

Abstract
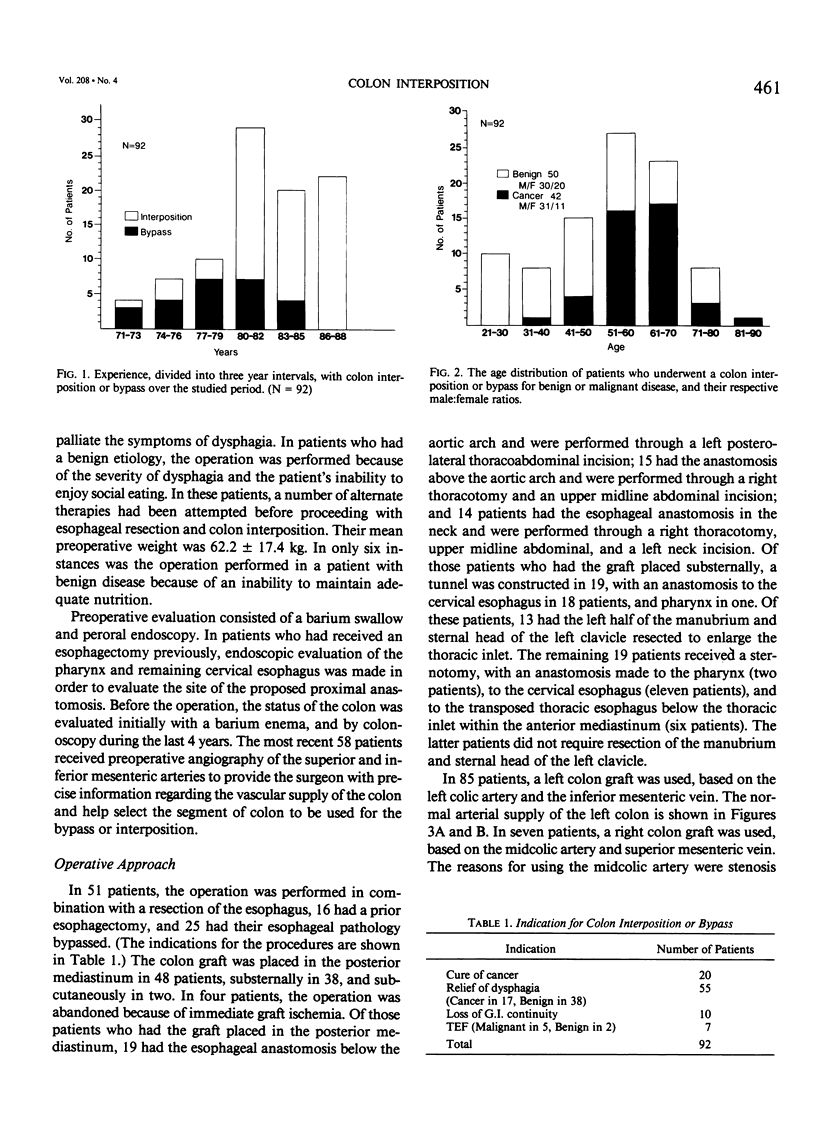
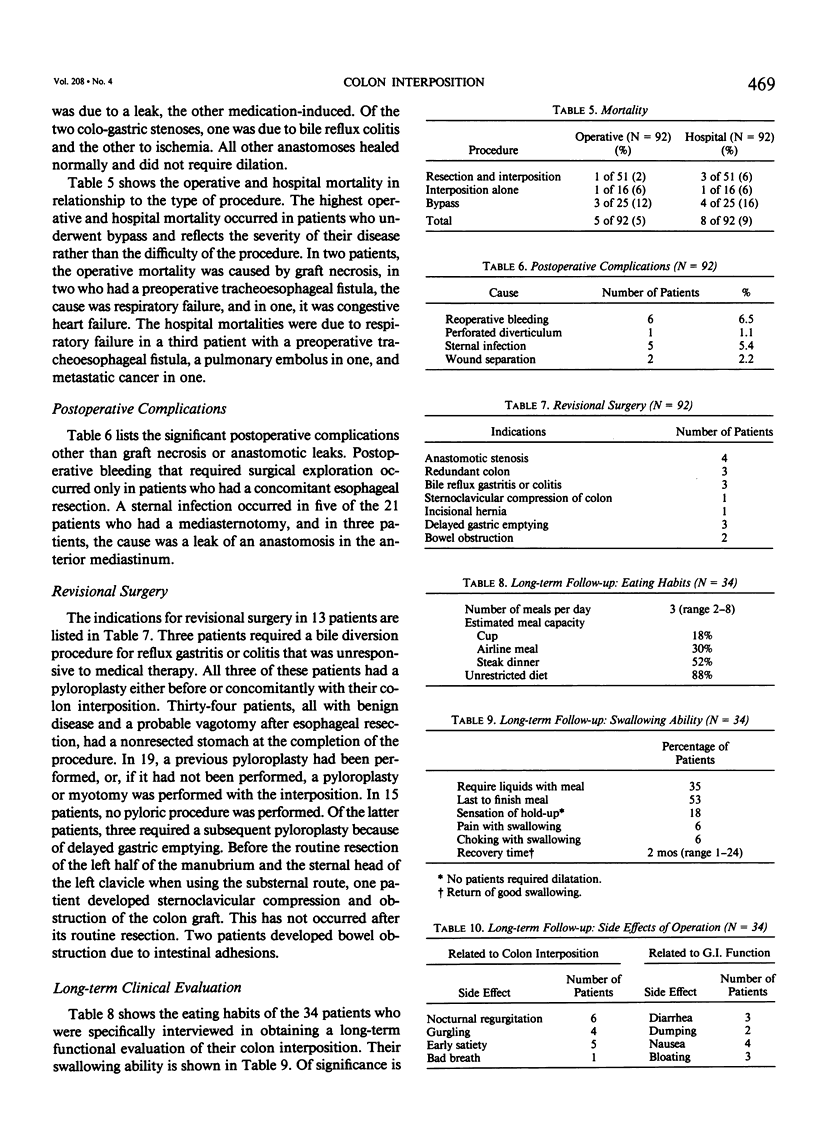
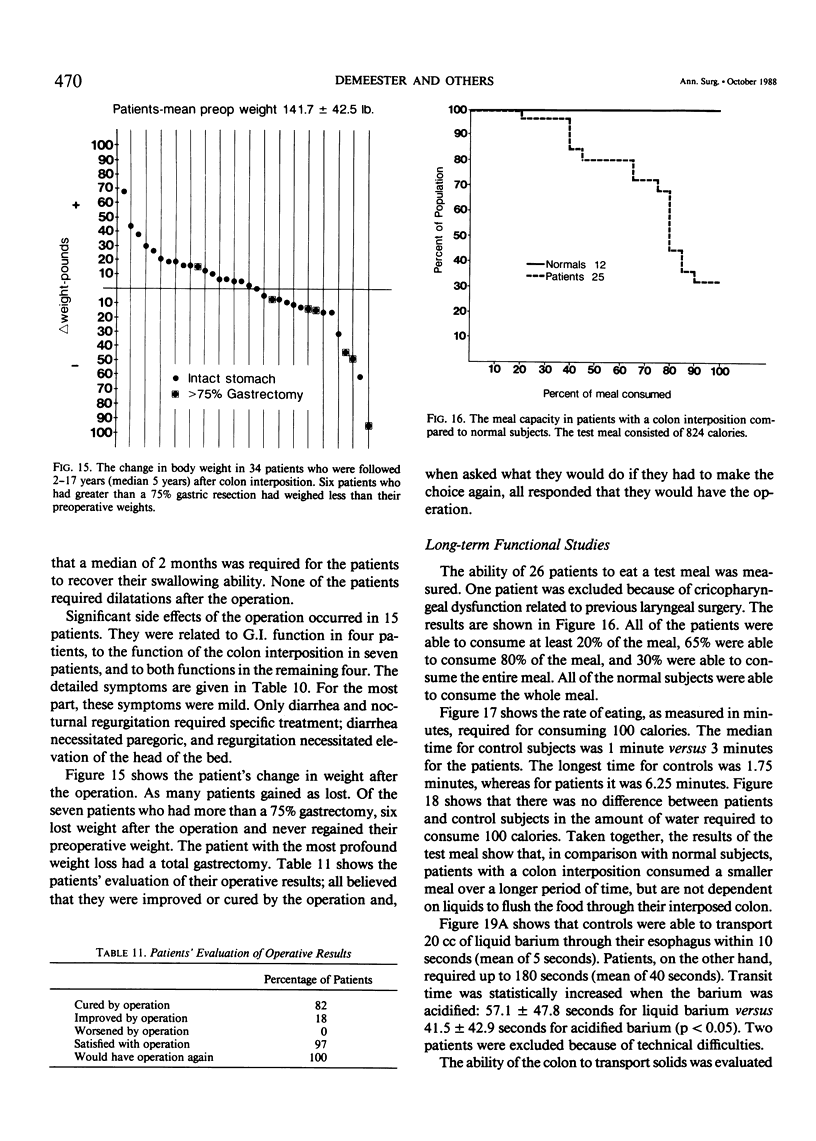
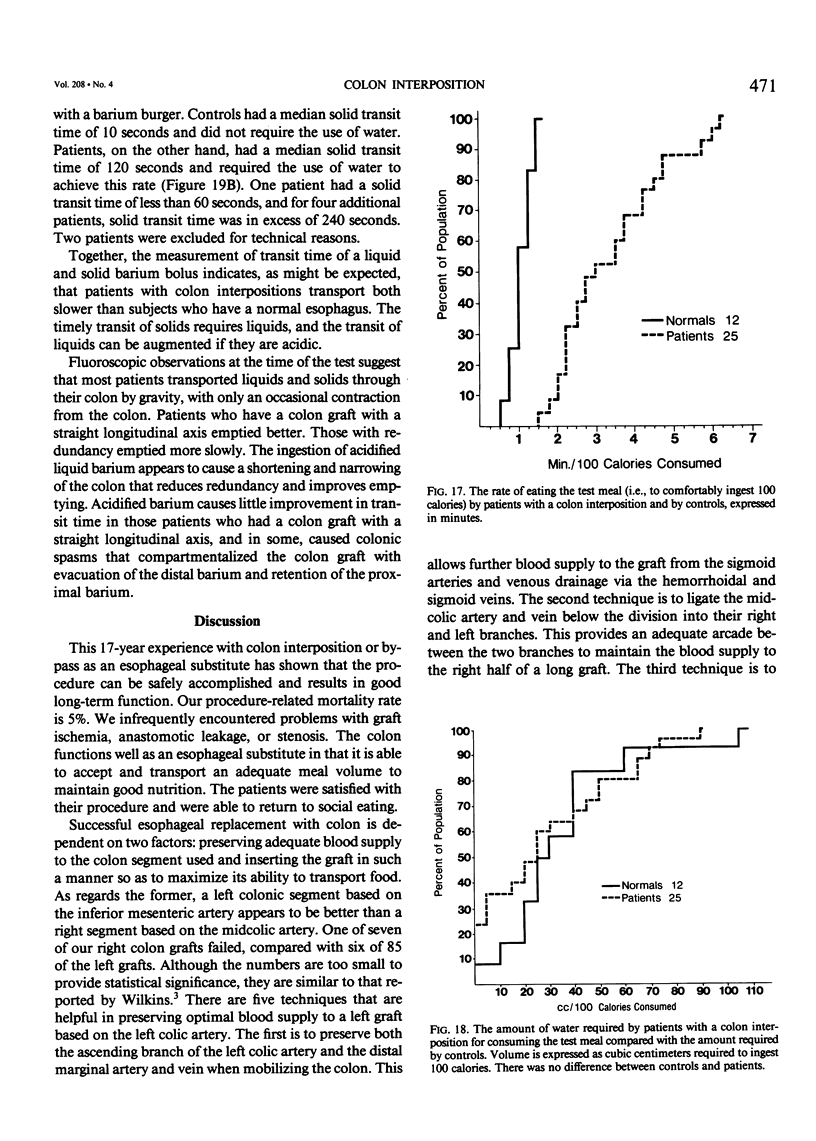
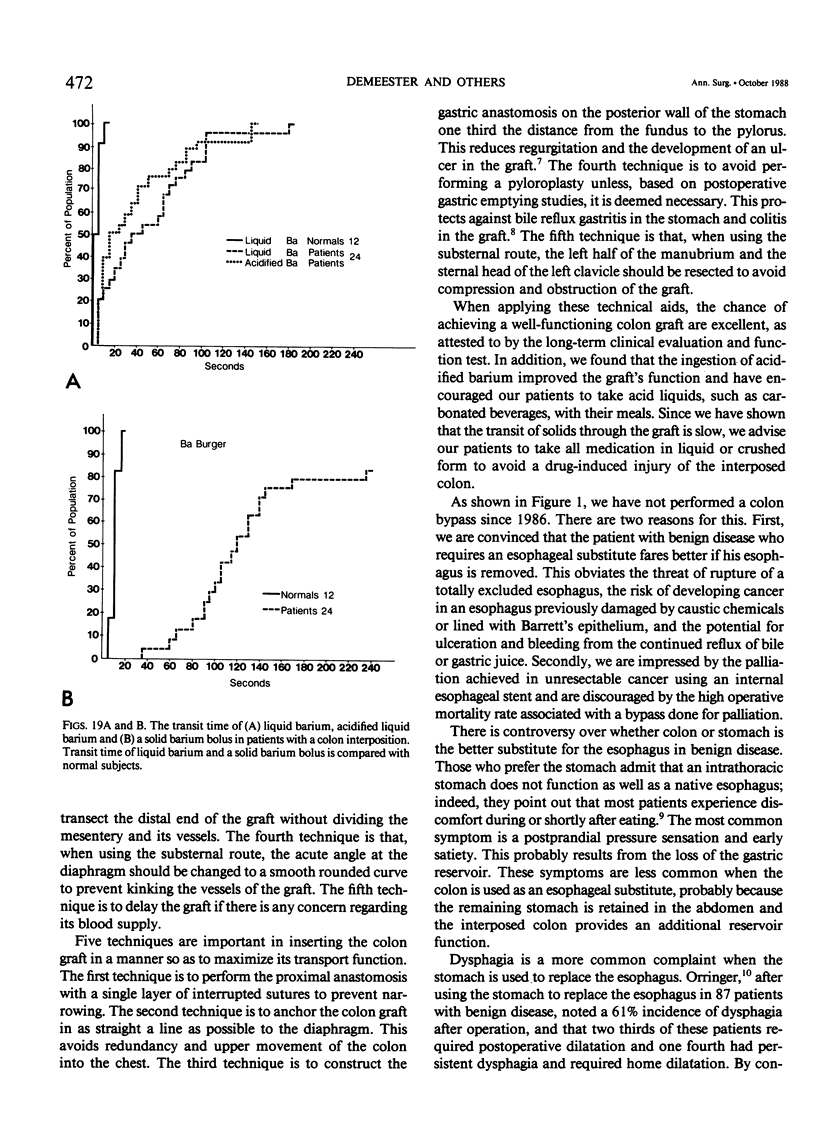
Over a 17-year period, 92 patients with esophageal disease underwent colon interposition or bypass, with each operation performed by the same surgeon. The indication was cure of cancer in 20 patients, relief of dysphagia in 55 (cancer in 17 patients and benign in 38), loss of gastrointestinal (G.I.) continuity in ten, and tracheoesophageal fistula in seven patients (malignant in five, benign in 2). The thirty-day operative mortality rate was 5%, and the hospital mortality rate was 9%. Graft necrosis occurred in seven of 92 patients, four of whom later underwent a successful second reconstruction. Thirteen patients required subsequent revisional surgery. In 85 patients, the left colon based on the inferior mesenteric artery was used, and in seven, the right colon was used. Technical insights were gained to help preserve the blood supply to the graft and improve its function in transporting food. Thirty-four patients were available for interview 2-17 years after operation (median of 5 years) 28 of whom had benign disease, and six of whom had malignant disease); 82% of the patients felt they were cured of their preoperative symptoms, 18% improved, and none worsened. Eighty-eight per cent of the patients were able to receive an unrestricted diet. All patients except one were satisfied with the results of surgery, and, asked what they would do if they had to make the choice again, all responded that they would have the operation. Twenty-six of the interviewed patients had their eating ability evaluated with a test meal and the transit time of a liquid and solid barium bolus measured. Compared to controls, patients with colon interpositions consumed a smaller capacity meal over a longer period of time and were not dependent on liquids to flush the food through the colon graft. A colon interposition provides good quality of deglutition, is very durable, and is the organ of choice for patients who require an esophageal substitute and are potential candidates for long survival.
Full text
PDF

Images in this article
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Belsey R. Reconstruction of the oesophagus. Ann R Coll Surg Engl. 1983 Nov;65(6):360–364. [PMC free article] [PubMed] [Google Scholar]
- Donner M. W., Silbiger M. L., Hookman P., Hendrix T. R. Acid-barium swallows in the radiographic evaluation of clinical esophagitis. Radiology. 1966 Aug;87(2):220–225. doi: 10.1148/87.2.220. [DOI] [PubMed] [Google Scholar]
- Hinder R. A. The effect of posture on the emptying of the intrathoracic vagotomized stomach. Br J Surg. 1976 Aug;63(8):581–584. doi: 10.1002/bjs.1800630805. [DOI] [PubMed] [Google Scholar]
- Isolauri J., Koskinen M. O., Pöyhöen L., Uusitalo A., Markkula H. Duodenogastrocolic reflux after colonic interposition measurement using scintigraphic method. Surg Gynecol Obstet. 1988 Feb;166(2):142–146. [PubMed] [Google Scholar]
- Malcolm J. A. Occurrence of peptic ulcer in colon used for esophageal replacement. J Thorac Cardiovasc Surg. 1968 Jun;55(6):763–772. [PubMed] [Google Scholar]
- Postlethwait R. W. Colonic interposition for esophageal substitution. Surg Gynecol Obstet. 1983 Mar;156(3):377–383. [PubMed] [Google Scholar]
- Wilkins E. W., Jr Long-segment colon substitution for the esophagus. Ann Surg. 1980 Dec;192(6):722–725. doi: 10.1097/00000658-198012000-00005. [DOI] [PMC free article] [PubMed] [Google Scholar]