
Fig 8.
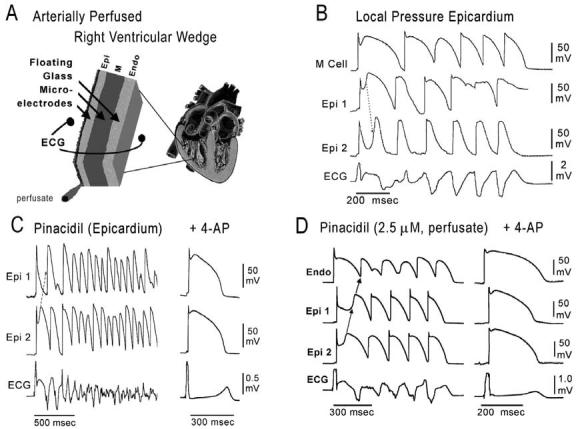
ECG and arrhythmias with typical features of the Brugada syndrome recorded from canine right ventricular wedge preparations (see inset, top left). A: Schematic of arterially perfused right ventricular wedge preparation. B: Pressure-induced phase 2 reentry and VT. Shown are transmembrane action potentials simultaneously recorded from two epicardial (Epi 1 and Epi 2) and one M region (M) site, together with a transmural ECG. Local application of pressure near Epi 2 results in loss of the action potential dome at that site but not at Epi 1 or M sites. The dome at Epi 1 then re-excites Epi 2, giving rise to a phase 2 reentrant extrasystole which triggers a short run of ventricular tachycardia. Note the ST segment elevation due to loss of the action potential dome in a segment of epicardium. C: Polymorphic VT/VF induced by local application of the potassium channel opener pinacidil (10 μM) to the epicardial surface of the wedge. Action potentials from two epicardial sites (Epi 1 and Epi 2) and a transmural ECG were simultaneously recorded. Loss of the dome at Epi 1 but not Epi 2 creates a marked dispersion of repolarization, giving rise to a phase 2 reentrant extrasystole. The extrasystolic beat then triggers a long episode of ventricular fibrillation (22 sec). Right panel: Addition of 4-AP (2 mM), a specific Ito blocker, to the perfusate restored the action potential dome at Epi 1, thus reducing dispersion of repolarization and suppressing all arrhythmic activity. BCL = 2000 msec. D: Phase 2 reentry gives rise to VT following addition of pinacidil (2.5 μM) to the coronary perfusate. Transmembrane action potentials from two epicardial sites (Epi 1 and Epi 2) and one endocardial site (Endo) as well as a transmural ECG were simultaneously recorded. Right panel: 4-AP (1 mM) markedly reduces the magnitude of the action potential notch in epicardium, thus restoring the action potential dome throughout the preparation and abolishing all arrhythmic activity. (Panel D is from ref. 72 with permission.)