City Health Officials at www.naccho.org. Additional information on the sanitary survey instruments is available from CARE Peru at baffigov@carepe.org.pe.
Peer Reviewed