

Abstract
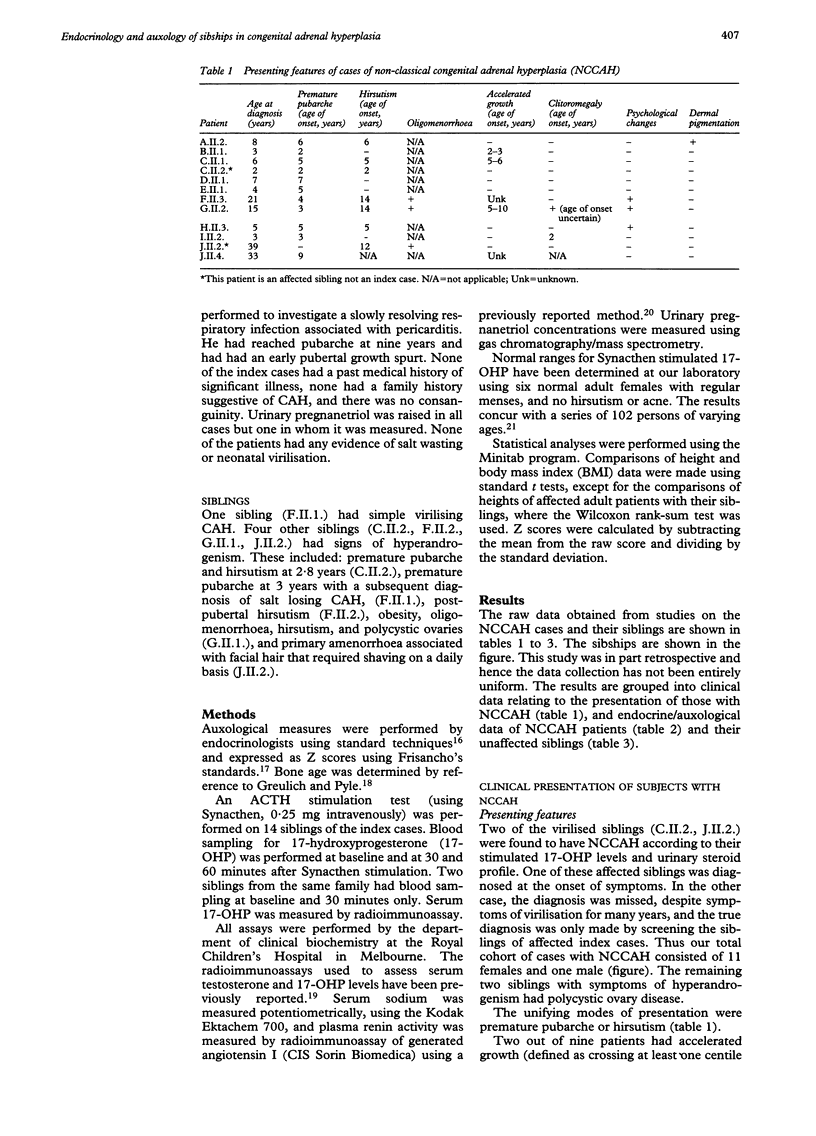
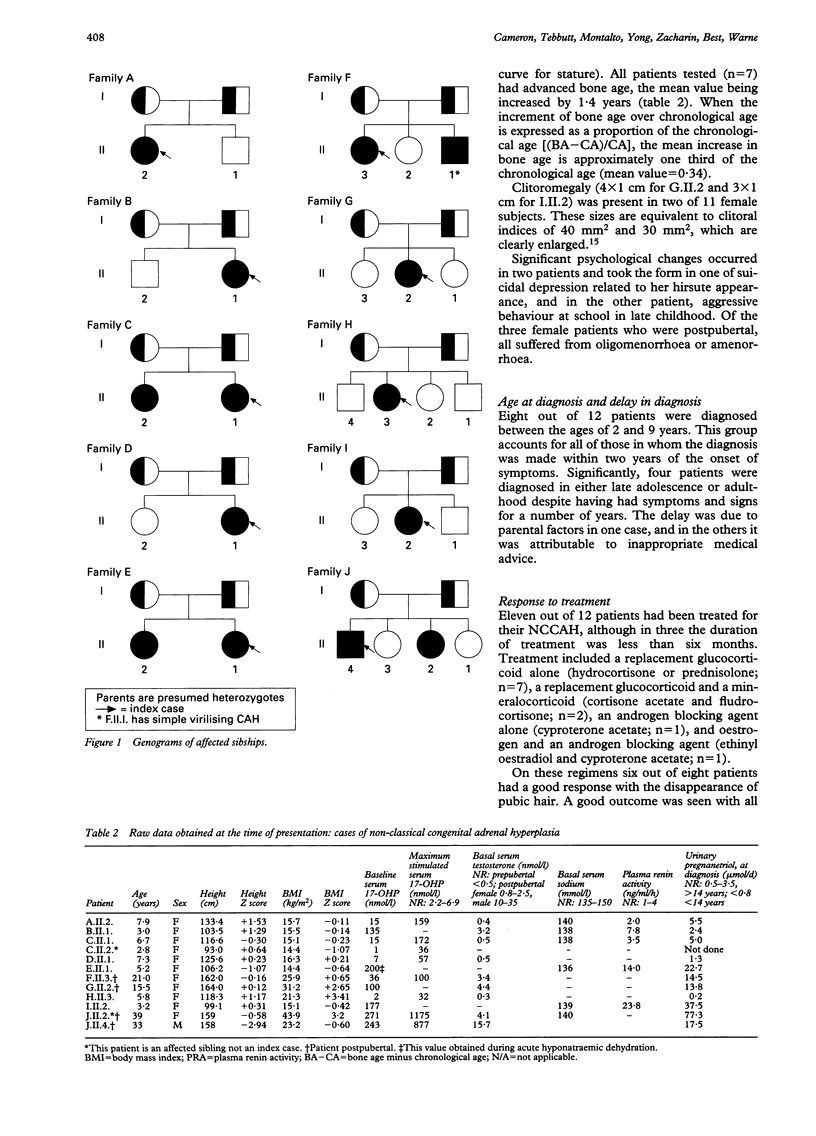
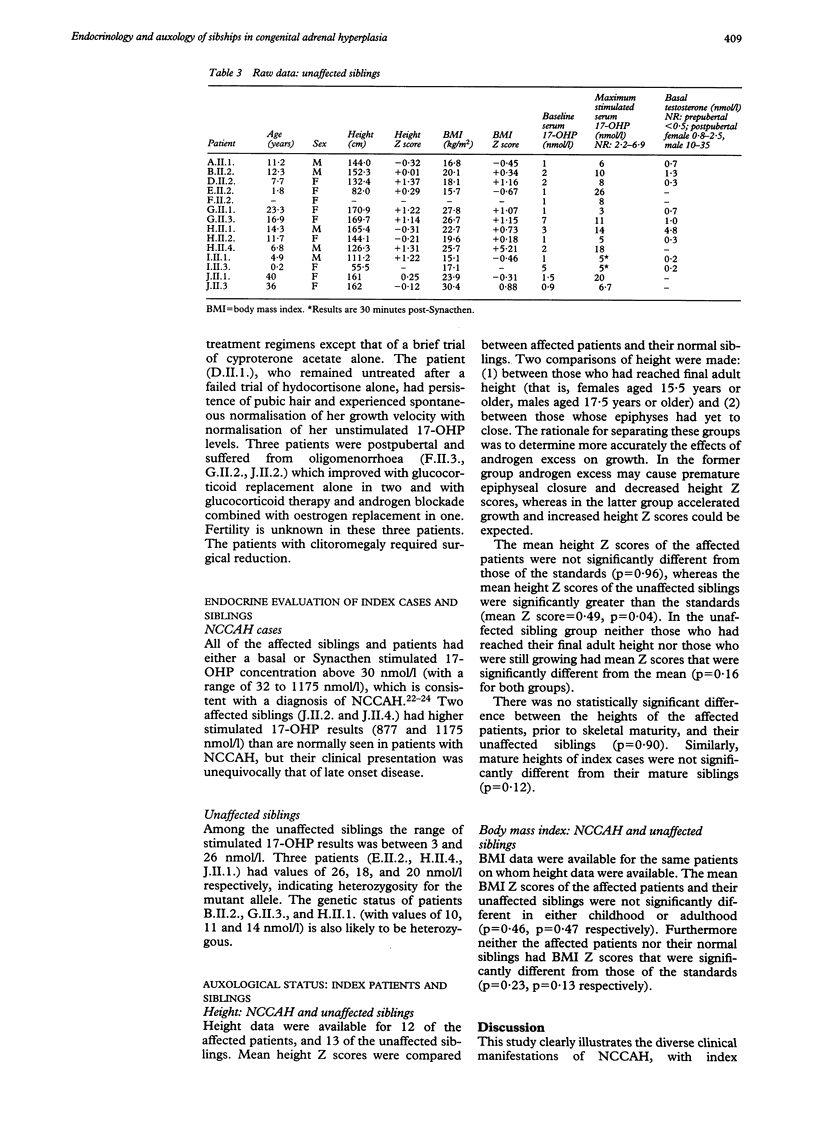
The symptoms, auxological characteristics, and stimulated 17-hydroxyprogesterone (17-OHP) concentrations in a group of patients with non-classical 21-hydroxylase deficiency (NCCAH) were compared with those of their siblings. Ten index cases consisting of nine females and one male patient aged 3-33 years and 16 siblings were studied. In the sibling group five subjects were slightly virilised and of these, two females were found to have NCCAH according to their stimulated 17-OHP concentrations. The remaining nine siblings, who were not virilised, all had normal stimulated 17-OHP concentrations. Among the total NCCAH group (index cases and affected siblings) eight patients had the diagnosis made within two years of the onset of symptoms. In four patients diagnosis was delayed until adulthood. In seven patients investigated, bone age was significantly increased before treatment. The mean height and body mass index Z scores of the affected patients as a total group or when divided according to skeletal maturity were not significantly different from either the normal mean or from their unaffected siblings. Virilised siblings of patients with NCCAH should have stimulated 17-OHP levels measured to exclude the disease. Patients with NCCAH do not appear to be at risk of short adult stature despite increased bone age in childhood.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Azziz R., Zacur H. A. 21-Hydroxylase deficiency in female hyperandrogenism: screening and diagnosis. J Clin Endocrinol Metab. 1989 Sep;69(3):577–584. doi: 10.1210/jcem-69-3-577. [DOI] [PubMed] [Google Scholar]
- Baskin H. J. Screening for late-onset congenital adrenal hyperplasia in hirsutism or amenorrhea. Arch Intern Med. 1987 May;147(5):847–848. [PubMed] [Google Scholar]
- Bormann M., Kochhan L., Knorr D., Bidlingmaier F., Olek K. Clinical heterogeneity of 21-hydroxylase deficiency of sibs with identical 21-hydroxylase genes. Acta Endocrinol (Copenh) 1992 Jan;126(1):7–9. doi: 10.1530/acta.0.1260007. [DOI] [PubMed] [Google Scholar]
- Carel J. C., Marrakchi Z., Roger M., Morel Y., Chaussain J. L. Les déficits en 21-hydroxylase à révélation tardive de l'enfant (après l'âge de trois ans). Ann Pediatr (Paris) 1993 Sep;40(7):410–420. [PubMed] [Google Scholar]
- Child D. F., Bu'lock D. E., Anderson D. C. Adrenal steroidogenesis in hirsute women. Clin Endocrinol (Oxf) 1980 Jun;12(6):595–601. doi: 10.1111/j.1365-2265.1980.tb01381.x. [DOI] [PubMed] [Google Scholar]
- Chrousos G. P., Loriaux D. L., Mann D. L., Cutler G. B., Jr Late-onset 21-hydroxylase deficiency mimicking idiopathic hirsutism or polycystic ovarian disease. Ann Intern Med. 1982 Feb;96(2):143–148. doi: 10.7326/0003-4819-96-2-143. [DOI] [PubMed] [Google Scholar]
- Dewailly D., Vantyghem-Haudiquet M. C., Sainsard C., Buvat J., Cappoen J. P., Ardaens K., Racadot A., Lefebvre J., Fossati P. Clinical and biological phenotypes in late-onset 21-hydroxylase deficiency. J Clin Endocrinol Metab. 1986 Aug;63(2):418–423. doi: 10.1210/jcem-63-2-418. [DOI] [PubMed] [Google Scholar]
- Drucker S., New M. I. Nonclassic adrenal hyperplasia due to 21-hydroxylase deficiency. Pediatr Clin North Am. 1987 Aug;34(4):1067–1081. doi: 10.1016/s0031-3955(16)36303-9. [DOI] [PubMed] [Google Scholar]
- Dumić M., Brkljacić L., Mardesić D., Plavsić V., Lukenda M., Kastelan A. 'Cryptic' form of congenital adrenal hyperplasia due to 21-hydroxylase deficiency in the Yugoslav population. Acta Endocrinol (Copenh) 1985 Jul;109(3):386–392. doi: 10.1530/acta.0.1090386. [DOI] [PubMed] [Google Scholar]
- Gordon M. T., Conway D. I., Anderson D. C., Harris R. Genetics and biochemical variability of variants of 21 hydroxylase deficiency. J Med Genet. 1985 Oct;22(5):354–360. doi: 10.1136/jmg.22.5.354. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Höller W., Scholz S., Knorr D., Bidlingmaier F., Keller E., Albert E. D. Genetic differences between the salt-wasting, simple virilizing, and nonclassical types of congenital adrenal hyperplasia. J Clin Endocrinol Metab. 1985 Apr;60(4):757–763. doi: 10.1210/jcem-60-4-757. [DOI] [PubMed] [Google Scholar]
- Knorr D., Albert E. D., Bidlingmaier F., Höller W., Scholz S. Different gene defects in the salt-wasting (SW), simple virilizing (SV), and nonclassical (NC) types of congenital adrenal hyperplasia (CAH). Ann N Y Acad Sci. 1985;458:71–75. doi: 10.1111/j.1749-6632.1985.tb14592.x. [DOI] [PubMed] [Google Scholar]
- Kohn B., Levine L. S., Pollack M. S., Pang S., Lorenzen F., Levy D., Lerner A. J., Rondanini G. F., Dupont B., New M. I. Late-onset steroid 21-hydroxylase deficiency: a variant of classical congenital adrenal hyperplasia. J Clin Endocrinol Metab. 1982 Nov;55(5):817–827. doi: 10.1210/jcem-55-5-817. [DOI] [PubMed] [Google Scholar]
- Kuhnle U., Bullinger M., Schwarz H. P., Knorr D. Partnership and sexuality in adult female patients with congenital adrenal hyperplasia. First results of a cross-sectional quality-of-life evaluation. J Steroid Biochem Mol Biol. 1993 Apr;45(1-3):123–126. doi: 10.1016/0960-0760(93)90131-f. [DOI] [PubMed] [Google Scholar]
- Kuttenn F., Couillin P., Girard F., Billaud L., Vincens M., Boucekkine C., Thalabard J. C., Maudelonde T., Spritzer P., Mowszowicz I. Late-onset adrenal hyperplasia in hirsutism. N Engl J Med. 1985 Jul 25;313(4):224–231. doi: 10.1056/NEJM198507253130404. [DOI] [PubMed] [Google Scholar]
- Lashansky G., Saenger P., Fishman K., Gautier T., Mayes D., Berg G., Di Martino-Nardi J., Reiter E. Normative data for adrenal steroidogenesis in a healthy pediatric population: age- and sex-related changes after adrenocorticotropin stimulation. J Clin Endocrinol Metab. 1991 Sep;73(3):674–686. doi: 10.1210/jcem-73-3-674. [DOI] [PubMed] [Google Scholar]
- Miller W. L. Clinical review 54: Genetics, diagnosis, and management of 21-hydroxylase deficiency. J Clin Endocrinol Metab. 1994 Feb;78(2):241–246. doi: 10.1210/jcem.78.2.8106606. [DOI] [PubMed] [Google Scholar]
- Montalto J., Whorwood C. B., Funder J. W., Yong A. B., Callan A., Davies H. E., Connelly J. F. Plasma C19 steroid sulphate levels and indices of androgen bioavailability in female pattern androgenic alopecia. Clin Endocrinol (Oxf) 1990 Jan;32(1):1–12. doi: 10.1111/j.1365-2265.1990.tb03744.x. [DOI] [PubMed] [Google Scholar]
- New M. I., Lorenzen F., Lerner A. J., Kohn B., Oberfield S. E., Pollack M. S., Dupont B., Stoner E., Levy D. J., Pang S. Genotyping steroid 21-hydroxylase deficiency: hormonal reference data. J Clin Endocrinol Metab. 1983 Aug;57(2):320–326. doi: 10.1210/jcem-57-2-320. [DOI] [PubMed] [Google Scholar]
- New M. I. Steroid 21-hydroxylase deficiency (congenital adrenal hyperplasia). Am J Med. 1995 Jan 16;98(1A):2S–8S. doi: 10.1016/s0002-9343(99)80052-7. [DOI] [PubMed] [Google Scholar]
- Sane K., Pescovitz O. H. The clitoral index: a determination of clitoral size in normal girls and in girls with abnormal sexual development. J Pediatr. 1992 Feb;120(2 Pt 1):264–266. doi: 10.1016/s0022-3476(05)80439-1. [DOI] [PubMed] [Google Scholar]
- Speiser P. W., Dupont B., Rubinstein P., Piazza A., Kastelan A., New M. I. High frequency of nonclassical steroid 21-hydroxylase deficiency. Am J Hum Genet. 1985 Jul;37(4):650–667. [PMC free article] [PubMed] [Google Scholar]
- Tanner J. M. Normal growth and techniques of growth assessment. Clin Endocrinol Metab. 1986 Aug;15(3):411–451. doi: 10.1016/s0300-595x(86)80005-6. [DOI] [PubMed] [Google Scholar]
- Temeck J. W., Pang S. Y., Nelson C., New M. I. Genetic defects of steroidogenesis in premature pubarche. J Clin Endocrinol Metab. 1987 Mar;64(3):609–617. doi: 10.1210/jcem-64-3-609. [DOI] [PubMed] [Google Scholar]
- Wilson R. C., Mercado A. B., Cheng K. C., New M. I. Steroid 21-hydroxylase deficiency: genotype may not predict phenotype. J Clin Endocrinol Metab. 1995 Aug;80(8):2322–2329. doi: 10.1210/jcem.80.8.7629224. [DOI] [PubMed] [Google Scholar]
- Yong A. B., Montalto J., Pitt J., Oakes S., Preston T., Buchanan C. Corticosterone methyl oxidase type II (CMO II) deficiency: biochemical approach to diagnosis. Clin Biochem. 1994 Dec;27(6):491–494. doi: 10.1016/0009-9120(94)00048-z. [DOI] [PubMed] [Google Scholar]
- Young M. C., Ribeiro J., Hughes I. A. Growth and body proportions in congenital adrenal hyperplasia. Arch Dis Child. 1989 Nov;64(11):1554–1558. doi: 10.1136/adc.64.11.1554. [DOI] [PMC free article] [PubMed] [Google Scholar]
- van der Kamp H. J., Slijper F. M., Brandenburg H., de Muinck Keizer-Schrama S. M., Drop S. L., Molenaar J. C. Evaluation of young women with congenital adrenal hyperplasia: a pilot study. Horm Res. 1992;37 (Suppl 3):45–49. doi: 10.1159/000182400. [DOI] [PubMed] [Google Scholar]